 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 62, No. 10, October, 2008, pp. 397-406 ORIGINAL CONTRIBUTION Reference ranges for lymphocyte subsets in adults from western India: Influence of sex, age and method of enumeration Das BibhuR, Bhanushali AparnaA, Khadapkar R, Jeswani KanchanD, Bhavsar Mita, Dasgupta A Research and Development, SRL Ranbaxy Ltd, Plot No 113, MIDC,15th Street, Andheri (East), Mumbai-400 093 Code Number: ms08071 Abstract Background: The enumeration of absolute CD4 counts is of primary importance, since therapeutic protocols for HIV1 patients are based on these.Aims: To establish reference ranges for the CD4 and CD8 T-lymphocytes in the Indian population. Settings and Design: Enumeration of absolute numbers and percentages of lymphocyte subsets was performed in 252 healthy adult Indians. Methods and Materials: The assays for SPT were carried out using the Beckman EPICS XL-MCL flow cytometer and the cytostat tetraCHROME reagent containing CD45/CD8/CD4/CD3 monoclonal antibodies. For comparison with DPT the absolute lymphocyte count was obtained using the Coulter STK-S fully automated hematology analyzer. Statistical Analysis: Regression analysis and Students t test were used for data analysis. Results: Median values were as follows; absolute CD3 counts 1446 cells/mm3 (total), 1361 cells/mm3 (males) and 1511 cells/mm3 (females); absolute CD4 counts are 771 cells/mm3 (total), 705 cells/mm3 (males) and 839 cells/mm3 (females); absolute CD8 counts are 555 cells/mm3 (total), 552 cells/mm3 (males) and 561 cells/mm3 (females). The median CD4/CD8 ratio for the total samples was 1.34, for males 1.22 and for females 1.49. Conclusions: In this study we have established reference ranges for normal Indian adults using the fully automated Single Platform Technology. The lymphocyte subsets values of our population are closer to those of the population from Botswana and China rather than the Western population. The absolute CD3 and CD4 counts and the CD4:CD8 ratio are higher in females than in males. Consistently higher values are obtained by the DPT as compared to the SPT. Keywords: CD4 T lymphocytes, CD-8 T-lymphocytes, reference range, single platform flow cytometry. Introduction The progressive loss of CD4 T lymphocytes through virally mediated cell destruction is the predominant pathophysiological manifestation of the human immunodeficiency virus 1 (HIV1). [1] According to the Indian National AIDS Control Organization (NACO) estimates, 5.134 million people were living with HIV in 2004. [2] Therapeutic protocols for HIV1 patients are based on CD4 lymphocyte absolute counts, which are used as a prognostic marker [3] and also to monitor the effectiveness of antiretroviral treatment. Hence reliable methods for enumeration of lymphocyte subsets are of great importance, as new drugs may induce rapid and dramatic modifications of otherwise relatively stable or regularly decreasing lymphocyte counts. [4],[5] The enumeration can be accomplished using single or dual platform counting technologies. However it is the single platform approach (SPT), that is considered as the gold standard for absolute cell assessments. [6] In a multisite trial, [7] comparison of two different SPT methods with a predicate two-color assay in which the absolute lymphocyte count was derived by conventional hematology was employed. They concluded that the fully automated Beckman Coulter tetraONE system resulted in a small but significant improvement in the within laboratory precision of the CD4 and CD8 cell counts and percentages. However a recent study [8] states that they would prefer DPT over SPT for activation markers (DR, CD25 and CD38) of HIV patients. There have been studies from northeast India, [9] from the Western region [10] and a multi centric study, [11] however, given the differences in the technology and ethnicity of the Indian population a need was felt to establish immunohematological reference ranges for the Indian setting based on NCCLS guidelines. We have utilized the fully automated Beckman Coulter tetraONE system employing CD45 lymphocyte gating, automated analysis and Flow-Count fluorospheres to establish the reference ranges. Materials and Methods Subjects: A total of 252 adults from Western Maharashtra (120 men aged from 18 to 56 years and 132 women aged from 15 to 56 years) were enrolled in this study. Individuals included were healthy adults between 15 and 60 years of age presenting for a routine health check-up. The participants had to fill a questionnaire regarding loss/gain of weight, vaccination, infection in the past 4 weeks including viral, bacterial, fungal, and other pathogens, use of antibiotics in the past 4 weeks, hospitalization within the past 2 years, and history of medication, including analgesics, nonsteroidal anti-inflammatory agents, anti-ulcer drugs, anti-hypertensive drugs, and other cardiovascular drugs. Subjects who reported a positive history for any of these items were excluded from the study. Blood specimens were collected after an overnight fast of 12 hrs by veni-puncture using the vacutainer system from Becton Dickinson (Franklin Lakes, NJ USA) in the anticoagulant EDTA. The samples were analyzed on the day of the collection. Instrumentation: The hematology instrument used for determining absolute lymphocyte count by the dual platform technology (DPT) was a Coulter STK-S which is a fully automated hematology analyzer and quantitatively measures and computes hematological quantities including a full "five-part" differential. The flow cytometry analysis was performed with the Beckman Coulter EPICS XL-MCL flow cytometer (Beckman Coulter, Miami, USA.) using the tetraONE SYSTEM software. Instrument performance was ensured by the following:
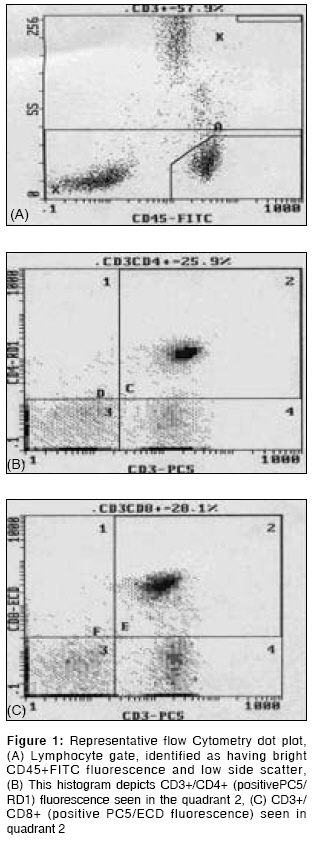
Flow cytometric immunophenotyping: However absolute CD3 + CD4 + and CD3 + CD8 + were calculated by multiplying the specific subset percentage by the absolute lymphocyte count. Single Platform Method: The assay was performed in the following manner for the single platform technology (SPT). 50 µl whole blood specimens were incubated with 5 µl of reagent CYTO-STAT tetraCHROME containing CD45-FITC/CD4-RD1/CD8-ECD/CD3-PC5 monoclonal antibodies. Red Blood Cells are lysed with the Immunoprep TM reagent system (Beckmann Coulter), 50 µl flow-count fluorosphere added and analyzed using CS3D flow count protocol. The tetraOne system software was used for gating and analysis of CD4/CD8. The software provides 3-dimensional lymphocyte gating using forward scatter, side scatter and CD45 [Figure - 1]. Flow count fluorospheres provide real live absolute counts of lymphocytes. To obtain the absolute count determination on the EPICS XL flow cytometer, at least 1,000 fluorospheres are counted; the absolute count for the whole blood sample is then automatically calculated using the following formula: Absolute Count (cells/µL)
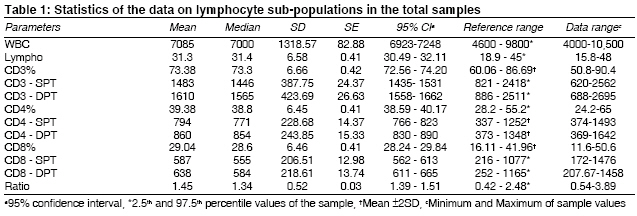
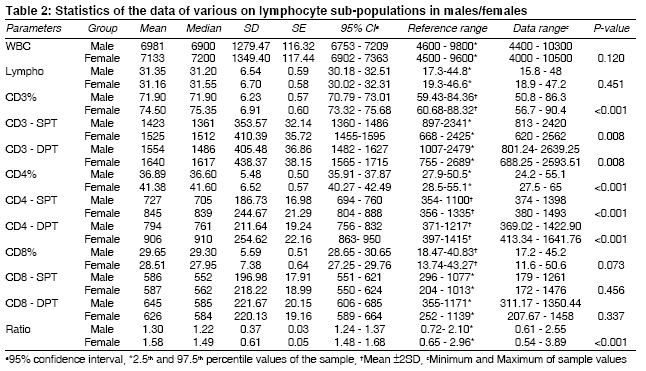
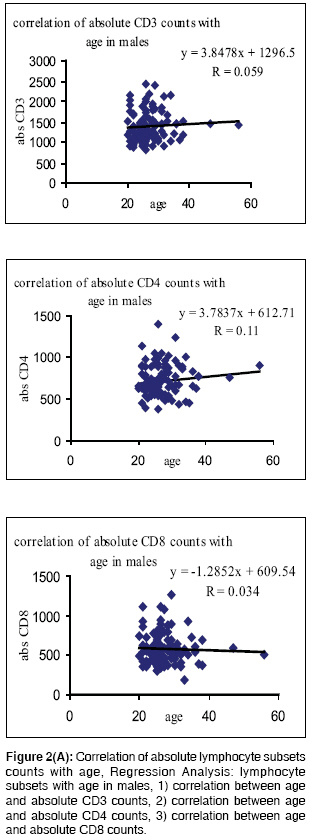
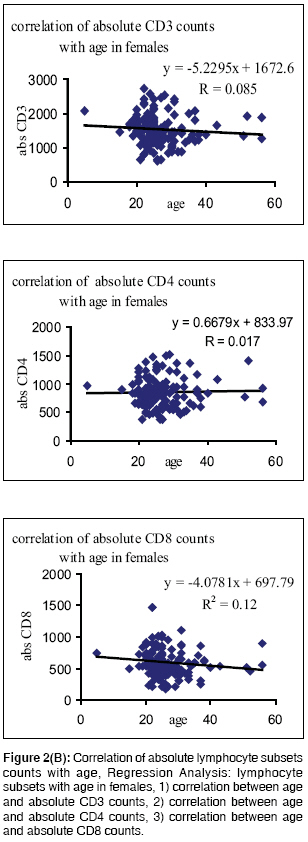
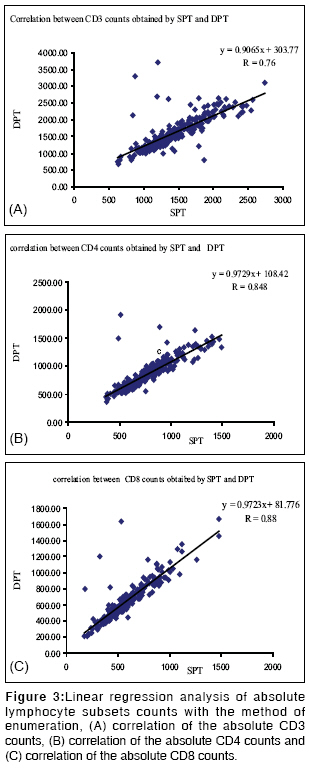
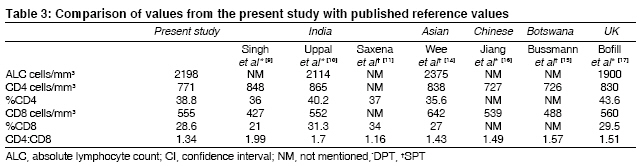
Statistical Analysis Results Of the 252 samples analyzed, 120 were males and 132 were females. These samples were selected on the basis of the exclusion criteria as mentioned earlier. The median age of males was 26 years and that for females was 25 years. Summary statistics for white blood cells (WBC), lymphocyte counts and percentage as well as absolute counts of lymphocyte subsets in the total sample are given in [Table - 1]. Gender specific values of these parameters are given in [Table - 2]. [Table - 2] also reflects the significance of these parameters with respect to sex. The median %CD3 value in the total sample was 73%, (in males 72% and in females 75%). The median absolute CD3 counts in total population was 1446 cells/mm 3 (in males 1361 cells/mm 3 and in females 1511 cells/mm 3 ). The overall median %CD4 count was 39%, (in males 37% and in females 42%). The median absolute CD4 counts in the total population was 771 cells/mm 3 (in males 705 cells/mm 3 and in females 839 cells/mm 3 ). The median %CD8 count was 29% (in males 29% and in females 28%). The median absolute CD8 counts in total population was 555 cells/mm 3 (in males 552 cells/mm 3 and in females 561 cells/mm 3 ). The median CD4/CD8 ratio for the total population was 1.34 (for males 1.22 and for females 1.49). When the parameters were analyzed on the basis of gender, statistically significant differences were seen, for absolute counts of CD3 lymphocytes (P = 0.008) and absolute CD4 counts (P < 0.001), but not for absolute CD8 counts (P = 0.456). The median values were higher in females. The CD4:CD8 ratio was also higher in females (P < 0.001). No significant differences were found between age and the different parameters studied [Figure - 2a, 2b]. Comparative values obtained by the single platform technology and the double platform technology are also given. The absolute CD3 count in the total population shows a difference of greater than 100 cells/µ1 between SPT and DPT, and in both CD4 and CD8 absolute counts a difference of greater than 50 cells/mm 3 . Regression analysis was done to compare the correlation between the two techniques. The correlation coefficient R for CD3 counts was 0.76, for CD4 counts 0.84 and for CD8 counts 0.88. When the values obtained by the two techniques were again analyzed for statistical significance by the Students t test using paired sample criteria statistically significant difference P < 0.001 was seen for CD3, CD4 as well as CD8 counts [Figure - 3]. Values obtained by the SPT have been used to establish the reference range. Discussion The value of lymphocyte subsets obtained in our population is different from those of the other populations [Table - 3]. Our study is at variance with values obtained in the Indian cohort as well as the Chinese and Malaysian populations of a multi-racial study. [14] Interestingly the study employed SPT but a different protocol (Trucount tubes). Our results are however similar to that of the population from Botswana [15] and China. [16] In the Indian scenario, the study from Western India [10] has enumerated higher counts and reported that these are similar to adult Caucasians. [17] The multi centric study from India [11] has given the national means of percentages of lymphocytes as CD3 68.65%, CD4 34.04% and CD8 14.67%. The values of the lymphocyte subsets in our study, are higher, which could be ethnicity related (lower values of lymphocyte population have been reported for South Indian population, [18] which also forms a part of this multi centric study) or method related (gating strategy was based on forward-side scatter plot). Gender specific variation in absolute CD4 and CD8 counts has been seen in our study [Table - 2]. These results are akin to many other studies, which have reported that males have higher CD8 percentages and females have higher CD4 percentages. [5],[19],[20] Differences in immune cell numbers between genders may be secondary to the differential influences of sex hormones shown in murine studies. [21] The impact of age on lymphocyte subsets is not well established. Some studies have shown that the number of CD4 + cells increased while the number of CD8 + decreased with age, [22],[23] while others state that the numbers of both CD4 + and CD8 + increase with age. [24] Our results do not show any significant differences in the percentages of CD4 and CD8 as well as the CD4:CD8 ratio with respect to age [Figure - 2a, 2b]. A multi centric study [25] had highlighted three major reasons for interlaboratory variability: variations in sample processing, suboptimal lymphocyte gating that uses light scattering and variations in white cell count measurement. Other studies have also shown that the major source of interlaboratory variation in lymphocyte subset enumeration is the automated blood analyzer when DPT is used. [26],[27] This source of variation can be eliminated by the SPT that is adopted in this study. Conclusion We have established reference ranges for the lymphocyte subsets for healthy Western Indians using the tetraONE System (which has automated CD45 lymphocyte gating and analysis and fluorosphere-derived absolute counting) and following the latest guidelines. Our study reveals that the lymphocyte subsets in our population are closer to those of the population from Botswana, and China than the Western population, and this needs to be taken into account while devising protocols for the treatment of individuals with HIV. Our study also confirms the gender difference in the lymphocyte subset counts, however the impact of age is less certain.References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08071f3.jpg] [ms08071f2b.jpg] [ms08071t3.jpg] [ms08071t1.jpg] [ms08071f1.jpg] [ms08071f2a.jpg] [ms08071t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}