 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
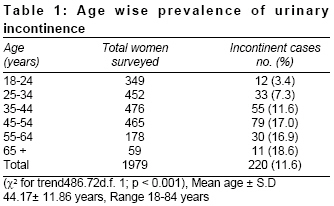
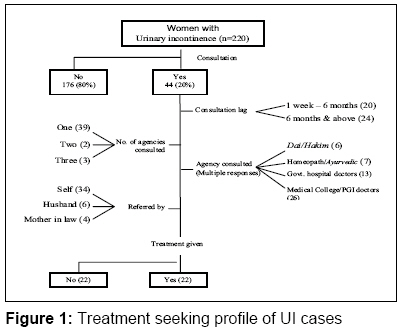
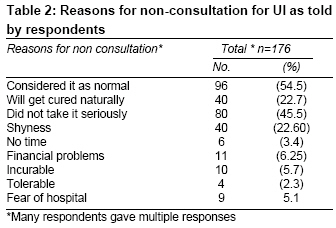
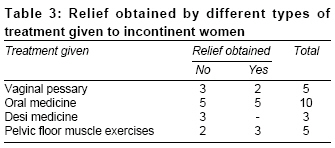
Indian Journal of Medical Sciences, Vol. 62, No. 9, September, 2008, pp. 354-358 ORIGINAL CONTRIBUTION Treatment seeking behavior for urinary incontinence among north Indian women Kumari Santosh, Singh AJ, Jain Vanita School of Public Health, PGIMER, Chandigarh-160 012 Code Number: ms08063 Abstract Background: Urinary incontinence is a common but neglected problem of women.Aims: To ascertain the treatment seeking behavior of north Indian women having urinary incontinence (UI). Setting: Two residential colonies of Chandigarh. Design : Cross-sectional face-to-face interview based study. Materials and Methods: This study was conducted by a trained nurse during April 2005-July 2005 among women aged 18 years and above. Women with UI were identified in a screening survey. They were interviewed individually regarding their treatment seeking behavior and socio-demographic data. Statistical Analysis Used: Percentage, mean, standard deviation, chi-square test. Results: Of the 220 enlisted incontinent women 20% (44) women consulted some health agency. Only 8.6% (19) women had heard about pelvic floor muscle exercises. Seventy-two percent (158) cases had UI for more than one year. The most common reason quoted for not seeking treatment was, 'UI was considered as 'normal', 'did not take it seriously' and 'shyness.' Many (153;70%) women reported that UI affected their daily routine as well as social activities like shopping and visiting friends. Conclusion: Urinary incontinence seriously affected the quality of life of women. Still, consultation rate for UI was low in the north Indian women. Keywords: Reproductive health, treatment seeking behavior, urinary incontinence, women′s health Introduction Globally, urinary incontinence (UI) affects the quality of life of at least one third of women. Many women are too embarrassed to talk about it and some believe it to be untreatable even in western countries. [1],[2] This problem is more pronounced in India, where women usually do not seek treatment for their reproductive health problems and do not vocalize their symptoms. There is a "culture of silence" and low consultation rate among Indian women regarding such problems. [3],[4] Women in India have also been reported to have a high tolerance threshold for seeking treatment.Embarrassment, shyness, lack of money/time, fear of surgery and painare usually the reasons given by women for non-consultation. Moreover, in India, female doctors are usually not available in peripheral are asand women are dependent on their husbands for treatment (escort, permission, money). [5],[6],[7] Against this background, the present study was conducted with an objectiveto ascertain the treatment seeking behavior of incontinent cases in north Indian women.The results of the study will help in planning appropriate strategies for providing optimum treatment to incontinent women. Materials and Methods The study was conducted in PGIMER (Postgraduate Institute of Medical Education and Research) Employees′ Colonyand in Dadumajra Chandigarh, (the field practice area of National Institute of Nursing Education of PGIMER) between April-July 2005. Individual women were the units of study. Dadumajra is a resettlement colony with 3003 houses (population 15000). Systematic random sampling was used to select every third house for the study. The colony has modern sanitary facilities, underground drainage and clean water supply. A few Ayurvedic practitioners and registered medical practitioners are located in Dadumajra. A government all opathic dispensary with MBBS doctors also functions in the colony. Most of the in mates are daily wage earners, rickshaw pullers, drivers and petty businessmen. Some are government employees (mainly sweepers and peons while a few are teachers or clerks). PGIMER Employees′ Colony is situated in the institute campus. The colony houses lower grade employees (sweepers, hospital attendants), clerks, laboratory technicians, nurses and junior engineers of the institute. The total number of houses in the colony at the time of study was 665 (approximate population 3300). All the houses of the colony were surveyed to interview women aged 18 and above. A survey schedule was used to identify incontinent cases through face-to-face interviews and to collect identification and incontinence specific data viz. name, age, parity, education and lower urinary tract symptoms. Stress incontinence was considered if a woman said she leaked urine during coughing, sneezing, exercise, laughing or standing. Urge incontinence was considered when a woman complained that she lost urine during sleep, felt a strong urge to empty her bladder before leaking urine or could not control urine once the urge to void was there. Mixed incontinence was considered if she said yes to both the problems. Severity of incontinence was assessed based on the frequency and volume of incontinence. Participants were asked, "In the last month, for about how many days have you lost urine, even a small amount beyond your control? (Never or less than one / Less than one day per week / Several days per week / Almost daily), with a range of response score from 1-4. Volume of leak was estimated by the question, ′How much urine do you leak?′ A response of "A drop or two" was scored as 1; "enough to change undergarments" was scored as 2. Multiplying frequency score by volume score derived severity of incontinence. A score of 1-2 was considered as mild incontinence, 3-4 as moderate incontinence and a score of more than 4 as severe incontinence. [8] The cases of UI detected by screening survey were interviewed individually regarding their treatment seeking behavior.Verbatim responses were also recorded. Informed consent was taken before the survey.Analysis was done using percentage, range, mean, standard deviation and chi-square test. Results Overall, 230 incontinent women were enlisted among the 1979 screened. Ten women did not agree to participate in the interview (response rate 95.6%). Among the remaining 220 women literacy rate was 60% (132) and 35% (77) had education tenth and above; 45 (20.5%) women were under 35 years of age, the peak age was in the range of 45-54 years. Mean parity was 3.3 (SD 1.4, range 0-8). Sixty percent (132) women lived in nuclear families, a majority of the respondents (75%;165) were housewives and 20% (44) were employed. A majority (79%;174) were Hindus, 8% (18) were Sikhs, 9%(20) were Christians and the rest were Muslims. Per capita monthly income was less than Rs.1000 in 80 (36%) cases while in 42 (19%) it was Rs. 3000 and above; 117 (53%) women were overweight.According to the type of incontinence, 46% (101) women had stress UI, 28% (61) had mixed UI and 26% (57) had urge incontinence. A majority (159; 72%) of the women were suffering from incontinence for more than one year and 96 (43.6%) women had this problem for more than five years.The mean duration of UI was 7 years (range 1 month - 58 years). Prevalence of UI in the study area increased with age [Table - 1]. Overall, 153 (69.5%) women said that UI affected their daily routine.Consultation rate for incontinence was 20% [Figure - 1]. [Table - 2] shows the reasons for nonconsulation. Out of 176 cases 96 (54.5%) considered urinary incontinence as normal, 80 (45.5%) cases did not take it seriously. None of the respondents in DMC was advised surgery, while one woman in PGI was advised to consult a urologist for surgery; however, she did not comply with the advice. The effect of different types of remedies tried by the respondents is shown in [Table - 3]. Discussion The prevalence of UI has been reported to vary globally between 20-60%. [1],[2],[3],[8],[9] In the West, a consultation rate of less than 50% has been reported. [2],[9],[10],[11] The present study yielded a prevalence rate of 11.6%. Still, only afifth of the affected women had consulted someone. A variety of reasons were reported by women for nonconsultation. More than half of the affected women considered UI as a ′normal′ part of women′s lives and mentioned this as a reason for not seeking any treatment. A similar reason was cited in another study. [12] Low consultation rate and the lag in consultation indicate that in India women have profound tolerance. More than half of the respondents consulted a health agency more than six months after the onset of the symptoms. In a few cases it was as late as after 18 years. Other studies have also reported a consultation lag of more than five years. [2],[5],[6],[8],[12],[13] This indicates that either the treatment was not available - or that if some treatment was taken it was ineffective or there was a higher relapse rate. Fear of hospital visits and investigations, financial problems and lack of time were also stated as reasons for nonconsultation. Another reason was shyness to report reproductive system morbidities to a doctor in thealien setting of a hospital. [1],[5] One of the respondents in our study also stated, "I feel ashamed to discuss this problem with anyone. What will other people think about me?" Overall, 48% of the women who consulted someone were not given any treatment, i.e., no medicine, exercise or surgery was advised. In other words, 90% of the total subjects (80% non-consultation + 48% of those who consulted) did not receive any treatment for incontinence. Out of 44 cases who received treatment, only 12 cases had some relief. Similar findings were observed in a study from Taiwan also, where 71% of cases were not given any treatment. [14] In our study, only 8% women had heard about pelvic floor exercises, which were advised to 5 cases only. One of our respondents said," Earlier, some doctor had, in fact, told me about this exercise. But, I just ignored it and thought that he was making fun of me and that it won′t help." Oral antibiotics were prescribed in 10 cases and vaginal pessary in 5 cases. Surgery as a treatment modality for incontinence was not observed among our respondents. Overall, about 50% of these cases reported some relief from the symptoms. In a nutshell, this indicates that requisite respite from the malady is not available to the incontinent women in the study area. This problem of low consultation rate for UI, compounded by the lack of availability of effective treatment further assumes a serious dimension due to the fact that the incontinence affected the quality of life of a majority of women. One of our respondents said, ′′Mere kapde geele ho jaate hein.Jot bhi nahi jala sakti" (My clothes get wet. I can′t even light the sacred candle). Another woman said, "My husband avoids me as my clothes smell of urine." Even children scolded their mothers because of incontinence, as one woman said, ′′Whenever I used to go out, I searched for the toilet first. My sons got irritated and said that it was my daily routine." There is, thus, a definite need to make available an effective cure for urinary incontinence to the hapless women. In this context emphasis needs to be given to trial of pelvic floor exercises which is a non-invasive technique not involving any expenditure and is reported to be quite effective .[15] Further operational research on this aspect may be conducted. Research should also be done to investigate societal influences on treatment seeking behavior in these women. Limitations of the study include the recall bias, since many of the women had incontinence for years together and hence might not been able to recall the treatment related details when the symptoms started. Since the study are as were purposively chosen, generalization of the study results should be exercised with caution. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08063t3.jpg] [ms08063f1.jpg] [ms08063t2.jpg] [ms08063t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}