 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
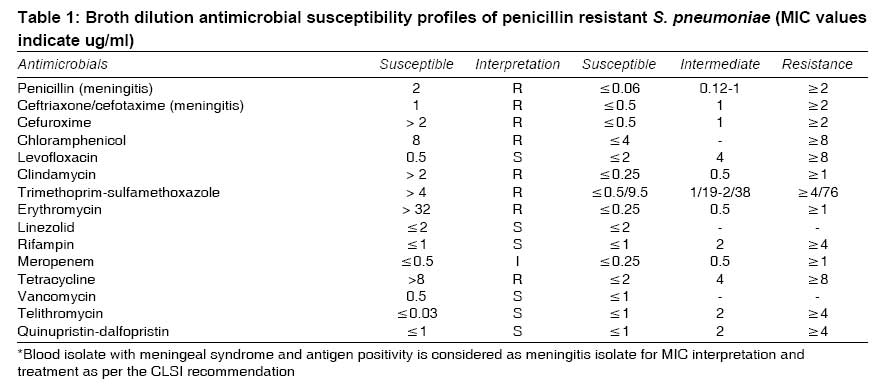
Indian Journal of Medical Sciences, Vol. 62, No. 12, December, 2008, pp. 492-495 Case Report Increasing invasive disease due to penicillin resistant S. pneumoniae in India Balaji Veeraraghavan, Thomas Kurien, Joshi HariHar, Beall Bernard Department of Clinical Microbiology, Christian Medical College, Vellore Code Number: 08087 Abstract S. pneumoniae continues to be a major cause of invasive disease worldwide with considerable mortality and morbidity. Here we report the emergence of penicillin intermediate resistance to S. pneumoniae in India, which may predispose for an increased incidence of invasive pneumococcal disease in both children and adults with multi-drug resistance profile resulting in clinical failure. Keywords: India, penicillin resistance, S. pneumoniae Introduction Streptococcus pneumoniae is a major cause of morbidity and mortality in India, especially in children, the elderly and immunocompromised individuals of all age groups. Penicillin has been an effective and affordable antibiotic for the treatment of invasive pneumococcal disease (IPD). Notably, among the Asian countries, India had the lowest percentage of penicillin intermediate resistance to S. pneumoniae (PIRSP) and virtually no complete penicillin resistance in IPD isolates. [1],[2],[3] Here, we report with great concern, the emergence of penicillin resistant S. pneumoniae (PRSP) in India.Case Report A 26-year-old male presented with recent history of fever, headache, left-side earache and altered sensorium. On examination, signs of meningeal irritation with bilateral sixth nerve palsy were observed. ENT examination revealed acute otitis media. Cerebrospinal fluid (CSF) indices were suggestive of acute pyogenic meningitis with total CSF leukocyte counts of 2400 /µl (70% PMN), glucose 30 mg/dl and protein 240 mg/dl. The CSF Gram stain and culture were negative, but positive by immuno chromatographic test (ICT), S. pneumoniae Binax ® NOWT. Contrast enhanced CT of the brain did not show any focal lesions. The patient was treated with high dose crystalline penicillin. His blood culture subsequently grew S. pneumoniae, which was found resistant to oxacillin by the disc diffusion test. The penicillin minimum inhibitory concentration (MIC) was 2 µg/ml by broth dilution method. He was treated with intravenous ceftriaxone and vancomycin for a total duration of ten days. His condition improved dramatically and he became afebrile. He was asymptomatic at discharge. Eight months later he developed meningitis again and the CSF grew S. pneumoniae. ENT examination revealed a congenital anomaly for which he subsequently underwent surgery. The resistant blood isolate from patients with meningeal symptoms and antigen positive is considered a meningitis isolate for MIC interpretation and treatment as per the standard recommended practice. This isolate was characterized at the Centers for Disease Control and Prevention (CDC, Streptococcus Laboratory, Atlanta, USA). Antimicrobial susceptibility profile demonstrating multidrug resistance (MDR) [Table - 1] was determined by the broth dilution method and interpreted using the 2007 CLSI guidelines. [4] CDC considers MDR to S. pneumoniae when an isolate is non-susceptible to three of the following antibiotics: penicillin, erythromycin, trimethoprim-sulfamethoxazole, tetracycline, chloramphenicol, clindamycin, rifampin, and levofloxacin. This study isolate belonged to serotype 23F and multilocus sequence type (MLST) ST1476, and is a single locus variant of ST81 from the internationally disseminated MDR clone Spain23F-1 [Table - 2], posted in http://www.sph.emory.edu/PMEN/index.html . Discussion A well-known and widespread study conducted in Asia by ANSORP [1],[2],[3] (Asian Network for Surveillance of Resistant Pathogens) reported the highest prevalence of penicillin resistance in isolates from Vietnam (71.4%), followed by Korea (54.8%), Hong Kong (43.2%), and Taiwan (38.6%) with virtually no resistance observed in India (0%). The prevalence of erythromycin resistance was also very high in Vietnam (92.1%), followed by Taiwan (86%), Korea (80.6%), Hong Kong (76.8%), China (73.9%) and India (1.3%) in 2004. Thereafter, a clear and distinctive increase in the prevalence and antimicrobial resistance rates among S. pneumoniae isolates is continuously being published independently in many Asian countries. At Christian Medical College, Vellore, antimicrobial resistance to S. pneumoniae was being monitored continuously for two decades. Until late 1995 all the S. pneumoniae isolated was consistently susceptible to penicillin. Thereafter the proportion of PIRSP has been steadily increasing over the last decade. This includes 3.8% in 1996-97 among the clinical isolates [1] 12.8% among carriage isolates; [2] 7.8% in 2000 - 2001 among the clinical pathogens [3] ; and 1.48% in 1993-97 among clinical isolates. [5] Nevertheless, in 1999, [6] a 4.6% (n = 25) which included eight CSF isolates with intermediate resistant to penicillin (0.125-1.0 µg/ml) was reported. Likewise, point prevalence studies reported by other groups in India also had similar trends. This includes 7.3% (n = 11) isolates; [7] 15.4% (n = 2) [8] and 25% (n = 3); [9] 20% (n = 30) with 0.12 - 1 µg/mL and 2 µg/mL of 26 and four respiratory isolates respectively. [10] However, in 2008, the Clinical Laboratory Standards Institute (CLSI) after re-evaluating with the more recent clinical data published new MIC penicillin break points for S. pneumoniae. [11] This latest recommendation for the first time is based on the clinical syndrome and route of penicillin administration. Further, this MIC break point tends to change the earlier findings of PIRSP, published in the literature up to early 2008, to a much lower percentage for non meningitis isolates [1],[2],[3],[5],[8],[9],[10] and higher percentage of complete penicillin resistance to meningitis isolates. [6],[7] However, this particular study isolate antimicrobial MIC break point interpretation remains valid as it conforms to CLSI 2008 recommendation also. The emergence of PRSP may be due to extensive use of amoxicillin for the treatment of upper respiratory tract infections in the community. The appearance of resistant S. pneumoniae may be related to clonal penetration by resistant strains from neighboring countries. It is important to note that Sri Lanka reports much higher levels of penicillin resistance (> 90% in 2006-07- unpublished data; Southeast Asia Pneumococcal Network Alliance). In this setting Tamil Nadu may be a natural site where early penetration is likely to occur. The emergence of resistant isolates can be effectively reduced by widespread pneumococcal vaccination. The available 23-valent pneumococcal polysaccharide vaccine for adults covers more than 80% and 7-valent pneumococcal conjugate vaccine for children covers around 50% of the serotypes identified in an Invasive Bacterial Infection Surveillance (IBIS) study (unpublished data). Further, there is an urgent need to establish a molecular pneumococcal surveillance network in India to monitor the antimicrobial resistance, serotype distribution and MLST profile for preventive strategies. This case report highlights the following: The emergence of PRSP may predispose for an increased incidence of IPD especially in children with MDR profile resulting in clinical failure. This finding signals the presence of the well-known rapid disseminating Spanish 23F penicillin-resistant clone in India Acknowledgment We acknowledge the use of the pneumococcal multilocus sequence type database (Imperial College, London, funded by Wellcome Trust). References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08089t1.jpg] [ms08089t2.jpg] |
| |||||||||


{kind=link}
{kind=link}