 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 62, No. 9, September, 2008, pp. 345-353 ORIGINAL CONTRIBUTION A comparative study of endoscopic ultrasonography versus endoscopic retrograde cholangiopancreatography in children with chronic liver disease El-Karaksy HanaaM, El-Koofy NehalM, Okasha Hussein, Kamal NaglaaM, Naga Mazen Department of Internal Medicine, Cairo University Code Number: ms08062 Abstract Background: Endoscopic ultrasonography (EUS) is a less invasive modality and may be equal or superior to endoscopic retrograde cholangiopancreatography (ERCP) in visualizing the biliary tree. Its role and feasibility in children need to be accurately defined.Aim: This study aimed at evaluation of EUS in assessment of children with chronic liver disease (CLD) in comparison with ERCP. Materials and Methods: The present study was carried out between September 2004 and February 2006 on 40 children suffering from CLD. Patients were selected from the Pediatric Hepatology Unit, Cairo University Children's Hospital, Egypt. They were included if they had: sonographic (n = 8) or histopathological evidence of biliary pathology (n = 2); autoimmune hepatitis with high gamma glutammyl transpeptidase (GGT) levels and/or not responding to immunosuppressive therapy (n = 15); cryptogenic CLD (n = 13); neonatal cholestasis with relapsing or persistent course (n = 2). They all underwent EUS and ERCP. Results: Three of six cases with intrahepatic biliary radicle dilatation had Caroli's disease by EUS and ERCP; and the other 3 had sclerosing cholangitis. EUS was equal to ERCP in diagnosis of biliary pathology. However, one false positive case was described to have dilatation and tortuosity of the pancreatic duct by EUS as compared to ERCP. EUS could detect early pancreatitis in 5 cases. One case with cryptogenic liver disease proved to have sclerosing cholangitis by both EUS and ERCP. Conclusion: EUS is an important diagnostic tool for biliary pathology and pancreatitis in children with pancreatico-biliary pathology. ERCP should be reserved for therapeutic purposes. Keywords: Children, endoscopic ultrasonography, endoscopic retrograde cholangiopancreatography, sclerosing cholangitis Introduction Endoscopic ultrasonography (EUS) is a major advance in gastrointestinal imaging [1] and is considered a well described examination method that is used to image suspected pathology in the gastrointestinal tract and in the adjacent organs. [2] Its diagnostic accuracy in the evaluation of pancreatico-biliary diseases exceeds 90%. [3],[4] Although endoscopic retrograde cholangio-pancreatography (ERCP) is the gold standard for pancreatico-biliary evaluation, it is invasive and is associated with complication rate of 2.5 to 11%. [5] EUS was reported to be a less invasive modality for confirming a normal biliary tree and should be considered a low risk alternative to ERCP. [6] Roseau and his group [7] demonstrated the feasibility of EUS in pediatrics (at least in older children).They found it less invasive and of equal results, if not superior, when compared to other modalities previously used such as ERCP. The primary aim in this study was to evaluate the role of EUS in pancreatico-biliary assessment of children with chronic liver disease, of various etiologies, in comparison to ERCP. The secondary aim was to compare the findings obtained by EUS with those obtained by conventional abdominal ultrasound. Materials and Methods The present study is a descriptive comparative study carried out between September 2004 and February 2006 on 40 children suffering from chronic liver disease presenting to the Pediatric Hepatology Unit, Cairo University Children′s Hospital, Egypt. EUS and ERCP were done at the Endoscopy Unit of the Internal Medicine Department, Cairo University, Egypt. The study protocol was approved by the Pediatrics and Internal Medicine departments′ reviewing boards. Children were enrolled in the study after an informed written consent was obtained from the parents. Inclusion criteria
Patients with sonographic evidence of biliary pathology. Exclusion criteria:
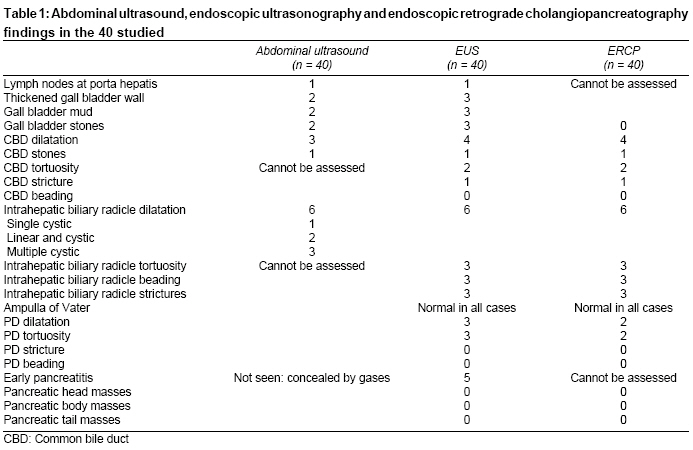
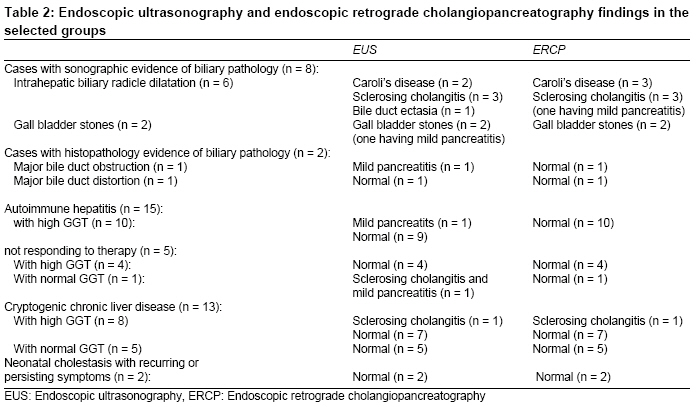
Results Forty EUS and ERCP procedures were done for the 40 selected patients with no reported complications. The findings of the 3 imaging modalities used in this study are shown in [Table - 1]. The liver size, echogenicity and vasculature, the spleen size, and the presence of ascites were well commented upon by conventional abdominal ultrasound. EUS was equal to abdominal ultrasound in commenting upon lymph nodes at the porta hepatic area, but was superior in detecting gall bladder wall thickness, gall bladder mud and stones. Common bile duct (CBD) dilatation was seen equally by EUS and ERCP and each was superior to abdominal ultrasound. Both EUS and ERCP could comment equally on the presence of stricture and tortuosity of CBD, and beading if present. However, CBD stones were seen equally by all 3 modalities. Intrahepatic biliary radicle dilatation was seen in 6 cases by all 3 modalities. Ultrasound could describe the dilatation as single cystic (n = 1), linear and cystic (n = 2) and multiple cystic lesions (n = 3). Intrahepatic biliary radicle dilatation was described in 3 out of 6 as showing strictures, beading and tortuosity by both EUS and ERCP. EUS could detect early pancreatitis in 5 cases (Cambridge classification), [8] which could not be commented upon by ERCP. Dilatation and tortuosity of the pancreatic duct (PD) was diagnosed in one case by EUS but was normal by ERCP. This was considered a false positive result as ERCP is the gold standard test in demonstrating PD abnormalities. According to our selection criteria, among the 8 cases selected for sonographic evidence of biliary pathology, 3 of the 6 with intrahepatic biliary radicle dilatation proved to have Caroli′s disease and the other 3 had sclerosing cholangitis by ERCP. EUS showed the same finding except in one case of Caroli′s disease where the description of the lesion was "bile duct ectasia" [Table - 2]. EUS and ERCP findings were normal in the 2 cases with histopathological findings suggestive of major bile duct obstruction or distortion and in the other 2 cases with neonatal cholestasis of persistent or recurrent course. Among the 15 cases with autoimmune hepatitis undergoing EUS and ERCP, 10 were responsive to therapy but had elevated GGT levels. Only two showed evidence of mild pancreatitis by EUS. One case was diagnosed by both ERCP and EUS as having sclerosing cholangitis among the 13 cases with cryptogenic chronic liver disease. This case had an elevated level of GGT. The remaining 12 cryptogenic cases had normal EUS and ERCP findings [Table - 2]. Discussion In this study we found that EUS can be successfully performed in children when using adult echo-endoscopes. Technical features of the echo-endoscope, such as size and length of the distal rigid tip, were not limiting features in this study. However, all procedures were done in children over 4years of age. In other studies, EUS was performed in children as young as 4years old. [9],[10] In this study the ultrasound findings agreed with EUS in most aspects but with superiority of EUS regarding the assessment of CBD stones, dilatation, gall bladder wall thickness, biliary mud and stones, and pancreatic ductal and parenchymal lesions. Actually, dilated bile ducts and the level of obstruction can be reliably demonstrated with US, but the cause can be determined in only a minority of patients. EUS is superior in detecting the cause of CBD dilatation in patients in whom ultrasound could not demonstrate the cause of dilation or in whom ultrasound revealed equivocal results. The sensitivity of EUS in detecting CBD stones ranges from 92 to 97% while that of ultrasound ranges from 15 to 56% in the best hands. [11],[12] Furthermore, EUS has a unique advantage over conventional ultrasound in the diagnosis of early chronic pancreatitis as ultrasound can diagnose it only in the advanced stages. Buscail and his colleagues [13] found that abdominal ultrasound is less accurate than EUS in visualizing the pancreas. EUS was equal to ERCP in detection of biliary strictures. In a study carried by Scheiman and his colleagues [6] in adults, the sensitivity, specificity, PPV (positive predictive value) and NPV (negative predictive value) of EUS for detection of biliary strictures were 67, 100, 100 and 96% respectively. In our study, all cases with negative PD pathology by ERCP were also negative by EUS; therefore, EUS information would be sufficiently reassuring regarding those who prove to be negative, thus enabling the clinician to rule out the possibility of underlying pathology. However, if a case proves to have PD pathology by EUS, further re-assessment by ERCP may be needed. Five of our studied patients had evidence of mild chronic pancreatitis by EUS. ERCP failed to diagnose these 5 patients with parenchymatous changes of pancreatitis as it can only visualize the pancreatic ductal system. Although diagnostic ERCP is widely available, there are many pitfalls in its use to diagnose early chronic pancreatitis. First, it is invasive with a potential for causing pancreatitis. [14] Second, it is expensive. Third, establishing a diagnosis of mild to moderate disease requires complete filling of the pancreatic ductal system, because the diagnosis relies on structural changes in the secondary and tertiary branches (Cambridge classification). [8] In the current study 3 out of the 5 patients diagnosed as having early chronic pancreatitis, had an underlying autoimmune hepatitis and one had sclerosing cholangitis diagnosed during the study. This association drew attention to the possibility of an underlying autoimmune process explaining both entities. Okazaki [15] reported the occasional coexistence of pancreatitis with other autoimmune diseases such as Sj φgren′s syndrome, primary sclerosing cholangitis, [16],[17] primary biliary cirrhosis, [17] sialoadenitis, interstitial nephritis and retroperitoneal fibrosis. In conclusion, pediatric patients with chronic liver disease with underlying biliary pathology can be well evaluated by EUS. EUS has high specificity. Negative cases should not be subjected to further evaluation by ERCP. ERCP should be performed if pancreatic duct pathology needs further assessment or if intervention is planned. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08062t1.jpg] [ms08062t2.jpg] |
| |||||||||

{kind=link}
{kind=link}