 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
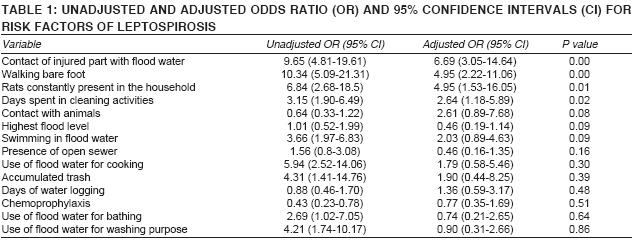
Indian Journal of Medical Sciences, Vol. 62, No. 11, November, 2008, pp. 431-438 ORIGINAL CONTRIBUTION A case control study to explore the risk factors for acquisition of leptospirosis in Surat city, after flood Bhardwaj Pankaj, Kosambiya JK, Desai VikasK Department of Community Medicine, Era's Lucknow Medical College & Hospital, Lucknow Code Number: ms08078 Abstract Background: Between August and November 2006, a population-based case control study was conducted to identify the probable risk factors for leptospirosis during flooding in Surat city.Materials and Methods: Sixty-two laboratory confirmed cases out of 129 suspected cases, and 253 age and sex matched fever and healthy controls were interviewed with the help of predesigned questionnaire. The association of risk factors with acquiring leptospirosis was assessed by adjusted OR with the help of logistic regression model to control confounders. Results: By univariate analysis, factors identified were, walking barefoot (OR = 10.34, 95% CI 5.09-21.31, P < 0.001), contact of injured part with flood water (OR = 9.65, 95% CI 4.81-19.61, P < 0.001), use of flood water for cooking (OR = 5.94, 95% CI 2.5-14.06, P < 0.001), for washing (OR = 4.21, 95% CI 1.74-10.17, P < 0.001), swimming in flood water (OR = 3.66, 95% CI 1.97-6.83, P < 0.001) and bathing (OR = 2.69, 95% CI 1.02-7.05, P < 0.001), trash within 500 m (OR = 4.31, 95% CI 1.41-14.76, P < 0.05) and rats in surroundings (OR = 11.05, 95% CI 3.18-45.9, P < 0.001). By multivariate analysis, four factors identified were, contact of injured part with flood water (Adjusted OR = 6.69, 95% CI 3.05-14.64, P < 0.001), walking barefoot (Adjusted OR = 4.95, 95% CI 2.22-11.06, P < 0.001), constant presence of rats in household (Adjusted OR = 4.95, 95% CI 1.53-16.05, p < 0.05) and spending more than four days in cleaning (Adjusted OR = 2.64, 95% CI 1.18-5.89, P < 0.05). Conclusions :Prompt and vigilant fever surveillance activities in pre-monsoon preparedness plan, intensive IEC messages, rodent control programs and improvement of environmental sanitary conditions may help to greatly reduce the incidence of leptospirosis. Keywords: Flood, leptospirosis, risk factor Introduction In recent years, clinicians and epidemiologists have given increasing attention to leptospirosis, with particular focus on two features: its epidemic potential and severe manifestations. It affects both humans and animals and it is emerging as an important public health problem in India. Leptospirosis has been recognized as an important occupational hazard of agricultural manual laborers, sewage workers, animal handlers, forestry workers, butchers and other outdoor workers who work in wet conditions. Recent outbreaks after flooding in urban areas of Surat, Mumbai, Manipal, the Andamans, and Chennai have raised new awareness concerning the risk of leptospirosis in disaster situations, as up to now disease is more endemic in rural areas. In urban areas of developing countries, a contaminated environment due to various factors such as inadequate drainage and sanitation facilities for both man and animals, presence of stray dogs, cattle, pigs, domestic rats and bandicoots, poor condition of slaughterhouses and people walking barefoot, contributes to the spread of this illness. Although annual rainfall-associated epidemics of leptospirosis in rural settings have long been recognized in South Gujarat, recent floods in Surat during August 2006 raised a need for exploring risk factors for acquiring leptospirosis in urban areas. This study attempts to explore the potential risk factors associated with the acquisition of urban leptospirosis, amenable to focused interventions, while designing control strategies for the future. Materials and Methods Study area This study was carried out in six (out of seven) zones of Surat city, namely Central, Katargam, Rander, Varachha, Udhna and Limbayat, from where most suspected cases of leptospirosis were admitted to different hospitals of Surat city. Study design It was a case control study Study period From August to November 2006 Methodology During August 2006, an outbreak of suspected leptospirosis was identified in Surat city. As per the State Health Department protocol, suspected cases of leptospirosis need to be urgently admitted to Government and private hospitals with facilities to manage such cases. Notification of leptospirosis cases to the State Health Authorities was made mandatory. A temporary epidemic control room was set up at New Civil Hospital, Government Medical College, Surat where every suspected case of leptospirosis had to be reported by all private and Government hospitals. A list of all suspected cases of leptospirosis was maintained and updated regularly with their full residential addresses along with probable diagnosis, signs and symptoms, laboratory investigations and outcome. Case definition for suspected case of leptospirosis Any person who presents with fever and has any one of the following symptoms: myalgia, conjunctival suffusion, anuria or oliguria and/or proteinuria, jaundice, hemorrhages with a history of exposure to flood water or mud is defined as suspected case of leptospirosis. Case definition for confirmed case of leptospirosis Suspected case of leptospirosis with paired sera samples showing positive results (ELISA IgM titer value > 20 IU) is defined as a confirmed case of leptospirosis. Selection of cases and controls Cases Subjects were selected from the list of suspected cases in the control room whose addresses could be located. Socio demographic information, clinical history and history of exposure to the floodwater were collected with the help of a pre-designed questionnaire. For all these subjects, first serum sample was taken at the time of admission to hospital. In the field, at the time of the interview, the second serum sample was collected. Finally, all those suspected cases both of whose sera samples turned to be positive, as per the definition of confirmed case of leptospirosis were taken as cases. Controls With each of the cases so identified, four age (± 5 years) and sex matched controls, two with fever and two asymptomatic, were selected. However, at the time of interview some of the persons with fever in the field demanded collection of their blood samples. Therefore, their samples were also collected and they were also enrolled as controls. For all these controls, socio demographic information and history of exposure to the floodwater was collected with the help of a pre-designed questionnaire. First serum sample was collected at the time of interview and the second serum sample was collected after 10-14 days. Those in whom both sera samples turned positive, were excluded from the list of controls. Undertaking of consent During the visit to the respondent′s house, detailed information about the study was given to the family to obtain their willingness to participate in the study and for providing sera samples with their verbal consent. Study tool A pre-designed pro forma was used to gather information. The data so obtained was as per the responses of the respondents along with visual inspection for the presence of trash and open sewer in close proximity to the residence. Statistical analysis After the completion of data entry, analysis was carried out using Epi_info version 6.04 software (Centers for Disease Control and Prevention, Atlanta, GA). The association of risk factors with occurrence of leptospirosis was first assessed by univariate analysis and odds ratios. To control for the confounding and to determine which exposures were most important in predicting seropositivity, a multivariable model was created. This way an adjusted odds ratio was calculated to get the most important risk factors associated with acquisition of leptospirosis by using a logistic regression model with the help of LIMDEP software. [1] Results This study reveals that the maximum flood level (mean HFL =12 ± 5 feet) was recorded in Katargam zone, which is a low-lying area of Surat city. During flooding, most affected people belonged to the economically and productive age group, where more than two thirds of the cases were of age group 15 to 34 years with mean age 29.06 ±11.09 years. It can possibly be attributed to more chances of exposure to flood water in this age group. Most cases belonged to Social Class III (51.6%). [2] Among cases and controls, the difference in socioeconomic status is not significant (P > 0.05). A majority of cases i.e., 38 (61.3%) spent four to seven days in cleaning activities after flooding. However a majority of controls 131 (52%) spent up to three days in cleaning activities. Among cases and controls, the difference in days spent in cleaning activities is statistically significant (P < 0.05). During this study it was observed that more than half of the cases were hospitalized three to five days after the onset of symptoms. Fever was observed as the most common symptom among these cases. Myalgia was present in 50% of cases. Approximately 15% of the cases present with jaundice. Conjunctival suffusion was seen as chief complaint in only 3% of cases. More than one third of cases stayed in hospital for 15 days and more. Discussion In the present study, it was found that of all zones the Central zone contributed the maximum number of cases 24 (39%), followed by Katargam 12 (19%) and Limbayat 10 (16%). The number of cases was more from Central, Katargam and Limbayat zones in comparison to Katargam zone despite the highest flood level (12±5 feet) being there. It was because a large proportion of labor groups who worked during cleaning activities after flood reside in these areas. Similar findings were reported by Akash Acharya et al. [3] who found that in Katargam area, the maximum level of floodwater was 20 feet. During the study, it was found that maximum time spent in cleaning of mud after flooding was in Katargam zone (mean 4.8 ± 2.5 days), as highest flood level was maximum in Katargam zone. A majority of cases i.e. 38 (61.3%) spent 4 to 7 days in cleaning activities after flood. However a majority of controls 131 (52%) spent up to 3 days in cleaning activities. Among cases and controls, the difference in days spent in cleaning activities is statistically significant (P < 0.05). Risk factors for occurrence of leptospirosis This population-based case-control study could identify various risk factors for acquisition of leptospirosis during flood. For the purpose of identifying risk factors for leptospirosis, all controls were compared with cases in analysis. Univariate analysis There is an established risk of acquiring leptospirosis among animal handlers in rural areas. As described previously, an effort was made to explore the possible association of livestock with occurrence of leptospirosis during floods. Among cases and controls the difference is not significant (P > 0.05). In a study, conducted by Misra [4] in Chikhli Taluka of district Navsari, Gujarat, the presence of livestock in affected villages was seen in 68.9% of families, where buffaloes were observed as one of the most commonly reared animal. In this study the difference in household ownership of livestock among cases and controls was not statistically significant. However in a study conducted by Jagadishchandra et al. [5] KMCH, in Manipal 55.95% of cases of leptospirosis gave history of contact with animals. The association was found to be significant (P < 0.05). In this study, walking barefoot in floodwater was found significantly associated with acquiring leptospirosis (OR = 10.34, 95% CI 5.09-21.31, P < 0.001). This may be due to flooding which prevents animal urine from being absorbed into the soil or evaporating, so leptospires pass directly into the surface waters or persist in mud. [7] Prolonged exposure of the skin to contaminated water provides an opportunity for invasion by leptospires. [6],[7] Similar findings were reported from a study conducted in Seychelles, by Bovet et al. [8] where the OR = 3, with 95% CI = 1.09-8.25. Bathing in floodwater was found significantly associated with acquiring leptospirosis (OR = 2.69, 95% CI 1.02-7.05, P < 0.001). Ashford et al. [9] also reported similar results in their study, in Nicaragua, where a significant association was seen between taking bath in floodwater and acquiring leptospirosis (P = 0.0039). The sighting of rats is very significantly associated with leptospirosis (OR = 11.05, 95% CI 3.18-45.9, P < 0.001). In a similar study, Sarkar et al.[10] reported that sighting rats in peri-domiciliary was a significant risk factor for leptospirosis (OR = 3.40, 95% CI = 1.74-11.78). In the present study it was found that out of 62 cases 58 (94%) and out of 253 controls 195 (77%) reported presence of accumulated trash in their surroundings. Living in close proximity to accumulated trash was found to be significantly associated with leptospirosis (OR = 4.31, 95% CI 1.41-14.76, P < 0.05). In a similar study by Sarkar et al.[10] living in close proximity to open sewers was found to be significantly associated with leptospirosis (OR = 5.07, 95% CI 2.04-12.64) while living in close proximity to accumulated trash was not found to be significantly associated with leptospirosis (OR = 1.53, 95% CI 0.7-3.31). Identification of residential proximity to places with accumulated trash and household rat infestation as risk factors indicates that much of urban leptospirosis during the epidemic season may be acquired through peri-domiciliary transmission. The established role of domestic rats as the principal reservoir (during urban epidemics) also supports this finding. Cases did not report direct contact with rats, suggesting that leptospiral transmission appears to occur primarily through exposure to an environment contaminated by the urine of rodent reservoirs. In the distant past, isolated cases of leptospirosis in adults due to exposure to rat urine have been reported in Mumbai. [11] Multivariate analysis A logistic regression model was applied to carry out multivariate analysis. A total of 14 factors [Table - 1] were assessed for their association with the outcome variable i.e. leptospirosis present or absent. The factors which are found to be independently associated with the occurrence of leptospirosis are as follows: Contact of injured part with floodwater The risk of occurrence of leptospirosis was found to be 6.69 times higher among those who had contact of their injured part with flood water compared to those who do not, provided other variables are adjusted (adjusted OR = 6.69, 95% CI 3.05-14.64, P < 0.001). Similar association was reported by Caste llanos et al. [12] during a study conducted in Mexico where the main risk factor related to leptospirosis infection during flooding was contact of subjects with floodwater when they had a skin cut or abrasion (OR 4·2; 95% CI 3·1-5·7). Walking barefoot When walking barefoot was tested, it was observed that the risk of occurrence of leptospirosis was found to be 4.95 times higher among those who walked barefoot in floodwater compared to those who did not (adjusted OR = 4.95, 95% CI 2.22-11.06, P < 0.001). In a study carried out in Barbados, Douglin et al. [13] reported that the most important risk factor for the occurrence of leptospirosis was walking through ponds or stagnant water after flooding (OR 25.62, 95% CL 2.89-1151.84). Rats constantly present in the household The risk of occurrence of leptospirosis was found to be 4.95 times higher among those who reported constant presence of rats in their household compared to those who did not, provided other variables are adjusted (Adjusted OR = 4.95, 95% CI 1.53-16.05, P < 0.05). In a similar study, Sarkar et al.[10] reported that sighting rats in peri-domiciliary was a significant risk factor for leptospirosis (adjusted OR = 4.49, 95% CI = 1.57-12.83). Days spent in cleaning activities The risk of occurrence of leptospirosis was found to be 2.64 times higher among those who spent more than four days in cleaning activities compared to those who did not (adjusted OR = 2.64, 95% CI 1.18-5.89, P < 0.05). Conclusion Findings from this study suggest that behavioral modifications, by reducing environmental exposure, may reduce the risk of leptospiral infection in this region. Most cases seemed to occur by cutaneous exposure of the legs while walking in stagnant water or moist soil. This implied that leptospira multiplied in the walking paths where water remained undrained for a period of two to three days after the rains was responsible for most cases. Most people in the state wore rubber chappals during the rainy season, which offered little protection against possible infection. Due to urban population growth and better job opportunities in urban areas, a large proportion of the population is bound to reside in urban slums. Ecologic studies of urban epidemics of leptospirosis identified that cases geographically clustered in these areas of poor sanitation and flooding during periods of heavy rainfall. [14],[15] During dry periods, high leptospira concentrations in the soil are limited to a few meters around waste accumulation sources. During floods, the infectious agent spreads and reaches distant areas under the impact of water. This same flood dilutes both the agent and also its infectivity at great distances from the source. This dispersion promotes the agent′s contact with population groups, i.e. individuals with no previous contact with the bacteria. Individuals living close to foci are believed to have more frequent contact with the agent, given the higher prevalence of infection there. Thus, a shift in seropositivity can be predicted in flood situations. The observations from this case-control investigation show that there are definable peri-domiciliary infrastructure deficiencies within urban settings that contribute to these outbreaks. These identified risk factors are conditions that are potentially correctable both by individuals and at the municipal and community level. The severe clinical outcomes of leptospirosis drain the country′s health resources. During this single outbreak in Surat city, more than 300 suspected cases of leptospirosis were hospitalized with many of them having complications like jaundice, acute renal failure, and bleeding diatheses necessitating intensive care monitoring and dialysis. Moreover, cases of severe leptospirosis identified by hospital-based surveillance are only a small fraction of all leptospiral infections. Severe disease is believed to represent 5-15% of clinical infections. [16],[17] Because urban epidemics of leptospirosis are characterized by high mortality, prevention and improved detection are required to improve clinical outcomes at the population level. In addition, rodent control programs must be targeted to decrease rodent populations in the peri-domiciliary and workplace environment in anticipation of annual periods of heavy rainfall. The utility of this model might be considered while giving IEC messages to the people, health workers, clinician and administrator. Appropriate health education messages and case definitions can be prepared using such models. Limitations of the study In the study, ELISA test instead of MAT is used as the confirmatory test for defining cases for our study. This is because the facility to carry out MAT test on all the samples is not available in Department of Microbiology, Government Medical College, Surat. Acknowledgment Dr Abhay Kavishwar, Associate Professor, Dept of Community Medicine, Government Medical College, Surat, and Dr Gagan Bihari Sahu, Assistant Professor, Center for Social Studies, Surat for their help in statistical analysis using LIMDEP software and Dr. Bharat Patel, Assistant Professor, Department of Community Medicine, Surat for manuscript review. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08078t1.jpg] |
| |||||||||


{kind=link}