 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
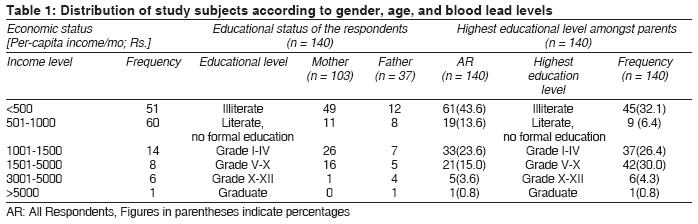
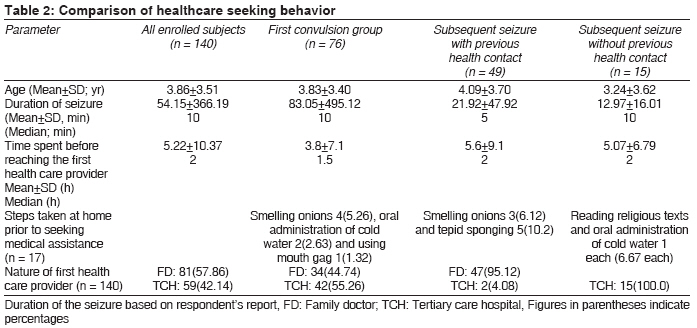
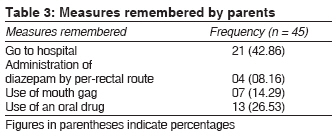
Indian Journal of Medical Sciences, Vol. 62, No. 8, August, 2008, pp. 331-335 ORIGINAL CONTRIBUTION Healthcare-seeking behavior after seizures in children Bavdekar Sandeep B, Ghule Rahul, Jadhav Sandhya Department of Pediatrics, Seth GS Medical College and KEM Hospital, Parel, Mumbai-400 012 Code Number: ms08059 Abstract Background: Hardly any Indian data is available regarding practices employed by parents for preventing injuries and aspiration and controlling convulsions in children.Aims: To describe the health care-seeking behavior and practices employed by parents when a child has convulsions. Settings and Design: Prospective questionnaire-based study in a tertiary care hospital setting. Materials and Methods: Parents of children (age: 1 month -12 years) admitted with history of convulsions were enrolled and information regarding demographic characteristics, time lag, preferred health care provider and measures taken in a convulsing child was elicited using a pretested questionnaire. Statistical Analysis Used: Demographic parameters and measures employed described as percentages. Results: One hundred and forty parents were interviewed. Seventy-six children had first episode. Forty-nine of 64 children with subsequent seizures had contact with a health care provider during the previous seizure episode. The median duration of seizures was 10 minutes (Mean: 54.15±366.39 min); but children were brought to the hospital after a median of 2 hours (Mean: 5.22±10.37 h). Measures such as smelling onions, oral administration of cold water, reading religious texts and insertion of mouth gag were employed. Although 45 with previous seizure-related health care contact agreed that they were informed about measures to be taken, none of them could remember more than one measure for preventing injuries and aspiration and controlling seizures. Only four narrated "per-rectal administration of diazepam" as a measure, although only one implemented it. Only four general practitioners used per-rectal diazepam to control seizures. Conclusions: Children with seizures reach health care providers after a considerable delay putting them at higher risk for developing neurological sequel. There is a need to develop appropriate strategies for disseminating information about "first aid" measures and steps for controlling convulsions and imparting relevant skills to parents. Keywords: Convulsions, first aid, parental education Introduction Convulsions constitute one of the commonest emergencies with which children are brought to the emergency room. They can threaten life and be associated with sequels such as focal neurological deficits, mental retardation and seizure disorder. [1] It is, therefore, essential that children with convulsions receive prompt treatment. Generally, parents do not know much about effective measures to be taken in case of convulsions [2],[3] and on seeing the child convulse spend the first precious minutes in ineffective measures. [4] There is paucity of such data in the Indian milieu. A study was undertaken to list steps parents take when a child convulses and ascertain if previous contact with a health care provider brings about any change. as this information would help devise appropriate interventions. Materials and Methods This prospective study was carried out in the Department of Pediatrics of on 1800-bedded tertiary care hospital in Mumbai after obtaining permission from the institutional ethics committee. One of the parents of every child (age: 1 month - 12 years) admitted to the Pediatric ward was enrolled in the study after obtaining written informed consent. If they agreed to participate, a pretested questionnaire was administered by a single observer (RG) within 24 hours of admission to the health facility, so as to avoid inter-observer variability and lapses in memory. The questionnaire was tested and validated in a pilot study involving parents of 15 pediatric patients with convulsions admitted to the same institution. The information regarding demographic characteristics and measures taken by caregivers were described in terms of percentages. Results One hundred and forty respondents (mother: 103, father: 37) were interviewed. As shown in [Table - 1], 61(43.6%) of respondents were illiterate and in 45 (32.1%) of households none of the parents was literate. The monthly household income ranged from Rs. 1200- Rs. 30000 with per capita income varying from Rs. 343 - Rs. 5050 [Table - 1]. The etiological factors for convulsions amongst the 140 children (83 boys and 57 girls; age 1.5 months - 12 years) enrolled in the study included febrile seizure 88, epilepsy 39, meningitis and meningoencephalitis 8, hypocalcemia 2 and tuberculosis of the central nervous system, hydrocephalus and neurocysticercosis 1 each. There were 76 subjects with the first episode of seizure. Of the 64 children admitted with subsequent convulsion, 15 had no previous contact with any health care provider for convulsions. Information regarding age, sex ratio, duration of convulsion and time taken to reach the health care provider is provided in [Table - 1]. One hundred subjects were admitted after a generalized tonic-clonic convulsion while the rest had partial tonic-clonic convulsion. Eleven (7.86%) subjects were brought to the hospital in a convulsive state, with a gap of 2.2±1.5 hours before effective therapy was received. The mean duration of seizure was 54.15±366.19 min (median 10 min) and parents spent 5.22±10.37 hours (median 2 h) before they could reach the first health care provider. Parents of 81 subjects chose their family doctor as the first health care provider while the other 59 rushed to a tertiary care centre. Measures taken by general practitioner included: advice to go to a hospital (81, 100%), administration of an oral drug (14, 17.28%) and administration of diazepam per-rectally (4, 4.94%). Eleven patients were having convulsions when they reached the general practitioner. But, only four practitioners provided effective therapy in the form of administration of anti-convulsant by per-rectal route. No patient received an anti-convulsant drug via intravenous route. [Table - 2] depicts the demographic characteristics, time lag in presenting to the doctor and list of measures taken by parents at home, which included smelling onions, oral administration of cold water, tepid sponging, reading religious texts and using a mouth gag. From amongst 49 parents who had previous contact with a doctor for previous seizure, 45 conceded that they were told about certain measures to be taken in case of a seizure. The measures that parents remembered are enumerated in [Table - 3]. No one could remember more than one measure. Although four remembered about per-rectal administration of diazepam, it was not implemented by anyone. The reasons given for this non-compliance included fear, ignorance about the way of administering it and lack of medical knowledge. Discussion Parents can play an important role in preventing injuries and aspirations associated with convulsions and can also take effective steps to control convulsions at home. The latter is of great significance since longer-duration seizures carry an increased risk of developing permanent neurological sequels. Studies have documented that prior to the first convulsion in their child, parents have hardly any knowledge about the measures to be taken in case of such an emergency. [5],[6] This is not surprising given the fact that such information is not available to the general population. Several educational interventions aimed at tackling these gaps in knowledge, reducing parental anxiety and empowering them to implement appropriate preventive and therapeutic measures in children at risk for recurrent seizures have been evaluated. Although some programs are found to be effective, [4],[7] this "effectiveness" has been judged on the basis of answering a questionnaire before and after the intervention program and not on the basis of steps actually taken, when faced with a convulsing child. It has also been found that inappropriate measures such as cardiac massage and mouth-to-mouth respiration continue to be employed even after providing information. [8] Hardly any data from India is available in this regard. [9] The study portrays a sorry state of affairs. The knowledge of parents regarding measures to be taken when their child convulses is abysmally low and their knowledge and practices do not improve even after being informed about effective measures. Their recall is highly inadequate and those who remember hardly ever use it when faced with a subsequent seizure. The reasons for this could be many and include: lapse in memory, panic reaction (making them act on impulse), lack of practicing skills or pressure from other household members to continue to employ age-old (but ineffective) measures. Above all, the findings also could point towards ineffectiveness of methodology used for providing information. There are several other facts that are a matter of concern: The patients reach the hospital after a prolonged period (Mean: 5.22 h, Median: 2 h) after the onset of a convulsion. It means that children with prolonged seizure would be left with neurological sequels, since they take hours to reach the health post. It may, however, be noted that the duration of seizure recorded was based on respondents′ response, which may not always be accurate. The study also brings into focus the role of "family physicians", who hardly ever take measures to control the convulsion, but just direct the parents to go to the nearest hospital. In the study, 11 patients were brought convulsing to the family physician. However, only one received the effective measure of per-rectal administration of diazepam. No one received any intravenous drug for control of seizures. There seems to be a need for informing family physicians about appropriate measures to be taken when faced with a convulsing child and imparting skills to handle this emergency. The study had its limitations. It is theoretically possible that several children were managed effectively at home or by family doctors and hence did not report to the hospital. This does not seem to be the case, as 129 children were brought to the hospital even after their seizure was controlled. The reasons for delay in reaching the hospital after seizure have not been ascertained. It could be a combination of factors such as time spent at home on inappropriate measures, panic leading to delay in planning actions, staying put in the hope that seizure would subside spontaneously and delays in transportation. Despite the relatively small numbers enrolled, the study has demonstrated that parents do not have adequate knowledge about measures effective in controlling seizures, that there is hardly any improvement in knowledge and practices related to controlling seizures even after a health contact and that family physicians fail to take appropriate measures for controlling seizures. It is probably essential to implement innovative strategies that include demonstration and practice of skills for parents with children at risk of developing seizures. In addition, there is a need to inform the general population regarding the "first aid" measures that would help prevent aspiration and injuries in a convulsing child. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08059t1.jpg] [ms08059t3.jpg] [ms08059t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}