 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
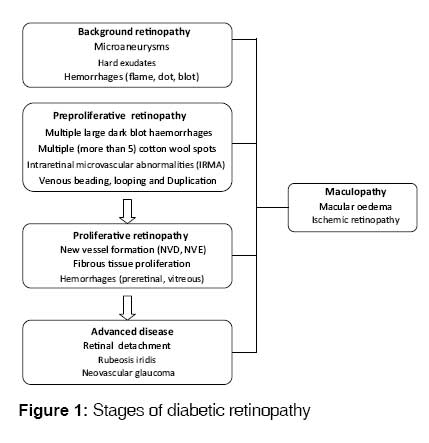
Indian Journal of Medical Sciences, Vol. 62, No. 12, December, 2008, pp. 500-519 Practitioners section Diabetic retinopathy: A comprehensive review Shah ChiragA Department of Life Sciences, Accelaire Consulting and Research Pvt. Ltd., Pune-411 037 Code Number: ms08093 Abstract Diabetic retinopathy (DR) remains one of the leading risk factors and causes of blindness worldwide. Tight metabolic and blood pressure control has been shown to significantly decrease the risk of development as well as progression of retinopathy and remains a cornerstone in the medical management of DR. Laser photocoagulation and vitrectomy are important tools for preventing severe visual loss from sight-threatening DR and its complications. New pharmacological therapies to target the underlying biochemical mechanisms that cause DR are also being evaluated in order to overcome the limitations of current treatment modalities. In this context, the role of protein kinase C inhibitors, intravitreal injections of steroids, vascular endothelial growth factor inhibitors, angiotensin converting enzyme inhibitors such as candesartan, and growth hormone inhibitors is promising. Although treatment can help prevent blindness in a majority of cases, the key variable in the success of therapy lies in identifying patients with retinopathy before their vision is affected. This calls for timely eye examination of diabetic patients. The present article is a comprehensive review of DR with special emphasis on its pathophysiology and management aspects. Keywords: Diabetic retinopathy, management, pathophysiology Introduction Diabetic retinopathy (DR) is one of the commonest and easily demonstrable examples of microvascular damage that diabetes inflicts throughout the body. DR is among the leading causes of blindness in people of working age, affecting both the genders equally. [1],[2] Patients with type 1 diabetes may show evidence of retinopathy as early as 5 years after the onset of diabetes, and almost all patients will show varying degrees of retinopathy 20 years after the onset of diabetes. Background retinopathy may even be present at the time of diagnosis of type 2 diabetic patients, consistent with the usually long duration of subclinical hyperglycemia in such patients and more than 60% of type 2 diabetic patients will have some degree of retinopathy after 20 years of onset of diabetes.Etiology and Pathogenesis Various studies have shown that chronic hyperglycemia, hypertension and hyperlipidemia contribute to the pathogenesis of DR. Hyperglycemia damages retinal vasculature in several ways and progression of DR is generally related to the severity and duration of hyperglycemia. The exact mechanism by which raised glucose levels lead to vascular disruption seen in retinopathy is poorly defined. However, various biochemical pathways have been suggested to demonstrate correlation between hyperglycemia and microvascular complications of retinopathy. Among these pathways, increased activity of protein kinase C (PKC) and glycation of key proteins that lead to formation of advanced glycation end (AGEs) products are more important than polyol accumulation or oxidative stress. Role of PKC activation The increased activity of various PKC isoforms plays an important role in the pathogenesis of DR. [3],[4],[5] Activation of PKC causes cellular changes, leading to enhanced permeability of retinal vasculature, alterations in retinal blood flow, basement membrane thickening and cellular signaling by vascular endothelial growth factors (VEGFs) leading to ocular neovascularization. [6],[7] Role of AGEs Increased blood glucose concentration in diabetes can lead to formation of AGEs by non enzymatic binding of glucose to protein side chains. [8] Animal studies have demonstrated that accumulation of AGEs is associated with microaneurysm formation and pericyte loss whereas animals treated with AGE formation inhibitor (aminoguanidine) show reduced retinal damage. [9],[10] Role of polyol accumulation Experimental studies have demonstrated that accumulation of polyol in animals is associated with changes similar to those seen in DR in humans. [11],[12] In the presence of increased polyol concentrations, hyperglycemia of diabetes leads to high intracellular sorbitol concentrations through enzymatic activity of aldose reductase. This increase in sorbitol concentration has been hypothesized to cause osmotic damage to vasculature of retina. [13] Oxidative damage Hyperglycemia of diabetes and other biochemical pathways described above can lead to formation of reactive oxygen species (ROS) (free radicals) that leads to oxidative stress and damage to retinal vasculature. [14] Further, normalization of glucose-induced superoxide production has been shown to block at least three independent pathways of hyperglycemia- induced vascular damage. [15] Animal and human studies have also suggested that antioxidants such as vitamin E may prevent some of the vascular dysfunction associated with diabetes. [16],[17],[18] Role of Growth factors Understanding of the biochemical pathways underlying DR have clearly demonstrated the important role of a number of growth factors (vascular endothelial growth factor (VEGF), growth hormone, insulin-like growth factor-1, PKC, transforming growth factor-β and pigment epithelium derived factor) in the development of structural changes in the retinal vasculature (increased retinal vascular permeability, retinal ischemia, neovascularisation) and progression of DR. [19],[20],[22] Clinical Stages of Diabetic Retinopathy The retina is particularly vulnerable to microvascular damage in diabetes due to its high metabolic and oxygen demands and its dependence on an intact blood-retinal barrier. Damage is caused by both microvascular leakage from breakdown of the inner blood-retinal barrier and microvascular occlusion both of which can be distinguished from each other by fluorescein angiography. The stages of DR are summarized and shown in [Figure - 1]. Background retinopathy Individual lesions of background retinopathy may appear and regress but their total density tends to increase with lengthening duration of diabetes. Vision is not damaged unless maculopathy coexists; over 50% of patients do not progress beyond this stage. Microaneurysms are outpouchings of capillaries and are among the first clinically detectable signs of retinopathy. [23] They arise due to ballooning of weakened capillary walls or endothelial buds attempting to revascularize ischemic retina. They appear as tiny red dots, commonly temporal to the macula. Although microaneurysms are not fixed features and may even disappear, sudden appearance of numerous microaneurysms is an indication of worsening retinal ischemia. Hard exudates are the result of precipitation of lipoproteins and other circulating proteins through abnormally leaky retinal vessels. They appear as yellow lipid deposits with a waxy or shiny appearance and may form a circinate pattern around foci of leaking capillaries. Hard exudates encroaching upon the macula may affect the vision. [23] Hemorrhages occur due to rupture of weakened capillaries Small dots or larger blot hemorrhages are present within the densely packed deeper layers of retina while hemorrhages occurring in the superficial nerve fiber layer appear flame shaped. Maculopathy Maculopathy is a disease of macula and can accompany any stage of DR including background retinopathy. Maculopathy is a serious condition and may affect central vision. [24] It is characterized by macular edema and ischemic maculopathy. Macular edema is due to extravasation of plasma proteins due to damage of blood-retinal barrier. Clinically significant macular edema is defined as any one of the following:
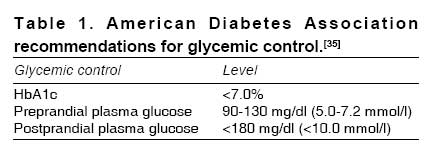
A substantial proportion of patients with clinically significant macular edema will show serious visual loss, highlighting the importance of treatment of this condition. [23] Ischemic maculopathy arises due to extensive microvascular occlusion and may cause severe loss of central vision. [24] Preproliferative retinopathy [23] This stage is characterized by worsening retinal ischemia, which may lead to formation of new vessels (neovascularization). It is characterized by the presence of one of the following:
Proliferative retinopathy This stage is characterized by new vessel formation which appears as arcade of abnormal structures commonly arising on the optic disc (new vessel disc or NVD) or elsewhere on the retina (new vessel elsewhere or NVE). Fibrous tissue and hemorrhages may also accompany. Abnormal new vasculature may threaten vision due to complications such as retinal detachment, hemorrhage and glaucoma. NVD carries a worse prognosis than NVE and if left untreated often leads to vitreous hemorrhage and increases chances of blindness. [23] Advanced eye disease This stage represents advanced retinal damage that leads to blindness in the absence of intervention. This stage is characterized by vitreous hemorrhage, progressive fibrovascular proliferation, retinal detachment, rubeosis iridis and neovascular glaucoma which may lead to a painful blind eye. [23] Important Management Aspects in Diabetic Retinopathy Although specific treatment modalities for retinopathy threatening vision have improved over years of clinical and research experience, importance of preventive measures (tight glycemic and blood pressure (BP) control, smoking cessation, regular eye screening) cannot be underestimated. Routine comprehensive eye evaluation helps to detect early treatable stages of DR which are frequently asymptomatic. Comprehensive eye examination is recommended within 3 to 5 years of disease onset in type 1 diabetic patients aged 10 years or older and immediately after diagnosis in type 2 diabetes. Diabetic patients without evidence of retinopathy should undergo eye examinations every year to detect its emergence. For patients with moderate-to-severe preproliferative disease, more frequent eye examinations are necessary to determine when to initiate therapy. [25] Importance of glycemic control Preliminary observational studies [26],[27] as well as large randomized controlled trials (RCTs) have shown a direct and consistent relationship between HbA1c (glycated hemoglobin) level and the incidence of DR. Effective glycemic control has been demonstrated to reduce both the incidence and progression of DR. The Diabetes Control and Complications Trial (DCCT) randomized patients (n = 1441) with type 1 diabetes to receive intensive glycemic or conventional therapy with the objective to investigate whether this would prevent or delay the progression of early preproliferative retinopathy and whether tight glycemic control could prevent the progression of early retinopathy to clinically more advanced forms. Conventional treatment comprised one to two daily injections of insulin, without adjustment in daily insulin dose while intensive treatment consisted of three injections of insulin or insulin by an external pump with the goal of achieving normal glycemia. Results of over 6.5 years of follow-up showed that, compared to conventional treatment group (median HbA1c, 9.1%), incidence of DR reduced by 76% (P < 0.002) and progression of DR by 54% (P < 0.011) in the intensive treatment group (median HbA1c, 7.2%). Similar beneficial effects of intensive therapy were evident in subgroups by age, sex, percentage of ideal body weight, duration, level of retinopathy, BP, clinical neuropathy, albuminuria and baseline HbA1c level. Even in the long term, the rate of DR progression in the intensively treated group remained significantly lower than in the conventional group. [28],[29],[30],[31],[32] Findings of DCCT highlighted the importance of instituting tight glycemic control early in the course of diabetes. The results of DCCT were further confirmed by the UK Prospective Diabetes Study (UKPDS). The UKPDS randomized 3867 newly diagnosed patients of type 2 diabetes to either conventional therapy or an intensive treatment with sulfonylurea or insulin. [33] Over 10 years′ follow-up, a 11% reduction in HbA1c was observed in the intensive group compared with the conventional group. Further, the risk for any diabetes-related end point (sudden death, death from hyperglycemia or hypoglycemia, fatal or nonfatal myocardial infarction, angina, heart failure, stroke, renal failure, amputation [of at least one digit], vitreous hemorrhage, retinopathy requiring photocoagulation, blindness in one eye, or cataract extraction), any diabetes-related death (death from myocardial infarction, stroke, peripheral vascular disease, renal disease, hyperglycemia or hypoglycemia, or sudden death) and all-cause mortality was 12% (95% CI 1-21, P = 0.029), 10% (95% CI 11 to 27, P = 0.34) and 6% (95% CI 10 to 20, P = 0.44) lower in the intensive therapy group respectively compared to conventional treatment group. Intensive therapy reduced microvascular end points by 25% (95% CI, 7-40%) and need for laser photocoagulation by 29%. Paradoxically, intensive glycemic control as highlighted by DCCT and UKPDS may provoke a transient deterioration in retinopathy with worsening of the background condition. The acute lesions in such adverse reactions typically resolve and overall long-term outcome is improved with good glycemic control. Further, a meta-analysis of 14 RCTs, [34] including the DCCT, indicated that intensive treatment may also be associated with a 3-fold increased risk of hypoglycemia and 70% higher risk of ketoacidosis as compared with conventional treatment. In the light of this discussion it is desirable to individualize the glycemic targets, as excessively stringent glycemic target (HbA1C < 6%), may increase risk of hypoglycemia. Similarly, certain populations (children, pregnant women, patients with severe or frequent hypoglycemia and elderly) may require special considerations. The American Diabetes Association′s recommendations [35] for glycemic control are presented in [Table - 1]. Importance of BP control Hypertension is one of the important and modifiable risk factors for the development and/ or worsening of DR. Raised BP causes endothelial stress with release of VEGF altering retinal autoregulation leading to increased perfusion pressure and injury. [36] Results of RCTs [37],[38],[39],[40] have demonstrated that hypertension is detrimental to each stage of DR and a tight BP control strategy can reduce the risk of eye complications from diabetes. In the UKPDS, 1148 hypertensive patients with type 2 DM were studied to assess the relationship between tight BP control and the different aspects of DR. Enrolled patients had type 2 DM for a (mean) duration of 2.6 years and a (mean) BP of 160/94 mmHg at baseline. Seven hundred and fifty-eight patients were randomly allocated to a tight BP control (< 150/85 mmHg) strategy and 390 patients were allocated to a less tight BP control (< 180/105 mmHg) strategy with angiotensin-converting enzyme inhibitor or beta-blockers as the main therapy. After 9 years of follow up, patients in the tight BP control strategy showed a 34% reduction (99% CI, 11-50%) in DR progression, 35% reduction in laser photocoagulation and 47% reduction (99% CI, 7-70%) in visual acuity deterioration compared to those assigned to less tight BP control. [37] As opposed to UKPDS, the findings of Appropriate Blood Pressure Control in Diabetes (ABCD) Trial (n = 470) however found no difference in DR progression between the groups assigned to a policy of tight BP (diastolic BP goal of 75 mmHg) control versus less tight BP control (diastolic BP goal of 80-89 mmHg) over a period of 5.3 years. This study also compared nisoldipine with enalapril as a first-line antihypertensive therapy for the prevention and progression of complications of diabetes (retinopathy, neuropathy). Analysis of the 470 patients in the trial (baseline diastolic BP ≥90 mmHg) revealed comparable control of BP, blood glucose and lipid concentrations, and smoking behavior in the nisoldipine (n = 237) and enalapril (n = 233) groups throughout the duration of follow-up. [38] Further, in order to investigate whether lowering BP in normotensive (BP < 140/90 mm Hg) type 2 diabetic patients offers any beneficial results on vascular complications, the ABCD trial randomized 480 patients to either moderate (80 to 89 mm Hg) or intensive (10 mm Hg below the baseline DBP) diastolic BP control groups and they were given placebo or nisoldipine or enalapril as an initial antihypertensive therapy respectively. At 5 years of follow-up, no difference was found in the (primary end point) creatinine clearance (P = 0.43), though the patients in the intensive group were less likely to progress to microalbuminuria (P = 0.012) and to overt albuminuria (P = 0.028). Further, the progression of DR (P = 0.019) was less frequent in the intensive group compared to moderate BP control group. [39] Understanding the role of renin-angiotensin system (RAS) in DR Preliminary studies have shown that angiotensin converting enzyme (ACE) is locally produced by endothelial cells of retinal vessels and retinal pigment cells. [40],[41] The retinal ACE expression causes adverse changes in retinal blood flow and vascular structure. [42] A small clinical study also showed that subjects treated with ACE inhibitors had relatively lower levels of vitreous VEGF than those not on ACE inhibitor treatment [43] indicating that the adverse effects of retinal ACE expression may be mediated by potentiation of VEGF activity. Compared to ACE, the angiotensin II has been particularly shown to potentiate activity of VEGF, which in turn leads to abnormal angiogenesis in retina, [44] increasing the risk of retinopathy progression. Further, there is a significant positive correlation between levels of angiotensin II and VEGF in the vitreous fluid in patients with proliferative retinopathy. [45] As discussed earlier in the pathogenesis of retinopathy, VEGF can further increase the permeability of retinal vessels, increasing the risk of macular edema. Animal studies in models of retinopathy in rats have shown that the formation of new abnormal retinal vessels in retinopathy can be inhibited by treatment with the ACE inhibitor lisinopril or the angiotensin II type 1 (AT1)-receptor blocker losartan. [46] The effect of the AT1-receptor blocker candesartan on VEGF and retinal function has also been studied in spontaneously hypertensive rats, wherein treatment with candesartan was shown to restore VEGF mRNA expression to normal levels, independent of its effects on systemic BP. [47] Greater understanding of retinal RAS has increased interest in further exploring the BP independent protective effects of ACE inhibitors and angiotensin II receptor blockers (ARB) in DR. The Eurodiab Controlled Trial of Lisinopril in Insulin Dependent Diabetes (EUCLID) investigated the effect of lisinopril on retinopathy in type 1 diabetics. Patients were not hypertensive and were normo- or microalbuminuric at enrollment. Over 2 years, lisinopril reduced the progression of DR by 50% (95% CI, 28-89%) and progression to proliferative DR by 80%. [41] This study concluded that ACE inhibitors may provide additional benefits in DR progression independent of BP lowering effect. [48] While the EUCLID study suggested beneficial effects of ACE inhibitors, UKPDS [37],[38],[39] and the ABCD study could not confirm the superiority of ACE inhibitors over other antihypertensives. Further, the importance of inhibition of the RAS and the effect of BP on the incidence and progression of microvascular complications were not answered. To address these questions, the Diabetic Retinopathy Candesartan Trials (DIRECT) Program was designed. This program consisted of three separate studies conducted with the objective of investigating the effect of an ARB, candesartan, on the burden of retinopathy in diabetic patients. DIRECT-Prevent 1 was conducted to assess the effectiveness of candesartan in reducing the incidence of retinopathy while DIRECT-Protect 1 evaluated the effect of candesartan on progression of retinopathy in type 1 diabetics. [49] DIRECT-Protect 2 assessed the effect of candesartan on progression and regression of retinopathy in type 2 diabetics. [50] DIRECT-Prevent 1 enrolled 1421 normotensive, normoalbuminuric type 1 diabetic patients (aged 18-50 years) without retinopathy and randomized to candesartan (n = 711) or to placebo (n = 710). DIRECT-Protect 1 enrolled 1905 normotensive, normoalbuminuric type 1 diabetic patients (aged 18-55 years) with retinopathy and randomized to candesartan (n = 951) or to placebo (n = 954). Incidence of retinopathy was seen in 178 (25%) patients in the candesartan group compared to 217 (31%) in the placebo group (Hazard Ratio (HR) for candesartan vs placebo, 0.82 (95% CI 0.67-1.00, P = 0.0508)). Progression of retinopathy occurred in 127 (13%) participants in the candesartan group versus 124 (13%) in the placebo group (HR, 1.02 (0.80-1.31, P = 0.85). These studies showed that candesartan reduced incidence of retinopathy in type 1 diabetes with no significant benefit on retinopathy progression. [49] The DIRECT-Protect 2 study randomized 1905 normoalbuminuric, type 2 diabetic patients (aged 37-75 years) who were normotensive or controlled hypertensives, to candesartan once a day (n = 951) or placebo (n = 954). The (median) duration of follow-up was 4.7 years. One hundred and sixty one (17%) patients in the candesartan group and 182 (19%) in the placebo group had progression of retinopathy (primary end point) by three steps or more on the Early Treatment Diabetic Retinopathy Study (ETDRS) scale. Although statistically non-significant, the risk of retinopathy progression was reduced by 13% in patients on candesartan compared with those on placebo (hazard ratio [HR] 0.87, 95% CI 0.70-1.08, P = 0.20). The proportion of patients who achieved regression of retinopathy (secondary end point) was 19% (n = 180) in the candesartan group compared to 14% (n = 136) in the control group, indicating that candesartan was associated with a 34% increase in the relative chance of regression (P = 0.009). The number needed to treat for regression benefits of candesartan in retinopathy was found to be 21. Subgroup analysis of patients depending upon baseline severity of retinopathy showed that patients with mild retinopathy showed greater regression benefits than patients with more severe retinopathy at baseline. Further, these beneficial effects were not attenuated by adjustment for baseline risk factors or changes in BP during the trial. An overall change towards less severe retinopathy by the end of the trial was observed in the candesartan group (odds 1.17, 95% CI 1.05-1.30, P = 0.003). Most common adverse events reported were hypertension, headache, influenza, and pain in extremities with no significant difference between groups. These results showed the beneficial effects of candesartan in improving retinopathy in type 2 diabetic patients. [50] None of the DIRECT trials could achieve the pre-specified end points. Further, it must be noted, that the reduction in incidence of retinopathy found in DIRECT Prevent 1 and DIRECT Protect 1 studies or decrease in the progression of retinopathy in DIRECT Protect 2, could not reach traditional statistical significance level, thereby making a clear recommendation of candesartan use for all diabetic patients difficult. The overall results however, suggest beneficial effect of candesartan in retinopathy in type 1 and type 2 diabetic patients. Further, these beneficial effects seen over a long duration of more than 4 years are definitely of significant clinical importance. Therefore, while choosing among pharmacological agents in type 1 diabetics without evidence of retinopathy or type 2 diabetics with retinopathy or those at risk of developing hypertension, candesartan may be given preference over others. Importance of serum lipid control There is a positive correlation between dyslipidemia and progression of retinopathy or macular edema. Dyslipidemia leads to development of hard exudates. [51] that in turn interfere with vision in DR/DME. A study of type 1 diabetic patients′ cohort from the DCCT/EDIC studies further confirmed this correlation and showed that severity of retinopathy was positively associated with triglycerides and negatively associated with HDL cholesterol levels. [52] Clinical studies have shown beneficial effects of atorvastatin and simvastatin in reducing hard exudates and progression of retinopathy respectively, in diabetic patients with dyslipidemia. [53],[54] The impact of long-term lipid lowering therapy on progression of retinopathy and the need for laser treatment in patients with type 2 diabetes has been assessed in the FIELD (Fenofibrate Intervention and Event Lowering in Diabetes) study. [55] FIELD was a randomized, multinational placebo controlled study (n = 9795, aged 50-75 years). The results showed that in the fenofibrate group (n = 4895) the need for first laser treatment for retinopathy was significantly (P = 0.0002) lower than in the placebo group (n = 4900) [3.4% versus 4.9%]. The progression of retinopathy (primary endpoint) did not differ significantly between the two groups (P = 0.19). However, patients with pre-existing retinopathy had significantly (P = 0.004) reduced progression (3.1%) of retinopathy in the fenofibrate group than the control group (14.6%). This study showed the beneficial effects of fenofibrate in reducing the need for laser treatment for DR, independent of plasma lipid levels. [55] The mechanism behind this novel property of fenofibrate may be the result of its antiapoptotic activity in retinal endothelial cells, independent of its lipid lowering activity. [56] Specific Treatment Modalities These include laser and surgical interventions in the management of DR. Laser photocoagulation Laser photocoagulation restores useful vision in many cases of proliferative retinopathy and maculopathy. The blue-green light of the argon laser is maximally absorbed by vascular structures. It has a spot size of 50-500 µm and can be used to target discrete lesions such as clusters of leaking vessels identified by fluorescein angiography, but is usually employed to destroy large areas of generally diseased retina. [57],[58] The aim of panretinal photocoagulation is to prevent the onset or induce regression of neovascularization without vitreous hemorrhage or fibrovascular proliferation. It ablates the peripheral retina with 1500 to 2000 burns that spare only a key-hole shaped central area that includes the disc, the macula and maculopapillary nerve bundle running between them. [57],[58] Thus it effectively concentrates the remaining retinal blood flow on to this crucial region, which serves central, high resolution color vision at the expense of the periphery. Results of Diabetic Retinopathy study (DRS) [59],[60] and the Early Treatment Diabetic Retinopathy Study (ETDRS), [61] have provided the strongest evidence to establish the place of panretinal photocoagulation as a standard technique for treating severe nonproliferative and proliferative DR and have shown that panretinal photocoagulation reduces the risk of moderate and severe visual loss by 50% in patients with severe nonproliferative and proliferative retinopathy. [59],[60],[61] Early PRP is recommended for patients with proliferative DR, especially in presence of high-risk features. [58] Laser treatment is also used to treat diabetic maculopathy either in the form of focal laser treatment or grid treatment. Focal treatment is required for focal lesions (e.g. microaneurysms, IRMA, or short capillary segments) located between 500 and 3000µm from the centre of the macula, which causes the hard exudates and retinal thickening. For lesions which do not leak the fluorescein dye but which are located beyond 3000µm from the center of the macula, focal laser photocoagulation is considered only if prominent leaks are present and are associated with retinal thickening that extend closer to the centre. Photocoagulation may also be used in grid pattern to treat diffuse areas of leakage or non-perfused retinal thickening. [57],[58] Properly conducted laser photocoagulation rarely causes serious complications. The adverse effects of PRP include visual field constriction, night blindness, color vision changes, inadvertent laser burn, macular edema exacerbation, acute glaucoma, and traction retinal detachment. [58] Vitreo-retinal Surgery Conventional laser treatment may fail in eyes with vitreous hemorrhage or in eyes with tractional retinal detachments and active progressive PDR. Early vitrectomy has been shown to improve visual recovery in patients with proliferative retinopathy and severe vitreous hemorrhage. The Diabetic Retinopathy Vitrectomy Study (DRVS) evaluated the risks and benefits of early surgical intervention versus conventional treatment for vitreous hemorrhage and very severe PDR. [62] The results of DRVS demonstrated that patients who underwent early vitreoretinal surgery had better outcome than those treated conservatively, with 25% of the early vitrectomy group versus 15% of the observation group having 20/40 or greater vision after 2 years′ follow-up. The indications of vitrectomy have now been widened due to advances such as intra-operative fundal imaging and laser treatment and bimanual instrumentation to manipulate the retina, which may help improve clinical outcomes. [62] Laser and Surgical Interventions for Diabetic Macular Edema The ETDRS study has provided evidence that focal laser photocoagulation preserved vision in eyes with DME with the greatest benefits in eyes with clinically significant DME. [63],[64] Diffuse DME which is nonresponsive to focal laser treatment may benefit from vitrectomy. However in the light of inconsistent findings from few RCTs, the role of vitrectomy should be restricted to the presence of vitreous traction and macular edema in association with visual impairment. [58] Role of Adjunctive and Other Pharmacotherapies Although medical management (control of blood sugar, BP, and serum lipids) and ocular management (laser photocoagulation and vitrectomy) remain the mainstays of DR management, advances in pharmacotherapy have shown promise in the treatment of DR. The three major classes of medications currently being studied in this context are corticosteroids, VEGF inhibitors/antagonists, and miscellaneous agents. Corticosteroids Corticosteroids may produce their effects through multiple mechanisms of actions apart from their potent anti-inflammatory and VEGF downregulating effects. Intravitreal triamcinolone (IVTA) has shown significant improvements in DME and visual acuity in various RCTs. [65] However, steroid-induced elevation of intra-ocular pressure (IOP) and steroid-induced cataract are commonly reported as adverse effects of IVTA. Intravitreal or retinal implants have also been developed, allowing extended drug delivery. In this context, a surgically implanted intravitreal fluocinolone acetonide was shown to be associated with improvement in visual acuity in DME. [66] An injectable, biodegradable intravitreal dexamethasone extended release implant was also evaluated in an RCT, with reported improvements in visual acuity and macular thickness. [67] VEGF inhibitors VEGF is an important mediator of angiogenesis and breakdown of blood-retinal barrier in the ischemic retina and its role in the pathogenesis of DR has already been described in earlier sections. Inhibition of VEGF activity may play a pivotal role in the prevention of DR. Three VEGF antagonists are currently under investigation and are briefly discussed below: Pegaptanib acts by targeting the 165 isoform of VEGF for treatment of neovascular age-related macular degeneration (AMD). In a RCT (n = 172) patients with DME were randomized to repeated intravitreal Pegaptanib or sham injections. The results showed that Pegaptanib treated eyes were more likely to achieve improvements in visual acuity (P = 0.03), macular thickness (P = 0.02), and need for focal laser treatment (P = 0.04) at 36 weeks than those on sham injections. [68] Retrospective analysis of the same study also showed regression of neovascularization in patients with proliferative DR (n = 16). [69] Another anti-VEGF agent, Ranibizumab, a recombinant humanised monoclonal antibody fragment with specificity for all isoforms of human VEGF, has been used for treatment of neovascular AMD [70],[71] and may also be useful for DR and DME. [72] Similar to ranibizumab, bevacizumab is a full-length humanised monoclonal antibody against VEGF which appears to produce similar efficacy for treatment of neovascular AMD and may also be effective for DME and proliferative DR. [73],[74],[75],[76] An ongoing RCT sponsored by the US National Eye Institute is comparing the effects of laser treatment, intravitreal bevacizumab, and combined intravitreal bevacizumab and laser or sham injection on DME. [77] PKC inhibitors Two PKC inhibitors are undergoing clinical evaluation to study their effects on reducing microvascular complications in diabetic patients. Ruboxistaurin is a specific inhibitor of PKC-b and is the first oral pharmacologic agent shown to reduce visual loss in diabetic patients over an extended period. The results from the PKC-b Inhibitor Diabetic Retinopathy Study 2 (PKC-DRS2) showed that Ruboxistaurin reduces the occurrence of sustained moderate visual loss by 40% in patients with moderately severe to very severe NPDR, simultaneously increasing the likelihood of visual improvement. Ruboxistaurin treatment also reduces progression of CSMO, progression of overall DME severity, and the need for initial focal photocoagulation. [78] The second PKC inhibitor, PKC412, inhibits multiple PKC isoforms and at least two other receptor kinases. [79] Preliminary clinical evaluations have shown that PKC412 at doses of 100 mg/day orally or higher may significantly reduce macular edema and improve VA in diabetic subjects. [80] Growth hormone inhibitors Somatostatin analogs may inhibit angiogenesis directly through somatostatin receptors present on endothelial cells, and also indirectly through the inhibition of postreceptor signaling events of peptide growth factors such as insulin-like growth factor 1 and VEGF. In a randomized controlled study (n = 23) of patients with severe NPDR or early PDR, octreotide (a long-acting somatostatin analogue) along with conventional treatment reduced the requirement for laser photocoagulation and reduced the incidence of ocular disease progression compared to conventional treatment alone. [81] A multicenter, randomized, placebo-controlled clinical trial of octreotide is currently under way in patients with severe NPDR and early PDR. [82] Place of other pharmacotherapies in the management of DR Results of clinical trials do not support the use of anti-platelet agents, [83] aldose reductase inhibitors [84] and advanced glycation end-products inhibitors [85] in the management of DR. The role of COX-2 inhibitor, celecoxib, in the treatment of PDR is being evaluated in an ongoing clinical trial. [25] Short-term high-dose antioxidant therapy with oral vitamin E may help in normalizing retinal hemodynamics in diabetic patients, [18] although this effect requires further evaluation in a large scale RCT. In the absence of substantial clinical evidence, the place of many potential pharmacotherapies such as Interferon-alpha 2a, acetazolamide, intravitreal injection of tissue plasminogen activator and pigment epithelium-derived factor cannot be defined in the management of DR. [25] Other Ocular Co-Morbidities Associated with Diabetes Apart from DR, a range of ocular pathologies is associated with diabetes, which may lead to blindness. Some of these conditions such as cataract, anterior ischemic optic neuropathy, diabetic papillopathy and ocular movement disorders are directly associated with diabetes whereas diabetes is one of the known or possible risk factors for other ocular conditions such as glaucoma, ocular ischemic syndrome, retinal vein occlusion retinal arteriolar emboli, retinal artery occlusion and abnormalities of the corneal epithelium. [86] DR and co-morbid cataract Diabetes may accelerate the progression of cataract, probably through deposition of AGE products in the lens. As a result, in diabetics, cataract may occur at a younger age and progress more rapidly, resulting in higher rates of cataract surgery at a relatively young age than non-diabetics. [86] Wisconsin Epidemiologic Study of Diabetic Retinopathy found the 10-year cumulative incidence of cataract surgery to be 8% in type 1 diabetics and 25% in type 2 diabetics, with older age being one of the commonest predictors of cataract surgery. [87] Intraocular lens (IOL) implantation should not be contraindicated in cataract patients with DR. [88] However, presence of preoperative rubeosis iridis, proliferative DR and possibly significant background retinopathy may be considered as relative contraindications for surgery. In patients presenting with cataract and active proliferative DR where adequate PRP is not possible before surgery, the following management options may be considered: [89]
It is not an uncommon finding that patients with diabetes may present with poorer vision outcomes post-cataract-surgery than those without diabetes, mostly due to the presence of co-morbid maculopathy or proliferative retinopathy in diabetes. Various studies have also shown that patients with diabetes have an increased risk of developing postoperative endophthalmitis which further results in poorer vision outcomes. [86] In a retrospective study (n = 37) conducted to determine whether cataract surgery (phacoemulsification) causes the progression of DR, it was found that an uncomplicated surgery had no significant influence on the postoperative progression of DR and that patients with preoperative NPDR had greater risk of postoperative retinopathy progression. [90] Also, another study showed male sex and among males, duration of diabetes, to be the risk factors for the occurrence of DR (new development of any DR) after cataract surgery and that inadequate systemic control of diabetes further increased this risk. [91] Message to Family Physicians Early detection, careful follow-up and prompt treatment are key stages in the successful management of DR. Apart from their pivotal role in counseling the patients on how to reduce the risks of developing diabetes and providing adequate medical care to patients with diabetes, family physicians can play a vital role in the prevention of blindness due to diabetes. Family physicians need to motivate their patients with diabetes to undergo initial eye examination and also impress upon them the importance of regular follow-up eye examinations. [92] All diabetic patients more than 12 years old should be advised to get their visual acuity tested and retina examined annually or more frequently if progressive changes are observed. [23] There should be a close liaison with ophthalmologists and a low threshold for referral. As diabetes has no cure, such periodic eye examination is the only way to detect the patients at risk of developing unnecessary blindness and to protect them by implementing timely and appropriate primary and/or secondary interventions.A Public Health Approach to Diabetic Retinopathy DR is a major public health problem. With an ongoing pandemic of type 2 diabetes mellitus, this problem will further get aggravated in the years to come. Although the standards of treatment and prevention of blindness due to DR are universally known and accepted, a large population of diabetic patients in developing as well as developed countries is still going blind, mainly due to lack of provision of standardized treatment to such patients. This is also a warning to the entire scientific community to focus upon developing a public health approach to DR based upon existing knowledge, tools and interventions than merely focusing extensively in developing new diagnostic technologies and/or treatment options. [93] Therefore, a management program for DR from a public health perspective should ideally include - timely eye examinations as recommended by WHO and/or other professional bodies, provision of standard preventive treatment, optimal treatment of blood sugar and blood pressure levels, efforts to educate diabetic patients about eye health and ultimately efforts to prevent type 2 diabetes by educating and empowering patients for self-management. This, while individually outside the scope of family physicians or physicians or ophthalmologists, who play vital roles in various stages of managing DR, the prevention of blindness due to diabetes is very much the duty of each of them, justifying the pressing need for a public health approach for comprehensive management of DR.Rehabilitation of Low Vision due to Diabetic Retinopathy Many patients with DR suffer from low/impaired vision. Low vision in turn creates difficulty in performing vocational as well as avocational tasks (reading, taking medications, self-monitoring of blood glucose for insulin management, giving themselves insulin injections, controlling diet, independent mobility etc) effectively and independently. Effective low vision care therefore is necessary to rehabilitate such patients′ vision and also assist them regain as independent a lifestyle as possible. For patients with mild vision loss, simple environmental modifications in terms of illumination, glare, contrast, figure-ground perception may be sufficient to be able to perform tasks of daily living. Patients with moderate to severe visual loss may benefit from eyeglasses, magnifiers, or closed-circuit television, in reading and writing activities. Improved products for insulin injection or glucose monitoring are also available and helpful for use by patients suffering from low vision. [94] Thus, a comprehensive rehabilitation program of low vision due to DR should not only involve family physicians but also other types of healthcare providers. It should however be remembered that rehabilitation is not a "quick fix" but a long-term process, the ultimate objective of which is to improve the patients′ quality of life and help them use their remaining vision in the most effective manner.Conclusion Despite effective treatments being available, DR still remains the major cause of preventable vision loss worldwide. Appropriately scheduled eye examinations along with proven primary interventions (strict glycemic and BP control) and timely secondary interventions (laser photocoagulation, vitrectomy) remain the cornerstones in the effective management of DR. A target of HbA1c level < 7% is ideal in patients with DR and any lowering of levels of HbA1c is beneficial in reducing the occurrence of new DR or delaying the progression of existing DR. A target systolic BP of less than 130 mm Hg is ideal in patients with DR and any lowering of systolic and/or diastolic BP is beneficial in reducing the occurrence of new DR or delaying the progression of existing DR. Although reduction in low-density lipoprotein cholesterol is associated with decreased macrovascular complications of diabetes, the role of lipid lowering therapy for DR prevention remains inconclusive whereas the use of anti-platelet agents and aldose reductase inhibitors is not supported in the absence of favorable evidence from clinical trials. Increasing understanding of the novel biochemical pathways involved in the pathophysiology of DR, and results from completed as well as ongoing clinical trials exploring the role of potential pharmacotherapies, further raise the optimism of having additional effective treatment options in the management of DR. References
Copyright 2008 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms08093f1.jpg] [ms08093t1.jpg] |
| |||||||||


{kind=link}
{kind=link}