 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 62, No. 10, October, 2008, pp. 407-415 ORIGINAL CONTRIBUTION Associations between sex hormone binding globulin and metabolic syndrome parameters in premenopausal obese women Akin Fulya, Bastemir Mehmet, Alkis Esma, Kaptanoglu Bunyamin Department of Endocrinology and Metabolism, Pamukkale Universitesi Endokrinoloji ve Metabolizma Hastaliklari, Kinikli Kampusu 20070 Denizli Code Number: ms08072 Abstract Background and Aims: The aim of this study was to determine sex hormone binding globulin (SHBG) concentrations in premenopausal obese women and to evaluate the relationships between sex hormones and features of the metabolic syndrome (MetS).Settings and Design: Retrospective cross-sectional analysis was carried out on 350 obese patients aged 25 to 69 years referred to the Department of Endocrinology, Pamukkale University in 2002-2003. Materials and Methods: 125 premenopausal euthyroid patients were eligible for this study. Subjects were divided into two groups according to the body mass index (BMI): Group I, women with BMI < 30 kg/m 2 (n = 17) and Group II,, women with BMI ≥ 30 kg/m 2 (n = 108). Median SHBG concentration of Group I was 50.1 nmol/L. Group II was divided into two subgroups according to the median SHBG concentration of Group I: subjects with high SHBG levels (SHBG concentration ≥ median level of the control group, i.e ≥ 50.1 nmol/L) and subjects with low SHBG levels (< 50.1 nmol/L). All statistical analyses were performed using SPSS 9.0 software (SPSS Inc.). Results: No significant difference was found in mean age between the low and high SHBG groups. The low SHBG group was significantly heavier, and with higher waist circumference than the high SHBG group. In the low SHBG group, fasting glucose, postprandial glucose and gamma glutamyl transferase (GGT) and free androgen index (FAI) were significantly higher. Lipid profile, blood pressure, uric acid, insulin and HOMA were found similar between two groups. Linear regression analyses revealed that body mass index and FAI were significant, being independent predictors of SHBG concentrations in premenopausal women. (r = 0.365, r square = 0.134). Conclusions: It is concluded that low SHBG concentrations may indicate visceral obesity and glucose intolerance in premenopausal women. Keywords: Insulin resistance, metabolic syndrome, obesity, premenopausal women, sex hormone binding globulin. Introduction Sex hormone binding globulin (SHBG) is the major binding protein for gonadal steroids in the circulation. [1] It was originally described as a hepatically secreted protein and thereby regulating the availability of free steroids to hormone-responsive tissues. [2] In women, increased androgenicity, as reflected by low circulating SHBG concentrations, has been related to hyperinsulinemia, glucose intolerance, and insulin resistance, as well as to the risk of cardiovascular disease and type 2 diabetes. An androgenic sex steroid profile as reflected by low circulating SHBG is also associated with an increased accumulation of abdominal fat in women. [3] At present there is much evidence that insulin may be an important modulator of SHBG concentrations. In vitro, insulin is a potent inhibitor of SHBG production by HepG2 cells [4] and reduces the stimulatory effect of 17b-estradiol and thyroxine. [5] In vivo, reduced serum SHBG levels may indicate the presence of insulin resistance states with hyperinsulinemia, such as polycystic ovary syndrome [6] or obesity. [7] Furthermore, a recent prospective study identified low levels of SHBG as a risk factor for future diabetes mellitus. [8] Thus, one may argue that low SHBG levels are associated with CHD by indicating the presence of the insulin resistance / hyperinsulinemia syndrome. Previous studies have demonstrated that reduced plasma levels of SHBG are related to alterations in several features of the MetS in men and women. [9],[10],[11],[12] Most of the research linking low SHBG and high androgens to cardiovascular risk has been restricted to postmenopausal women. [13],[14],[15] The aim of this study was to determine SHBG concentrations in premenopausal women who were otherwise healthy, and to evaluate the relationships between SHBG concentrations and features of the MetS. Materials and Methods Retrospective cross-sectional analysis was carried out on 350 obese and overweight patients aged 25 to 69 years referred to the Department of Endocrinology and Metabolic Diseases of Pamukkale University hospital in 2002-2003. Records are stored in folders in the institution and the same person retrieved all the data. We studied the Turkish population living in Denizli province of Aegean geographical region of Turkey. Our samples were from the inner part of the Aegean region of Turkey. All of the patients were obese and overweight, BMI > 25kg/m 2 . Patients who were under treatment with contraceptive drugs or hormone replacement therapy (HRT), or diagnosed with polycystic ovary disease, thyroid disease, chronic renal failure, chronic hepatopathy or cancer, were excluded from the study. Presence of medical conditions was assessed through self-report. Thyroid status was assessed by freeT3 (fT3), freeT4 (fT4), and thyrotrophin (TSH) levels. Insulin resistance was estimated by homeostatic model assessment ratio formula [HOMA-IR = (Fasting plasma insulin (µIU/mL) x fasting plasma glucose (mmol/L))/22,5]. [16] Free androgen index (FAI) was used to estimate the amount of testosterone unbound by SHBG and thus, immediately biologically active. FAI was calculated as the ratio of testosterone (ng/ml) to SHBG (ng/mL)x100. [3] The definition of menopausal status was in accordance with the following criteria: [17] -Women presenting normal menses or who in any case reported at least 10 cycles in the previous year and without climacteric-related symptoms, and having follicle stimulating hormone levels lower than 12.75 IU/l, were included in the premenopausal group. 125 premenopausal euthyroid patients were eligible for this study (mean age: 35.6 ± 9.35 Patients were divided into two groups according to the body mass index (BMI): Group I (overweight women), women with BMI < 30 kg/m 2 (n = 17) and Group II (obese women), women with BMI > or = 30 kg/m 2 (n = 108). The values of the SHBG concentrations were scattered and median SHBG concentrations were used. Median SHBG concentration of Group I was 50.1nmol/L. Group II (obese women) was divided into two subgroups according to the median SHBG concentration of Group I. Women with high SHBG levels (SHBG concentration > or = median level of the control group, i.e.> or =50.1nmol/L) (n = 26) and women with low SHBG levels (< 50.1 nmol/L) (n = 82). Anthropometric measurements Blood pressure Metabolic syndrome definition
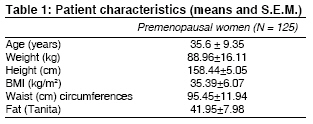
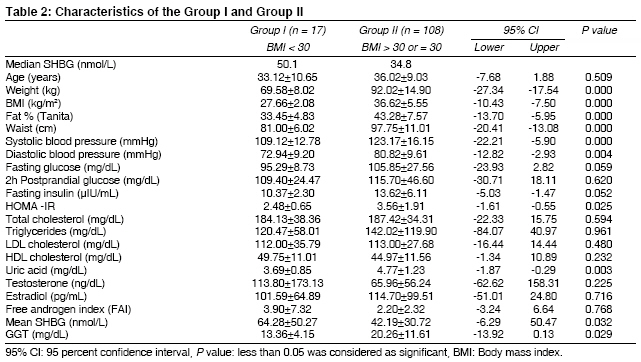
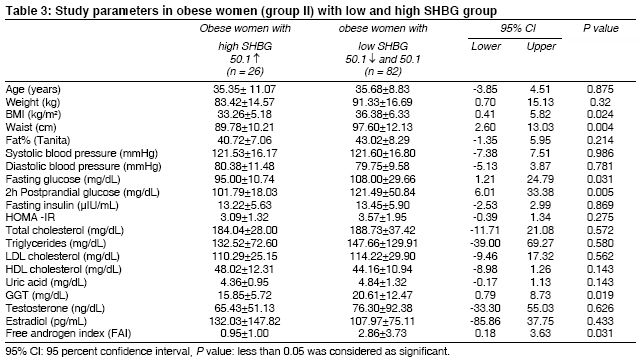
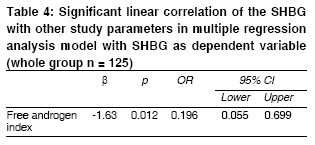
Laboratory analyses Statistical analyses P value less than 0.05 was considered as significant. Results The patient characteristics (means and S.E.M.) of the studied group and the measured parameters are shown in [Table - 1]. Median SHBG concentration of Group I was 50.1 nmol/L (mean value was 64.28 nmol/L with a standard deviation of 50.27 nmol/L). The values of the SHBG concentrations were scattered, and median SHBG concentrations were used. Characteristics and study parameters in women in Group I and Group II are shown in [Table - 2]. Subjects in Group I had lower BMI, with significantly lower waist circumference, fat %, systolic and diastolic blood pressure, uric acid, and GGT level (P = 0.000, P = 0.000, P = 0.000, P = 0.000, P = 0.004, P = 0.003, P = 0.029). HOMA values were significantly lower and SHBG concentrations were significantly higher in this group as well (P = 0.025, P = 0.025). Group II (our obese group) was divided into two subgroups according to the median SHBG concentration of the Group I. The obese women with SHBG concentrations > 50.1nmol/L were regarded as the group with high SHBG and women with SHBG concentrations < 50.1 nmol/L were regarded as the group with low SHBG. The study parameters of the obese subgroups are shown in [Table - 3]. No significant difference was found in mean age between low and high SHBG group (P = 0.875). The low SHBG group was significantly heavier, and had higher BMI, with higher waist circumference than high SHBG group (P = 0.032, P = 0.024, P = 0.004). In the low SHBG group, fasting glucose, postprandial glucose, GGT and FAI levels was significantly higher (P = 0.001, P = 0.005, P = 0.019, P = 0.031). Similar lipid profile (TG, HDL cholesterol), blood pressure, uric acid, insulin and HOMA were found between two groups (P = 0.580, P = 0.138, P = 0.986, P = 0.781, P = 0.143,P = 0.869, P = 0.275). Significant correlations of the SHBG with other study parameters using multiple linear regression analysis, with SHBG as the dependent variable are shown in [Table - 4]. Linear regression analyses (backward) revealed that free androgen index (FAI) was a significant independent predictor of SHBG concentrations in premenopausal women (P = 0.012)[Figure - 1]. Discussion Whether SHBG is a causal agent of the MetS or merely represents a marker for primary endocrine abnormalities leading to these metabolic alterations remains unclear at the present time. We investigated the interactions of a variety of clinical and laboratory parameters characterizing the metabolic syndrome. We focused on premenopausal women, because most of the previous studies were on postmenopausal subjects. Tchernof, Garaulet and coworkers performed similar studies in premenopausal women too. [3],[19] But the size of our study group was larger than Tchernof and Garaulet′s groups. The biggest epidemiological study about SHBG and cardiovascular risk in multiethnic premenopausal and perimenopausal women is the SWAN (Study of Women Across the Nation) study. They reported that low SHBG and high FAI were strongly associated with CV risk factors even after controlling for BMI. [20] In our study FAI was used to estimate the amount of testosterone unbound by SHBG, thus biologically active like SWAN group. In the present study, obese women with low SHBG concentrations had significantly higher FAI. The cause and effect relationships between SHBG concentrations and MetS components in obese women could not be assessed because of the cross sectional nature of our study. Another big comprehensive study was performed by Hajamour et al. [12] Their data were obtained from Quebec Family Study (QFC). They reported that plasma SHBG level may represent a significant predictor of the MetS in men and premenopausal women. The association between plasma SHBG and variables of glucose homeostasis were significant in premenopausal women. [7] Our results also confirm their data. Our study shows strong relationships between SHBG and anthropometric measurements and fasting glucose, postprandial glucose, GGT levels and FAI in premenopausal women. Linear regression analyses (backward) revealed that BMI and FAI were significant independent predictors of SHBG concentrations in premenopausal women [Figure - 1]. The accelerated accretion of adipose tissue in the intra-abdominal region coincident with the onset of menopause may explain part of the increased risk of cardiovascular disease in postmenopausal women. [4] But premenopausal women showed gynoid type obesity, with a smaller abdominal perimeter. They were lowest in most abdominal fat distribution parameters. [19] In this study, we found that total or intra-abdominal obesity mediated an important part of the relation between low SHBG and an altered metabolic profile by using BMI and waist circumference. The results of the present study are concordant with previous investigators. [3],[21],[22],[23] Our obese group showed upper body obesity, and had higher waist circumference and higher HOMA value than overweight subjects. Higher uric acid level and blood pressure was found as expected. Hyperuricemia is reported to be an inherent component of MetS and could be used as a simple marker for insulin resistance. Low SHBG frequently coincides with components of MetS, such as low levels of HDL cholesterol and high levels of triglycerides and apolipoprotein B. [11],[24],[25] In this study, no significant difference was found in mean insulin concentrations, HOMA index, blood pressure, triglycerides, HDL and uric acid between the low and high SHBG groups. Determinants of SHBG blood concentrations are likely to change on passing from premenopausal to postmenopausal status. [26] FAI is an important determinant of SHBG in both premenopausal and postmenopausal women as expected. Our finding also confirms these results. It is known that estrogens protect pancreatic b-cells from apoptosis and have insulinotrophic effects. [27] In postmenopausal status this effect is lost and insulin levels decrease. The positive effect of estradiol on SHBG levels is probably stronger in premenopausal women than in postmenopausal women. That is why SHBG didn′t correlate insulin resistance and MetS component in premenopausal obese women. In a recent study, it has been noted that after menopause, the impact of insulin resistance on SHBG level seems more important than estradiol. Therefore, it could be argued that SHBG level can be correlated with insulin resistance for postmenopausal women. [28] The major difficulty with our study is that values of the SHBG concentrations were scattered. The mean value was 64.2 nmol/L with SD of 50.3, therefore we used median SHBG concentration to show the significance of the work. A similar study was designed by Cikim et al.[29] They studied 307 premenopausal women. They used median SHBG levels too. Their low SHBG group was significantly younger, with higher waist-to-hip ratio (WHR). Triglycerides, uric acid, insulin and HOMA values were significantly lower their low SHBG group. Their multivariant regression analyses showed age and uric acid concentrations in the whole group. They reported that low SHBG concentrations may indicate a severe degree of insulin resistance in premenopausal women. But in our study, no significant difference was found in mean age between low and high SHBG group. The low SHBG group was significantly heavier and had higher BMI with higher waist circumference than high SHBG group. Although fasting glucose, postprandial glucose, GGT levels and FAI were significantly higher in our low SHBG group, lipid profile (TG, HDL cholesterol), blood pressure, uric acid, insulin and HOMA were found similar between the two groups. In summary, according to our findings, SHBG levels didn′t correlate with insulin resistance in premenopausal obese women. Linear regression analyses (backward) demonstrated that BMI and FAI were significant independent predictors of SHBG concentrations in premenopausal obese women. It is concluded that low SHBG concentrations may indicate visceral obesity and glucose intolerance in premenopausal obese women. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08072t3.jpg] [ms08072t2.jpg] [ms08072t1.jpg] [ms08072t4.jpg] [ms08072f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}