 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
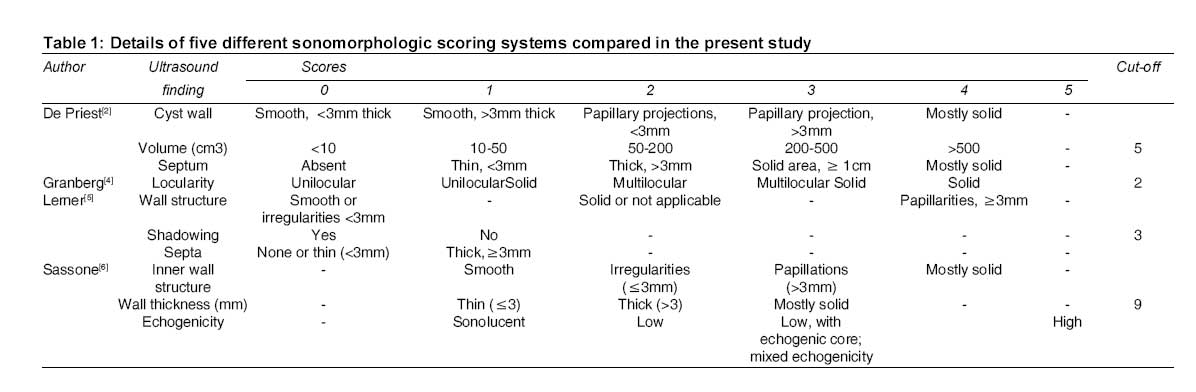
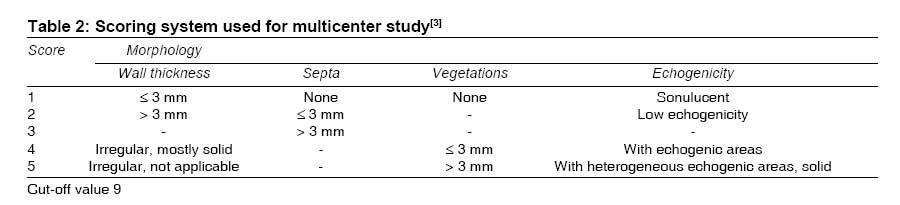
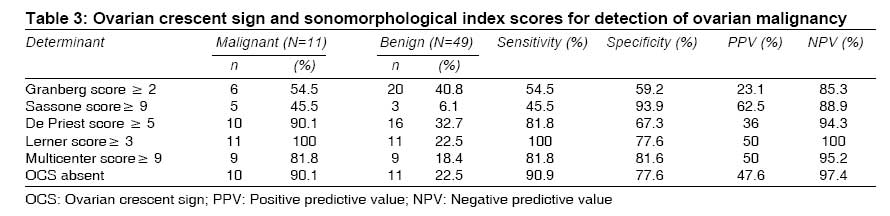
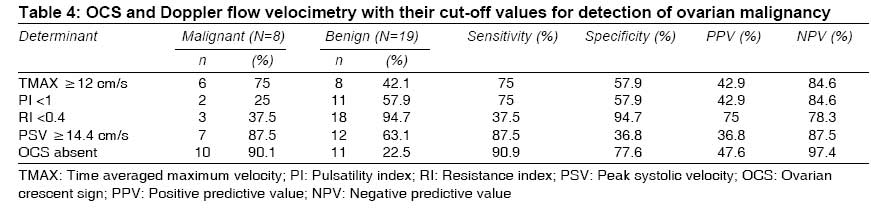
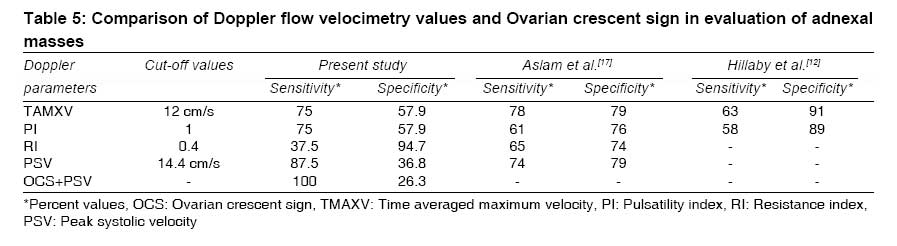
Indian Journal of Medical Sciences, Vol. 62, No. 12, December, 2008, pp. 477-483 ORIGINAL CONTRIBUTION Ovarian crescent sign and sonomorphological indices in preoperative determination of malignancy in adnexal masses Kalghatgi-Kulkarni Kiran, Kushtagi Pralhad Department of Obstetrics-Gynecology, Kasturba Medical College, Manipal University, Manipal- 576104 Code Number: ms08087 Abstract Objective :To compare the value of ovarian crescent sign (OCS) and various sonomorphologic scoring systems in consolidating pre-operative suspicion of ovarian malignancy in adnexal masses. Keywords: Adnexal mass, ovarian cancer, ovarian crescent sign, sonomorphological index, ultrasonography Introduction Over the decades various methods to identify the nature of adnexal mass pre-operatively have been tried. There are no universally accepted criteria for distinguishing between benign and malignant conditions on the basis of ultrasound findings. Several systems for classifying and scoring the abnormalities in the form of morphological index have been described. [1],[2],[3],[4],[5],[6],[7] Risk of malignancy index using menopausal status, CA125 value and morphological scores have been proposed. [8],[9],[10] All these methods use complex calculations and study multiple parameters to develop a score. The importance given to the parameters is also variable. Even Doppler flow studies have failed to provide more useful diagnostic information than transvaginal sonography or estimation of CA 125. [11] The value of detection of normal ovarian tissue in the adnexal masses, the ovarian crescent sign (OCS), is highlighted as a single ultrasound parameter in prejudging the nature of adnexal mass as benign or malignant. [12] This appears simple, immediate, and comparable to other methods. It does not involve any calculations or multiple parameters. It has been reported that absence of OCS is a more sensitive indicator of malignant nature than the risk of malignancy indices. [13] It has even been used as one of the morphological features to discriminate borderline from the invasive malignant lesions. [14] Since all these reports [12],[13],[14] were from one group and from one region, this study was planned to replicate the utility of OCS in other regions and the present communication attempts to validate OCS in comparison with other reported sonomorphologic scoring systems and Doppler flow evaluation in suspecting malignant nature of the adnexal mass. Materials and Methods A prospective study was carried out in 60 women with adnexal mass requiring surgery attending gynecology service. Excluded were cases reporting with a proven diagnosis of malignancy. The study was approved by the Hospital Ethics Committee. Ultrasound examination was done by a gynecologist trained in ultrasonography. The various parameters noted were bilaterality (unilateral or bilateral), wall thickness, inner wall structure, locularity, septal thickness (if multilocular), echogenicity, shadowing, tumor volume (pi /6 x d1 x d2 x d3), ascites, intra-abdominal metastasis and ovarian crescent. Doppler flow velocimetric studies in 32 cases were carried out by a designated radiologist. Time averaged maximum velocity (TAMXV), peak systolic velocity (PSV), end diastolic velocity (EDV), pulsatility index (PI) and resistance index (RI) were noted. Sonomorphological scores were calculated as per the scoring systems described by De Priest et al., [2] Granberg et al., [4] Lerner et al., [5] Sassone et al.[6] [Table - 1] and multicenter scoring system [3] [Table - 2]. Criteria used to identify ovarian crescent were presence of hypo-echogenic tissue with or without ovarian follicles (i) located adjacent to the cyst wall (ii) not separated from the cyst by applying a moderate amount of pressure and (iii) enclosed within the ovarian capsule encircling the tumor. [12] Sonomorphological scores and Doppler flow velocimetry values were compared with presence or absence of OCS in reference to histopathologic diagnosis of malignancy of the mass. All statistical analyses were performed using SPSS software (Statistical Package for Social Sciences; SPSS Inc., Chicago, IL, USA), version 11. Sensitivity, specificity, positive predictive value and negative predictive value were calculated. The chi-square test was applied to test the significance of differences between proportions. A probability (P) value of < 0.05 was considered as significant. Results Eleven of 60 specimens (18.3%) were reported as having malignant disease. Except a case of carcinoid, all others were epithelial malignant tumors. Among 49 of the benign group, epithelial ovarian cystic tumors comprised 42.8% (13 mucinous and 8 serous cystadenomas). Endometriotic lesions were the next common diagnosis (in 10 cases, 20.4%) followed by 6 cases of dermoid, 5 follicular and 2 paratubal cysts. There was a case each of fibrothecoma, ovarian abscess and hydrosalphinx apart from two cases of subserous fibroid. The mean age of cases studied was 41.4 + 14.5 years with the youngest aged 19 and the eldest, 78 years. Although not significant (P = 0.366), the proportion of cases with malignancy was higher in women beyond 50 years of age. There were 41 cases who were premenopausal and the proportion of malignant adnexal masses was similar in pre- and post-menopausal groups (6 of 35 and 5 of 19 cases, P=0.277). At ultrasonography, OCS could be identified in 65% of cases (39 of 60) scanned. The visualization rate was significantly lower in postmenopausal than premenopausal women with benign adnexal masses (OCS seen in 29 pre- and 9 postmenopausal; OCS absent in 6 pre- and 5 postmenopausal; P = 0.023). The OCS was not seen in 10 of the 11 cases with malignancy. The lone case, in whom it was positive, was a stage 2 serous cystadenocarcinoma of borderline malignancy. The ovary was grossly normal looking. OCS was not visualized in 11 benign cases (four cases of large mucinous cystadenomas, two chocolate cysts, one case each of ovarian abscess, fibroid, ovarian fibrothecoma, cystic teratoma, and a multilocular papillary serous cystadenoma). Crescent sign was thus found to have high sensitivity (90.9%) and high negative predictive value (97.4%) in prejudging the adnexal masses. In comparison, the studied sonomorphological scoring systems were either sensitive or specific and did not appear to be better than OCS. Among them, Lerner′s was very sensitive (100%), while Sassone scoring system was more specific (93.9%). Scoring system proposed following a multicenter study was more balanced (sensitivity 81.8% and specificity 81.6%) [Table - 3]. Thirty-two cases were subjected to Doppler velocimetry studies, of which five did not show any vascularity. These cases were excluded from the analysis. The sensitivity, specificity, positive and negative predictive values for OCS were calculated for the 27 cases who had Doppler evaluation. Establishing cut-off level for end diastolic velocity was out of the scope of this study and there was a large overlap between the values in the benign and malignant lesions (range in benign lesions 2.2 to 20 cm/s; in malignant lesions 3.3 to 26 cm/s). Among the Doppler parameters, peak systolic velocity (PSV) had a higher sensitivity compared to the rest, though specificity (36.8%) was very much lower [Table - 4]. Discussion Since the report by Hillaby et al.[12] that the presence of normal ovarian tissue adjacent to an ovarian cyst is a useful morphological feature in the pre-operative differential diagnosis of adnexal lesions, they have further explored its utility and efficacy. [13],[14] OCS was found to be a better discriminator of malignancy in adnexal mass than tumor morphology (tumor volume and papillary proliferations), Doppler indices (PI and TAMXV) and CA 125 estimations leading to the conclusion that presence of OCS with a sensitivity of 96% and specificity of 76% may help to exclude an invasive ovarian malignancy. [12] The present study too obtained similar results of high sensitivity (90.9%) and high negative predictive value (97.4%) for OCS. In cases where Doppler parameters were available, OCS was found to be more sensitive, specific and predictive. Other studies [12],[15] have obtained comparatively higher specificity of 79-91 and 76-89% but poorer sensitivity of 63-78 and 58-61%, for TMAXV and PI, respectively, than our results[Table - 5]. All said, these sophisticated evaluations have not helped much. [11] And OCS seems a better tool in this respect. OCS had compared favorably with risk of malignancy index (RMI) [13] in identifying invasive and noninvasive tumors. Although RMI system divides mass into unilocular and complex on ultrasound appearance which can be identified with minimal ultrasound skills, waiting for CA 125 values and different versions of RMIs giving different importance to menopausal status and ultrasound parameters do not make RMI that simple. [8],[9],[10] The authors also found that OCS as discriminator for adnexal masses was more sensitive than different versions of RMI. Since specificity was comparatively lower, it was opined that OCS has equal utility if not better than RMI. It was also found that combining OCS with RMI did not have added benefit in the pre-operative diagnosis. [16] Though not adopted widely in routine clinical practice, to improve the accuracy of ultrasound diagnosis a number of morphological scoring systems incorporating systematic examination of a number of different tumor features on ultrasound scan have been designed. [2],[3],[4],[5],[6],[7] Assessment of tumor morphology by experienced operators has been considered superior to complex diagnostic models such as logistic regression and artificial neural networks devised to improve ultrasound diagnosis of ovarian cancer. [15],[17] These reported ultrasound studies using descriptive parameters, or the ones developed as scoring systems, use meticulous analysis of minute details of tumor architecture and/ or complex ultrasound tests such as Doppler assessment of intra-ovarian blood flow which require a trained sonologist. In the small group of 60 cases studied, some interesting observations were made that need to be explored. Malignant ovarian tumors were finding prevalence in younger women. The mean age of the cases admitted with adnexal mass in the present study was 41.4 + 14.5 years (range 19-78 years), comparable to the group studied by Alcazar et al. [7] However, women with malignant adnexal mass were younger by a decade when compared to the report by Hillaby et al. [12] The detectability of ovarian crescent was difficult in menopausal women probably attributable to the lesser ovarian volume in them. The relative ovarian volume in pre- and postmenopausal women has not been studied. Probability of failure to identify normal ovarian tissue in large ovarian lesions although benign as in four cases of mucinous cystadenomas should also be kept in mind. In them ovarian tissue may be compressed and pushed laterally or thinned out and spread. Ovarian crescent could be identified even if mass is malignant when destruction of ovarian tissue is not extensive as in one case of stage 2 borderline tumor whose ovary was grossly normal looking. Finding OCS in 75% of serous borderline tumors and none in invasive group, Yazbek et al. [14] opined that it is practical to use OCS for excluding invasive cancer. It is said that OCS is always easily detectable in endometriotic cysts; [12] in two of the ten cases we missed the finding. In both these cases chocolate cysts were within the ovary and ovarian tissue was destroyed. While ultrasound recording by one gynecologist trained in ultrasound who was not involved with the study can be taken as a strong point of the communication, inability to get Doppler studies done for all the cases and unavailability of data regarding ovarian volumes in pre- and postmenopausal women without adnexal mass remain the weaknesses. But still, by virtue of being very simple and not requiring expertise in gynecologic ultrasonography, OCS is a handy parameter to look for and it has the potential to develop as a tool in triaging adnexal masses for referral to specialty centers. It can be concluded that absence of ovarian crescent sign in a case with adnexal mass is a sensitive marker for malignancy with a dependable specificity. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08087t5.jpg] [ms08087t1.jpg] [ms08087t2.jpg] [ms08087t3.jpg] [ms08087t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}