 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
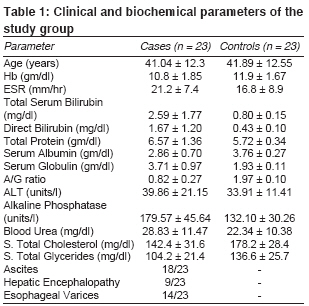
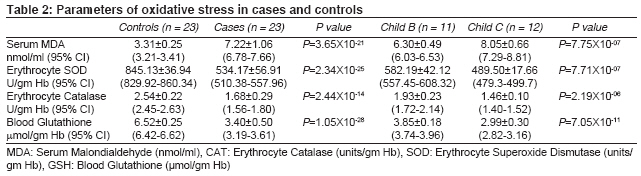
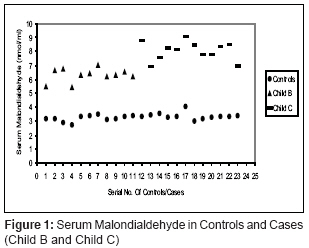
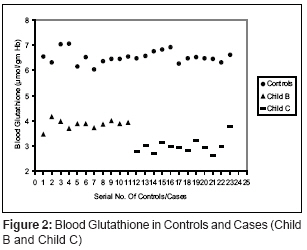
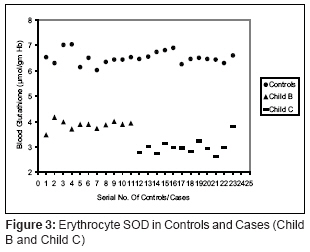
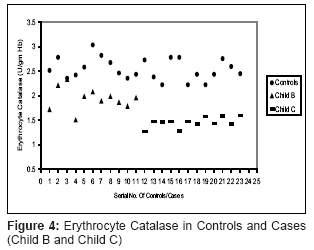
Indian Journal of Medical Sciences, Vol. 62, No. 11, November, 2008, pp. 444-451 ORIGINAL CONTRIBUTION Monitoring oxidative stress across worsening child pugh class of cirrhosis Bhandari Sumit, Agarwal MukulP, Dwivedi S, Banerjee BD Department of Medicine, University College of Medical Sciences and GTB Hospital, New Delhi-110 095 Code Number: ms08080 Abstract Context :Oxidative stress has been increasingly implicated in the pathogenesis and progression of cirrhosis. Keywords: Humans, cirrhosis, oxidative stress, reactive oxygen species, lipid peroxidation Introduction Oxidative stress is defined as an imbalance between pro-oxidant and antioxidant mechanisms in our body, the balance being tilted in favor of the former. [1] It has been unequivocally implicated in the pathogenesis and pathophysiology of many fibroprofilerative diseases such as atherosclerosis, glomerulonephritis, pulmonary fibrosis and cirrhosis. [2] Previous studies have demonstrated a correlation between hepatic and plasma glutathione. [3] Glutathione is a tripeptide synthesized in the liver which acts as an anti-oxidant. Erythrocyte antioxidant enzymes, such as superoxide dismutase (SOD) and catalase (CAT) have been found to be deranged in alcoholic liver disease, predisposing them to a hemolytic pattern. [4] Lipoperoxide concentrations, which signify increased free radical production, have been found to be elevated in liver and serum in patients with cirrhosis. [5] The present study was undertaken to assess the oxidative stress with respect to functional compromise of liver (as determined by Child-Pugh scoring), by measuring pro-oxidant (serum MDA) and antioxidant (RBC SOD and CAT, reduced glutathione-GSH) factors in patients with cirrhosis, and comparing them with corresponding values in age and sex matched controls. Materials and Methods After informed consent, 23 patients of cirrhosis (19 male, 4 female) aged between 24 to 65 years (median age 46 years), consecutively admitted in our department, entered the study. An equal number of age and sex matched healthy volunteers were recruited. Exclusion criteria were concurrent use of anti-oxidant drugs; co-existing diseases like diabetes mellitus (DM), chronic kidney disease (CKD); alcohol use within previous 2 weeks; gastrointestinal bleed or blood transfusion within previous 2 weeks. Diagnosis of cirrhosis was based on the clinical profile with biochemical and radiological investigations and a liver biopsy unless contraindicated. The predominant etiology of cirrhosis in 17 cases of cirrhosis was alcohol abuse, while chronic viral hepatitis was the cause in four cases, and two remained of cryptogenic origin. Eleven cases were cirrhosis belonging to Child′s grade B and 12 had Child′s grade C cirrhosis. Besides routine investigation, biochemical tests to measure serum MDA, RBC CAT and SOD, and blood GSH were done. Serum MDA level was measured as an index of lipid peroxidation using Satoh calorimetric method. [6] This assay is based upon the reaction of TBA (thiobarbaturic acid) with MDA, one of the aldehyde products of lipid peroxidation. The absorbance of the MDA-TBA adduct produced was measured at 532 nm spectrophotometrically. The erythrocyte SOD activity was determined by the method described by Marklund and Marklund, as modified by Nanda and Chatterjee. [7],[8] This method is based on the inhibition of pyrogallol auto-oxidation brought about by SOD. Erythrocyte catalase (CAT) activity was determined by the method of Sinha. [9] This is based on the principle that dichromate in acetic acid is reduced to chromic acid when heated in the presence of H 2 O, with the ultimate production of chromic acetate, which is measured at 570 mm. Reduced glutathione is measured by Teitze′s method [10] . This is based on the development of yellow color with DTNB (5, 5, dithiobis-2-nitrobenzoic acid), which is measured at 412 mm. Statistical analysis The cases were assigned a Child Pugh class. The continuous variables were recorded as a mean with standard deviation. The significance of difference between the various groups was calculated using the ANOVA-f test, followed by Tukey′s test to ascertain whether the differences between the various groups were clinically significant (P < 0.05). Results The clinical and biochemical parameters of the study subjects were as shown in [Table - 1]. All the cases had evidence of decompensation in the form of ascites and/or hepatic encephalopathy, reflecting the fact that cirrhosis goes largely undetected in initial stages in our country. The pro-oxidant and anti-oxidant markers in the blood of cirrhotics are shown in [Table - 2], with corresponding levels in controls. A further comparison reflecting the differences in these values in worsening cases (as determined by Child-Pugh scoring) is also shown. A significant increase in serum MDA value in cases was noted (P < 0.05). On further assigning the cases as per Child Pugh scoring, Child C cirrhosis had a worsening level of oxidative stress [Figure - 1]. A significant decrease in antioxidant markers, RBC CAT, SOD and blood GSH was noted. On grading the cases as per Child Pugh scoring, Child C had a significantly reduced level of antioxidant markers [Figure - 1],[Figure - 2],[Figure - 3],[Figure - 4]. Discussion Liver fibrosis was considered the result of repeated steatosis and chronic hepatitis until Lewis et al. hypothesized that the individual susceptibility of alcoholics to cirrhosis was due to variation in free radical scavenging enzymes and accumulated free radicals like superoxide. [11] The proposal that oxidative stress has a direct causative role in liver fibrogenesis was first put forth by Chojkier et al., who demonstrated (with cultured fibroblasts) the in vitro evidence of a possible molecular linkage between enhanced lipid peroxidation and induction of collagen gene expression. [12] The proposal was subsequently extended to the in vivo model when Houglum et al. established a close association between liver fibrosis induced by iron overload and protein adduct epitopes of MDA and 4-hydroxynonenal (HNE), another lipoperoxide aldehyde product. [13] Bedossa et al. have demonstrated the co-localization of increased collagen a-1 messenger RNA with carbon tetrachloride induced lipid peroxidation, by means of in situ hybridization and immunohistochemical studies in cultured rat hepatocytes. [5] Muraca et al. demonstrated that antioxidant supplementation was able to depress procollagen a-1 m-RNA over-expression. [14] A role of oxidative stress in the pathogenesis of chronic liver disease has been proposed by several authors using animal and human studies. [15],[16],[17] The aim of our study was to assess the changes, if any, in the levels of markers reflecting oxidative stress across worsening Child scores. Serum MDA was significantly elevated across worsening Child scores. Previous studies, in rat and micropig model of experimental liver cirrhosis induced by alcohol and iron, found increased level of MDA and HNE in the liver. [17],[18] Iron potentiated fibrogenesis was associated with intense and diffuse staining for MDA and HNE protein adducts. A significant increase in plasma TBARS has been noted in the plasma of 38 patients with cirrhosis by Yasa et al., with no significant difference between erythrocyte thiobarbituric acid reactive substances (TBARS) between controls and patients. [19] Significant increase in the level of plasma MDA in cirrhotics was noted by Nalini et al. [20] However, in a study by Clot et al., there were no significant differences between erythrocyte and plasma lipoperoxides in patients with cirrhosis and controls. [21] There was a significant decrease in erythrocyte SOD in our cases across worsening Child Pugh class. A similar trend has been noted in previous studies. [19],[20] However, Gerli et al., in a study involving 73 cirrhotics (22 Child A, 30 Child B, and 21 Child C) and 50 controls, demonstrated no significant difference between erythrocyte SOD among various groups. [4] The disparities between these studies may be explained by different biochemical methods applied and the acute condition of the patients, given the fact that Child Pugh class may vary if there is any precipitating factor such as pharmacological incompliance (with a substantial intra class variability in patient profile). Erythrocyte CAT was significantly lower in our cases, as compared to controls. A similar trend was noted by Gerli et al., with the decline in RBC CAT correlating well with the decline in liver function, as assessed by Child Pugh classification. [4] The level of GSH was reduced across worsening Child class of cirrhosis. A significant decline in RBC GSH was noted by various authors. [4],[20] It should be noted that a decline in RBC GSH correlates well with decline in blood GSH. It is also pertinent to note that investigators have shown that decrease in the level of GSH in blood reflects parallel decrease in level of GSH in the liver. [22] The biochemical pathways by which oxidative stress may cause cell injury are lipid peroxidation of membranes, oxidative modification of proteins and lesions in DNA. [1] Studies in intragastric ethanol fed rats have shown that the accumulation of MDA in the liver is associated with the development of antibodies recognizing protein MDA adducts. [23] Steward S et al. have further characterized peripheral blood mononuclear cell (PBMC) and antibody responses to human serum albumin (HSA) adducts to MDA. [24] They observed that alcoholic patients with cirrhosis had significantly higher cellular and humoral immune response to HSA-MDA adducts than controls and alcoholic patients without cirrhosis, implicating a role of cellular and humoral immunity in oxidative stress induced cirrhosis. Hence, various mechanisms by which oxidative stress may play a role in the pathogenesis and progression of chronic liver disease are stimulation of hepatic stellate cells, Kupffer cells, immune system and apoptosis. [25],[26] The chief drawback in our study is a small sample size. A correlation between oxidative stress in blood and liver biopsy specimens was desirable, but for the fact that there were obvious contra-indications to perform a liver biopsy (such as a deranged coagulation profile, ascites) in many patients. Being a cross-sectional study, sequential samples were not taken. However, care was taken to rule out any precipitating factor like GI bleed, acute infection which could influence oxidative stress, and the cases were relatively stable within their calculated Child-Pugh class. Conclusions Our study shows that Child class C cirrhosis has greater oxidative stress than Child class B cirrhosis suggesting that greater liver damage is associated with more oxidative stress. This needs to be corroborated in further studies with a larger sample size along with serial assessment of oxidative stress and its correlation with the (histopathological) progression of cirrhosis. This can also serve as a background for assessing the role of anti-oxidants in preventing the progression of cirrhosis. Acknowledgment We would like to acknowledge the highly co-operative and motivating role of the patients and volunteers without whom this study would not have been possible. We would also like to thank the Departments of Medicine and Biochemistry of University College of Medical Sciences and GTB Hospital, New Delhi where this study was conducted.References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08080f2.jpg] [ms08080f1.jpg] [ms08080t2.jpg] [ms08080t1.jpg] [ms08080f4.jpg] [ms08080f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}