 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
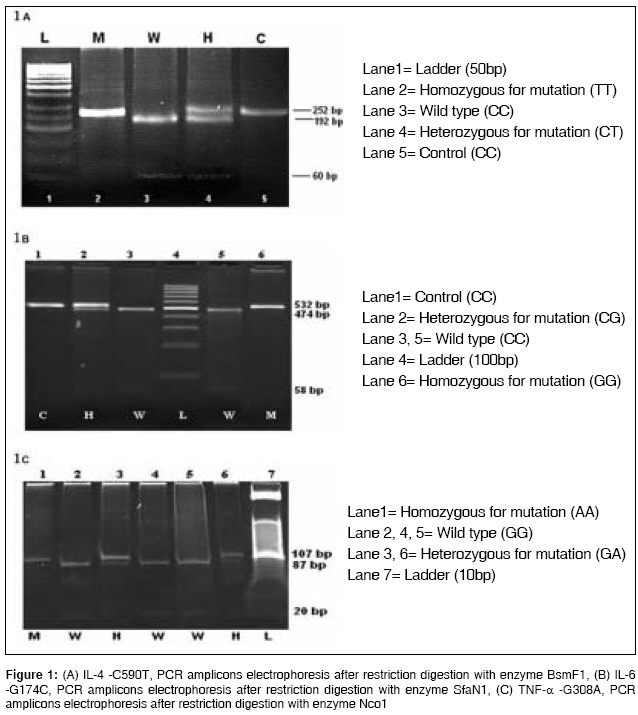
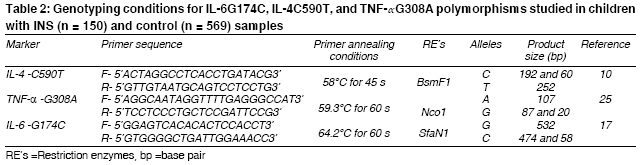
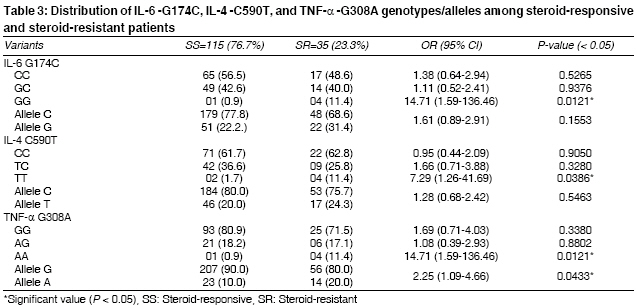
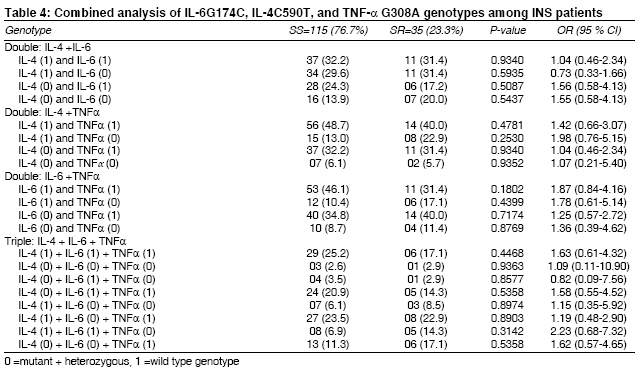
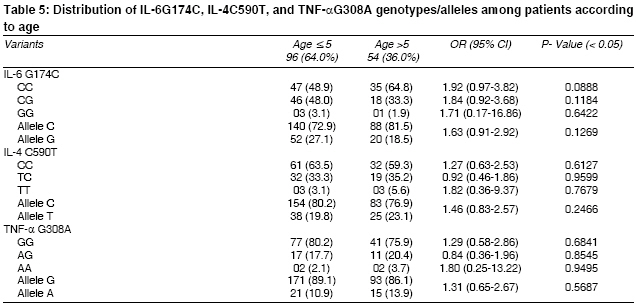
Indian Journal of Medical Sciences, Vol. 62, No. 10, October, 2008, pp. 383-391 ORIGINAL CONTRIBUTION Does cytokine gene polymorphism affect steroid responses in idiopathic nephrotic syndrome? Tripathi Gaurav, Jafar Tabrez, Mandal Kaushik, Mahdi Abbas A, Awasthi Shally, Sharma Raj K, Kumar Alok, Gulati Sanjeev, Agrawal Suraksha Department of Medical Genetics, SGPGIMS, Lucknow Code Number: ms08069 Abstract Background: Immunological responses may be possibly involved in the pathogenesis of idiopathic nephrotic syndrome (INS). Cytokines act as a potent immunomodulator. Pathogenesis of INS is associated with Th1 and Th2 cytokines imbalance. Keywords: Idiopathic nephrotic syndromes, IL-4, IL-6, TNF-α, steroid resistant, steroid responsive Introduction Idiopathic nephrotic syndrome (INS) is the most common glomerular disorder of childhood, with 1 to 2 new cases per 100,000 children per year. INS is characterized by the presence of proteinuria, which is associated with hypoalbuminemia and hyperlipidemia. Some patients with INS do not respond to glucocorticoids, i.e., they are steroid resistant (SR). Most of the children with INS are steroid sensitive (SS), i.e., they achieve remission following steroid treatment. However, some of the children with steroid sensitive nephrotic syndrome (SSNS) will undergo relapse once or more. About 50% of the relapsers are either frequent relapsers or develop steroid dependence. [1] The mechanisms underlying these different responses to steroids are not very well understood; however, there may be certain genetic factors involved for these differential drug responses. Histology of childhood INS is most commonly represented by minimal-change nephrotic syndrome (MCNS) followed by focal segmental glomerulosclerosis (FSGS) and rarely by membrano-proliferative glomerulonephritis (MPGN) and membranous glomerulonephritis (MGN). Children with FSGS, MPGN, and MGN usually have a poorer response to glucocorticoids. [1] Idiopathic nephrotic syndrome was proposed to be a disorder of T-cell dysfunction. [2] The mechanisms by which T-cells affect the course of the disease remain elusive. However, there may be circulating factors released from activated T-cells which may affect the pathogenesis of the disease. Th1 cells produce IL-2, IFN-γ, and tumor necrosis factor-beta (TNF-β ); and promote both macrophage activation resulting into DTH, and production of complement-fixing and opsonizing antibodies. Th2 cells, which synthesize IL-4, IL-5, IL-6, IL-10, and IL-13, provide optimal help for antibody production; and promote both mast cell growth and eosinophil differentiation and activation, resulting in humoral responses. [2],[3] INS is considered to be an immune-mediated disease; [4] however, the contribution of Th1 and Th2 cytokines is a matter of debate. Several cytokines are considered prime candidates for the role of mediators of INS. [5] However, such data is missing in the literature from the Indian subcontinent. The present study was conducted to investigate the possible association between IL-4, IL-6, and TNF-α gene polymorphisms and their effect on steroid responses in 150 children with idiopathic nephrotic syndrome. We have also tried to see the synergistic effects of various cytokine SNP polymorphisms; especially the constellation of TNF-α and IL-6 genetic variants might predispose some INS patients to differential response to inflammation, and also to the steroids. Materials and Methods Patients All children were subjected to detailed history-taking and physical examination. In addition, following biochemical tests were done to confirm the diagnosis of nephrotic syndrome: serum creatinine, total protein, albumin, cholesterol, triglycerides, urinary routine microscopy examination, urine protein and creatinine ratio in a spot sample Based upon the difference in steroid responsiveness, renal biopsies were carried out in most of the steroid-resistant cases and some of the cases of SD and FR as per availability of consent. The characteristics of INS patients included in the present study are shown in [Table - 1]. An informed written consent was obtained from all participants. The study was approved by the ethical committee of SGPGIMS and Department of Biotechnology, Government of India. Blood collection and DNA extraction Analysis of the IL-6, IL-4, and TNF-α genotype To improve the genotyping quality and validation, all mutant and heterozygous samples were re-genotyped blindly and results were noted only for those samples which were reproducible with no discrepancy. Genotyping of 20% of the samples was confirmed by DNA sequencing. Statistical analysis Results Allele and genotypes frequencies of IL-6, IL-4 and TNF-α were compared between the SS and SR groups. Among 150 INS patients, 115 (76.7%) were steroid responsive (SS) and 35 (23.3%) were steroid resistant (SR). The allele and genotype distribution of IL-6, IL-4, and TNF-α gene polymorphisms in SS and SR groups are shown in [Table - 3]. There was a strong association between IL-6 and IL-4 at the genotypic level in SS and SR groups (P = 0.0121, OR = 14.71, 95% CI = 1.59-136.46; and P = 0.0386, OR = 7.29, 95% CI = 1.26-41.69) respectively. Whereas TNF-α showed a strong association at genotypic level (P = 0.0121, OR = 14.71, 95% CI = 1.59-136.46) as well as at allelic level (P = 0.0433, OR = 2.25, 95% CI = 1.09-4.66) in SS and SR groups. Further synergistic effects of IL-4, IL-6, and TNF-a gene polymorphisms were evaluated, and no association of combined genotypes with SS and SR groups were observed [Table - 4]. An attempt was made to correlate the allele frequency of INS with onset of the disease. We divided the patient population into 2 age groups: ≤5 years and> 5 years. No significant difference was found between the 2 groups when age of onset and co-occurrence of the various genes and their genotypes were studied [Table - 5]. Discussion In the present study we have investigated an association between cytokines gene polymorphisms in 150 children with INS and their response to steroids. Children with INS were genotyped for the IL-4, IL-6, and TNF-α gene polymorphisms. Our results demonstrated that IL-6 -G174C and TNF-α -A308G polymorphism may be one of the genetic risk factors for INS and may affect steroid response among the north Indian population. Our results revealed that there was a strong association between IL-4 and IL-6 at genotypic level in SS and SR groups (P = 0.0386 and P = 0.0121 ). Interestingly TNF-α showed a strong association at genotypic level (OR = 14.71), as well as at allelic level (OR = 2.25) in both the SS and SR groups, which demonstrates that this may be one of the risk factors for INS and may affect steroid response. There are reports showing cytokine genes polymorphism to be associated with the development and severity of inflammatory diseases. [7],[8],[9] Minimal-change nephrotic syndrome (MCNS) in children is frequently associated with allergy and immunoglobulin E production. T helper subtype 2 cytokines, such as interleukin-4 (IL-4), may have an important role in the development of atopy. Some of the studies suggest that genetic variations in IL-4 may be associated with predisposition to MCNS, and partially to the clinical course of MCNS. [10],[11],[12] IL-4 production by peripheral Th cells is up-regulated in patients with MCNS and correlated with the severity of proteinuria. [13] Our results demonstrated that IL-4 -C590T SNP influences the prognosis of the disease. We have found that TT genotype was higher in the steroid-resistant group (P = 0.0386) as compared to SR. IL-6 and its genetic variants have been studied in various disorders which involve susceptibility to recurrent infections; thrombophilia; and immunological alterations, such as celiac disease, breast cancer, systemic lupus erythromatosus, and leishmaniasis. [14],[15],[16],[17] Though the roles of IL-6 and IL-6 -G174C are not well studied in nephrotic syndrome, their role have been found in mesangial proliferative glomerulonephritis and end-stage renal disease. [18] Our study revealed that GG genotype of IL-6 -G174C is more prevalent in the steroid-resistant group, thus pointing towards a poorer prognosis in children with nephrotic syndrome. Tumor necrosis factor alpha (TNF-α) is a potent immunomodulator and pro-inflammatory cytokine and has been implicated in many pathological processes. Polymorphism at position -308 of the TNF-α promoter, representing G to A base transitions, has been linked to increased TNF transcription. [19],[20] Earlier studies have shown increase of TNF-α synthesis and gene expression in patients with idiopathic nephrotic syndrome and focal glomerular sclerosis. [21],[22] Since TNF-α activates NF-kB and angiotensinogen [23],[24] hence steroid induced immuno- suppression is critically dependent upon inhibition of NF-kB Elevation of TNF-a has been found in the plasma and urine of patients with INS. [25] We studied the genotype of TNF-α G308A in patients with nephrotic syndrome and its relation with steroid responsiveness. AA genotype of TNF-α genotype was found to be significantly higher in the steroid-resistant group, along with a higher ′A′ allele frequency (20.0%). The transcriptional and post-transcriptional alterations of NF-kappaB/I-kappaBalpha in nephrotic syndrome [26] can be a potential pathway for TNF-α action in determining steroid responsiveness; however, this needs further evaluation for determining the proper therapeutic approach in children with nephrotic syndrome. Conclusion We may state that the studied polymorphism might affect steroid response in INS patients. Further, atopy-related pathway (involving IL-4) may be a good modulator for the prognosis and steroid resistance in nephrotic syndrome; whereas susceptibility to infection (involving IL-6) and markers of inflammation like TNF-α seems to determine, at least partly, the prognosis of nephrotic children, especially their response to steroid treatment. However, the role of other genetic and environmental factors cannot be ruled out. Hence further studies are required to precisely define the biochemical mechanism of action of these genes, which can help in the development of methods for the prediction, prevention, and treatment of idiopathic nephrotic syndrome.Acknowledgment We are indebted to the Department of Biotechnology (DBT) New Delhi, Government of India and SGPGIMS for the financial assistance.References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08069f1.jpg] [ms08069t4.jpg] [ms08069t1.jpg] [ms08069t2.jpg] [ms08069t5.jpg] [ms08069t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}