 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
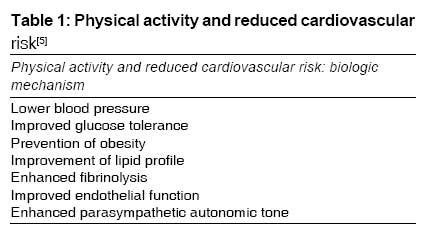
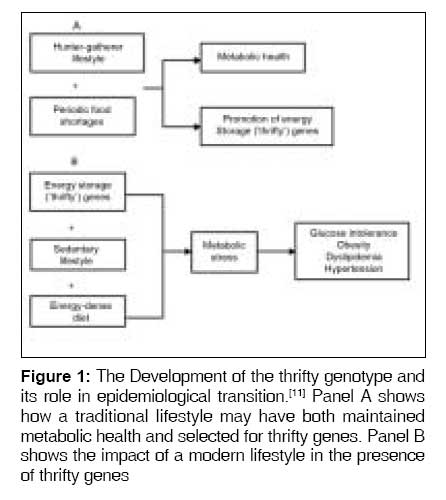
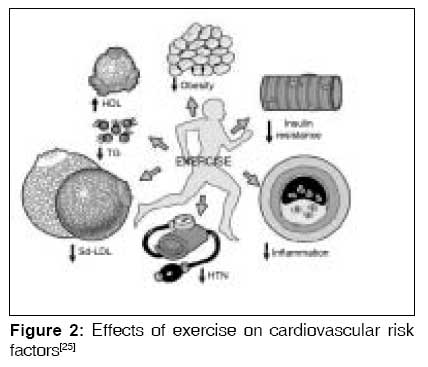
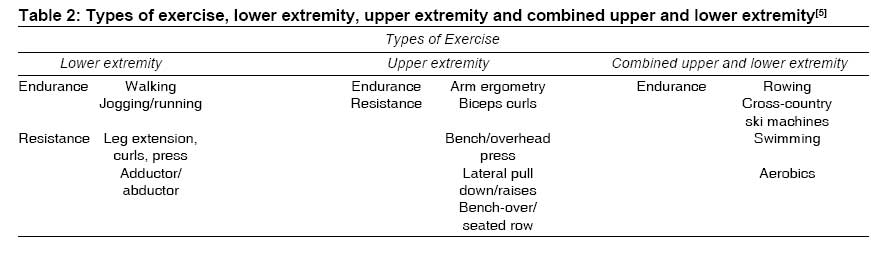
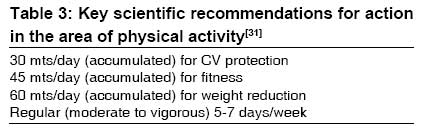
Indian Journal of Medical Sciences, Vol. 63, No. 1, January, 2009, pp. 33-42 Practitioners section Physical inactivity : A cardiovascular risk factor Prasad DS, Das BC Sudhir Heart Centre, Berhampur-760 002, Orissa Code Number: ms09008 Abstract Evidence regarding health benefits of physical activity is overwhelming and plays a critical role in both the primary and secondary prevention of coronary artery disease (CAD). Epidemiological investigations show approximately half the incidence of CAD in active compared to sedentary persons. A sedentary lifestyle is considered by various national and international organizations to be one of the most important modifiable risk factors for cardiovascular morbidity and mortality. Fortunately, a moderate level of occupational or recreational activity appears to confer a significant protective effect. Once coronary artery disease has become manifest, exercise training can clearly improve the functional capacity of patients and reduce overall mortality by decreasing the risk of sudden death. Well-designed clinical investigations, supported by basic animal studies, have demonstrated that the beneficial effects of exercise are related to direct and indirect protective mechanisms. These benefits may result from an improvement in cardiovascular risk factors, enhanced fibrinolysis, improved endothelial function, decreased sympathetic tone, and other as-yet-undetermined factors. Hence physical fitness, more than the absence of ponderosity or other factors, is the major determinant of cardiovascular and metabolic risk and long-term disease-free survival, in effect linking health span to life span. It is obviously in every individual's interest to assume the responsibility for his or her own health and embrace this extremely effective, safe, and inexpensive treatment modality. The need for a comprehensive review of this particular topic has arisen in view of the high prevalence of physical inactivity and overwhelming evidence regarding CVD risk reduction with regular physical activity. Keywords: Cardiovascular disease, physical inactivity, risk factor Introduction Physical activity, physical fitness, cardio respiratory fitness, exercise and metabolic fitness are related entities but have different definitions. Physical activity is defined as any bodily movement produced by skeletal muscles that results in energy expenditure [1] significantly beyond resting level, particularly involving continuous actions of large muscles. Exercise is defined as the systematic execution of physical activity for a specific purpose. [2] Exercise training may be a more accurate term, because similar activity may be viewed as exercise by one person and not by others. [1] Physical fitness is a set of attributes that enables an individual to perform physical activity. [3] It encompasses cardio respiratory fitness, muscular strength, muscular endurance, flexibility, and body composition. [4] Cardio respiratory fitness is best assessed by measures of maximal oxygen uptake (VO2max). Many studies estimate fitness levels by measurement of the peak work rate or MET level achieved during graded exercise tests. [5] Metabolic fitness is the state of metabolic systems and variables predictive of the risk for diabetes and cardiovascular disease which can be favorably altered by increased physical activity or regular endurance exercise without the requirement of a training-related increase in VO2max. [4] Regular physical activity, fitness, and exercise are critically important for the health and wellbeing of people of all ages. Research has demonstrated that virtually all individuals can benefit from regular physical activity, whether they participate in vigorous exercise or some type of moderate health-enhancing physical activity. Even among frail and very old adults, mobility and functioning can be improved through physical activity. [6] Physical activity results in increased exercise capacity and cardio respiratory fitness, which may lead to many health benefits. Individuals who are physically more active appear to have lower rates of all-cause mortality, probably due to a decrease in chronic diseases, including coronary artery disease (CAD). This low rate may result from an improvement in cardiovascular risk factors, enhanced fibrinolysis, improved endothelial function, decreased sympathetic tone, and other as-yet-undetermined factors. The same is depicted in [Table - 1]: Physical Activity and reduced cardiovascular risk [5] Regular endurance and resistance exercise leads to favorable alterations in the cardiovascular, musculoskeletal, and neurohumoral systems. These alterations result in a training effect that allows an individual to do increasing amounts of work at a lower heart rate and blood pressure. Such an effect is particularly desirable in patients with CAD, because it allows increased activity with less ischemia. [5] Physical Inactivity, Thrifty Genotype, Epidemiological Transition The rising burden of noncommunicable diseases which has occurred with modernization can be understood in the context of ′epidemiological transition′. [7] It has been proposed that obesity and type-2 diabetes had their roots in a natural selection of these early humans, favoring a "thrifty genotype", [8] which enabled highly efficient storage of energy during periods of food abundance. Similarly, the ′thrifty phenotype′ [9] explains how low-birth-weight babies, who have been exposed to a chronic energy-deprived state, hoard energy stores and go on to develop type-2 diabetes in adulthood. A corollary of these hypotheses is that these genetic or phenotypic adaptations that are useful in an energy deprived state become disadvantageous when the dietary energy intake becomes high and physical activity level drops. [10] The development of the thrifty genotype and its role in epidemiological transition: [11] is depicted in [Figure - 1].Physical Activity and Public Health It is now more than 50 years since the physical activity-CAD hypothesis was launched by Morris et al. [12] with his pioneer work on London bus drivers. In the 1950s, Morris and Crawford [13] first suggested that the rate of coronary artery disease (CAD) was inversely related to the level of physical activity during occupational activities. [13] In the London transportation study, sedentary bus drivers had almost twice the incidence of CAD as compared to the conductors who regularly walked up and down the stairs of double-decker buses. [12] Since then, physical inactivity has been documented as a well-established risk factor for CAD in Western populations; a sedentary lifestyle is associated with about a two-fold increase in risk of CAD. With increasing rates of urbanization and other major changes in human behavior, the prevalence of a sedentary lifestyle has further increased particularly among the young; it is estimated that children today expend approximately 600 kcal/day less than their counterparts 50 years ago. [14] A sedentary lifestyle resulting from low activity levels both at work and during leisure time is associated with a significant increase in cardiovascular disease (CVD) and all-cause mortality among both sexes. The associations are strong, independent of other major risk factors and illustrate the enormous preventive potential, given the high prevalence of a sedentary lifestyle in most communities. [15] Regular exercise results in an increase in exercise capacity and lower myocardial oxygen demand, leading to cardiovascular benefits such as lower mortality rates and fewer symptoms of CAD. [16],[17],[18] Organizations including the CDC, the American College of Sports Medicine (ACSM), and the American Heart Association (AHA), [19] have published consensus reports and recommendations for the promotion of physical activity in an attempt to increase leisure-time activity. In a joint statement, [3] the CDC and ACSM recommend that all adults participate in at least 30 minutes of moderate-intensity exercise on most, if not all, days of the week. Moderate-intensity physical activity is achievable for most adults and can be accomplished with many routine activities such as walking briskly, swimming, house cleaning, lawn mowing, and gardening. These recommendations emphasize that the 30 minutes of activity can be obtained intermittently throughout the day in 10-minute increments or in one continuous session. Thus, physical activity can become part of the daily routine and may involve using stairs instead of an elevator, walking or biking instead of driving, calisthenics, or use of exercise equipment while watching television. [3] An increase in lifestyle physical activity can be as effective as participation in traditional, structured exercise in improving caloric expenditure, blood pressure, and cardio respiratory fitness. [20] Physical inactivity also appears to correlate with various socioeconomic factors. Participation in leisure-time physical activity is positively associated with higher education, higher income, employment status, and marriage. [1] Evidence to date suggests that socioeconomic status is an important and independent factor in the etiology and progression of CVD. When socioeconomic status is characterized by the principal measures of education, occupation, and income, there appears to be a consistent, inverse relation between these indicators and CVD risk factors-primarily hypertension, obesity, cholesterol levels, and cigarette smoking. [21] Many studies have demonstrated that regular exercise and physical activity prevent primary and secondary cardiac events. In one of the most well-known studies, male Harvard University alumni without a history of CVD were followed for 16 years. [22] There was a 39% reduction in cardiovascular morbidity and a 24% reduction in cardiovascular mortality in subjects with exercise energy expenditures of more than 2,000 kcal per week. Oldridge et al. [17] performed a meta-analysis of ten randomized clinical trials that examined the effects of cardiac rehabilitation after myocardial infarction (MI). No differences in nonfatal MI were apparent; however, there was a 24% reduction in all-cause mortality and a 25% reduction in cardiovascular mortality among exercise rehabilitation patients compared with controls. Several population-based studies show that incremental levels of regular physical activity are inversely proportional to long-term cardiovascular mortality when controlled for the presence of other risk factors in both men and women. [3],[16],[22],[23] Paffenbarger et al. [23] have reported encouraging data that demonstrate that, when habitual physical activity levels are increased, subsequent mortality is decreased relative to those who remained physically inactive. These data strongly support the need to increase physical activity and fitness levels among both women and men, with the greatest reduction in mortality for those who are the least fit. The specific mechanisms by which physical activity reduces CAD mortality are not known. Exercise improves lipid profile, glucose tolerance, elevated blood pressure, obesity both generalized and regional (waist circumference/visceral obesity). In a cross-sectional analysis of a large cohort of men and women, increasing levels of physical fitness assessed by maximal exercise treadmill testing were found to protect against elevations in most coronary risk factors in persons with and without CAD. [24] However, modification of atherosclerotic risk factors does not fully explain the benefits that have been observed. Other possible mechanisms including effects on thrombosis, endothelial function, and autonomic tone may play an important role [Figure - 2]. [25] Physiology of Exercise; Types of Exercise Endurance (aerobic, dynamic) training consists of dynamic or isotonic exercise, which involves high-repetition movements against low resistance. Examples include walking, jogging, swimming, or cycling. Isotonic exercise implies that muscles shorten but maintain a constant tension, although tension does change to some degree during exercise. [26] Endurance exercises employ rhythmic contraction and relaxation of working muscles. This results in increased blood flow to active muscles during relaxation and increased venous return to the heart from the working muscles during contraction. Regular dynamic exercise is referred to as endurance training, because it results in improved functional capacity, enabling the individual to exercise for a longer duration or at a higher work rate. See [Table - 2] [5] Resistance training, also called static exercise, exerts muscles at high intensities without movement of the joints, which is anaerobic as opposed to aerobic endurance exercise. This training may also be referred to as isometric exercise, because muscle tension develops predominantly without muscle shortening. An example of resistance training is weightlifting. The development of muscle tension during resistance training restricts blood flow during contraction. Regular resistance training leads to increased strength and is commonly referred to as power or strength training. [5] Responses to Exercise Training Regular endurance or resistance training results in specific changes in the muscular, cardiovascular, and neurohumoral systems that lead to improvement in functional capacity and strength. These changes are referred to as the training effect and allow an individual to exercise to higher peak work rates with lower heart rates at each submaximal level of exercise. Endurance training results in increased venous return to the heart, which leads to higher LV volumes. Resistance training exposes the patient to chronic increases in after load due to increased total peripheral resistance and elevated blood pressure, yielding a greater LV wall thickness. These effects result in increased LV mass in both training groups. However, the LV mass-lean body mass ratio is elevated in the endurance trainer, whereas it is normal in the resistance trainer. [27] The increase in LV mass in the resistance trainer is proportional to the increase in skeletal muscle mass. Along with changes in myocardial mass, certain hemodynamic effects are observed from endurance and resistance training. Wall stress at rest in endurance trainers is normal; however, it is lower in resistance trainers due to increased wall thickness without ventricular dilation. [28] Systolic function and fractional shortening at rest are normal in both groups. However, compared with non-athletes, stroke volume is increased due to greater end diastolic volumes. [28],[29] Despite increased LV wall thickening, diastolic function appears to be normal in both groups. [30] Intensity, Frequency, and Duration of Physical Activity The CDC, ACSM [3] and Surgeon General [1] recommend that adults exercise for 30 minutes at moderate-intensity levels on most, if not all, days of the week to achieve a weekly energy expenditure of at least 1,000 kcal. These statements stem from evidence stating that regular moderate physical activity provides many health benefits. In addition, these recommendations stress that physical activity can be accomplished in multiple short intervals-which may be more feasible for many individuals-rather than continuous 30-minute exercise sessions. Low-intensity exercise should be performed more frequently and for longer duration. The CDC recommendations are based on data that suggest that the benefits of exercise are related to the total energy expenditure or dose measured in calories or duration of physical activity. However, an important question remains regarding the intensity of physical activity required to incur a mortality benefit. Intensity can be defined in terms of absolute and relative reflecting the rate of energy expenditure during exercise (expressed in METs or kcal per minute) or the relative percentage of maximum aerobic capacity that is maintained during the exercise or activity (expressed in terms of percentage of maximum heart rate or percentage of O2max achieved on exercise tests) [Table - 3]. [3] Risks of Exercise: Cardiovascular Risks: The risks of cardiovascular morbidity and mortality depend on whether one studies the general population or individuals with CAD. Although the risk of death during exercise is low, death in individuals over 35 years of age is usually the result of atherosclerotic CAD, whereas younger individuals are more likely to suffer from congenital cardiac malformations. [32] The incidence of sudden cardiac death during exercise for the population at large is 1 in 565,000 events per hour. [33] The risk of sudden death during exercise is much lower for young individuals than for middle-aged and older adults. Among high school and college athletes, the sudden death rate is estimated to be 1 in 133,333 male athletes and 1 in 769,230 female athletes. [34] Medical Screening Before Exercise Although regular exercise leads to health benefits, the incidence of cardiovascular events during exercise is estimated to be 10 times greater than that at rest among otherwise healthy persons. [33] The CDC [1] and AHA [33] conclude that most persons do not need to see their physician before starting a moderate-intensity physical activity program. However, it is advised that men older than 45 years and women older than 55 years who plan to start a program of vigorous intensity (>60% O2max) or individuals with risk factors, signs, or symptoms of cardiovascular or chronic disease consult their physician to design an exercise program. The US Department of Health and Human Services has published recommendations for the promotion of health and prevention of disease in Americans. [35] A major objective is to enhance the physical activity of inactive individuals in an attempt to reduce chronic diseases and improve quality of life. Moderate and high levels of leisure time and occupational physical activity are associated with a reduced CVD and all-cause mortality among both sexes. Promoting moderate levels of leisure-time and occupational physical activity are essential to prevent premature CVD and all-cause mortality. [36] The existing broad-based public health recommendations are reasonable and scientifically sound. However, it is hoped that customized activity prescriptions tailored to individual need, risks and benefits will someday replace the current generic recommendations. [5] Summary
Given limited resources for tertiary care in India and the important role of physical exercise in coronary risk reduction, improvements in physical activity should be promoted considering high prevalence of physical inactivity among Indian youth and adults who need the concerted and focused effort of one and all. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09008t3.jpg] [ms09008t2.jpg] [ms09008f2.jpg] [ms09008t1.jpg] [ms09008f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}