 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Sciences, Vol. 63, No. 2, February, 2009, pp. 53-57 ORIGINAL CONTRIBUTION Pulmonary distress following attempted suicidal hanging Nair Shalini, Jacob Joe, Aaron Sanjith, Thomas Maya, Joseph Mathew, Alexander Mathew Department of Neurological Sciences, Christian Medical College, Vellore
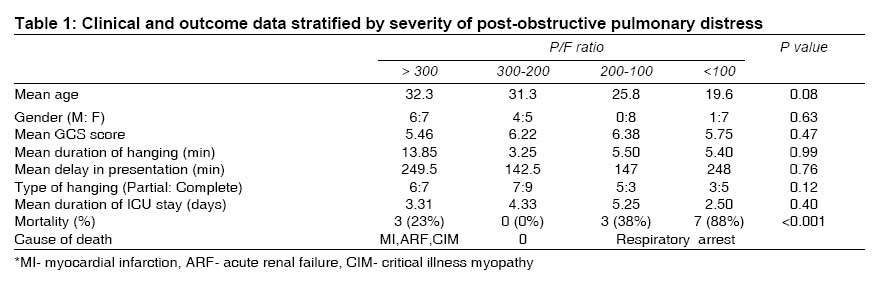
Code Number: ms09010 Abstract Objective : To assess the incidence of post-hanging pulmonary distress in cases of attempted suicidal hanging and predictors of outcome among these patients. Keywords: ABG, PaO 2 / FiO 2 ratio, post-obstructive pulmonary distress, prognostic factors, suicidal hanging Introduction Hanging is a common mode of attempting suicide in the developing world [1] and is increasing at an alarming rate in the developed world as well. [2] The existing literature on hanging is, for the most part, on the influence of the Glasgow coma scale and the presence of spontaneous circulation on the outcome [3],[4],[5],[6] ; and complications like post-obstructive pulmonary distress, which may be caused by pulmonary or neurogenic edema, ARDS, aspiration pneumonitis and neck vessel compression, have not been well described. The largest published review of post-obstructive pulmonary edema (26 cases) had laryngospasm as the commonest cause, with only 3 cases of hanging or strangulation. [7] The pathophysiology of type I post-obstructive pulmonary edema as in post hanging is thought to be influenced by both hydrostatic forces and increased permeability of alveolar epithelium following sudden upper airway obstruction, though the rapid rate of net alveolar fluid clearance and the raised edema fluid-to-plasma protein ratio tend to favor the hydrostatic mechanism. [8] This presumed mechanism of edema pathogenesis has led to a physical approach to management, using ventilation with positive end-expiratory pressure (PEEP) to reduce the edema fluid. We evaluated a cohort of 38 patients who had attempted suicidal hanging and had post-hanging pulmonary distress, in order to try and determine predictors of final outcome that would enable to prognosticate better at the time of presentation to casualty. Materials and Methods A retrospective study of patients admitted in a 5-year period (January 2001 to December 2005) was conducted with permission from the Institutional Review Board vide IRB-2-17-09-2008. Clinical and laboratory data were acquired by the principal investigator from computerized ICU and case records, and all radiological diagnoses were reconfirmed on the picture archival and communication system (PACS, GE). Data collected included demographics, type of hanging (partial or complete, depending on whether the feet were touching the ground or not) and probable duration of hanging, time to reach hospital, history of vomiting or attempted feeding, GCS score at presentation and P/F ratio from the admission arterial blood gas (ABG). Duration of ventilation, ICU stay, hospital stay and mortality were also recorded. Post-obstructive pulmonary distress was diagnosed at the time of presentation to casualty, historically from the acute onset of dyspnea and pulmonary injury, corroborated radiologically with bilateral paracardiac distribution of alveolar shadow with normal cardiac size and vascular pedicle width, thus ruling out cardiac cause for pulmonary injury. All patients with post-hanging pulmonary distress were immediately intubated and ventilated at arrival due to inadequate airway and breathing. Patients were then transferred to the ICU, ventilation was started with an FiO 2 of 1 and PEEP of 3 cm H 2 O, and an ABG was sent. The PEEP was then incrementally increased until an SpO 2 of 100% was achieved, following which the FiO 2 was progressively reduced to maintain a minimum SpO 2 of 99%. Patients were ventilated with sedation and muscle relaxants for at least 24 hours, and further use of relaxants was based on radiological and clinical improvement. The patient was gradually weaned off the ventilator, with liberal indications for tracheostomy in patients who had a significantly impaired sensorium due to hypoxic encephalopathy. Statistical analysis Analysis was done with SPSS 11 (SPSS Inc., Chicago, USA). Univariate analysis was performed using Pearson Chi-square and Mann-Whitney U tests. Multivariate analysis of the data was not possible due to small size of the study cohort. Results Over the 5-year study period, 335 patients who attempted hanging were admitted to the 12-bed Neurological Sciences ICU, constituting almost 9% of all admissions. Post-hanging pulmonary distress was diagnosed in 38 patients (11% of all patients who attempted hanging). The development of post-hanging pulmonary distress was a significant risk factor for increasing mortality in this cohort. Thirteen (34.2%) of the 38 patients with post-hanging pulmonary distress died, in comparison to 15 (5.1%) of 297 patients without pulmonary distress (P value ≤ 0.001). Demographic and clinical data are presented in [Table - 1]. The age and gender distributions in the patients who developed post-hanging pulmonary distress did not differ significantly from those of the entire population of patients with hanging, who were, predominantly, young females with a mean age of 24.5 years. The GCS, type of hanging, probable duration of hanging and delay in getting medical aid did not significantly affect the outcome in patients with post-hanging pulmonary distress, even if stratified for severity of pulmonary distress. The severity of post-hanging pulmonary distress was graded based on the P/F ratio of ABG at presentation, with a P/F> 300 being classified as mild, and a P/F < 100 being classified as severe pulmonary distress. Patients with severe pulmonary distress had the worst outcome, with 88% mortality (7/8 patients); while the mortality for mild pulmonary distress was only 23% (3/13 patients). Univariate analysis demonstrated that this difference was significant (P < 0.001). Though the absence of death in the category of P/F 200-300 was intriguing, the result was still within the 95% confidence interval. Discussion Suicide constitutes 8% to 12% of all unnatural deaths in India, with up to 41% attributed to hanging. [9] The patient population in existing literature on hanging is predominantly male, with an average age of 40 years and a history of substance abuse. [6],[7] In contrast, our study population consisted predominantly of young females with a mean age of 24.5 years, and most cases arose from domestic disputes. The published prognostic factors in hanging include the GCS, absence of spontaneous circulation on arrival at the hospital, presence of seizures, duration of hanging and delayed presentation to a medical facility. [2],[5],[6],[10] None of these factors were found to affect the outcome in this cohort of patients. There are no studies evaluating the effect of pulmonary injury on survival in patients who attempted suicidal hanging. Salim et al.[4] found no pulmonary complications in their 10-year experience with 63 patients of hanging, while we found an incidence of 11% in 335 patients. Existing literature on post-hanging pulmonary distress lacks systematic evaluation of hanging as the etiology, as the most common reported cause is laryngospasm following extubation after anesthesia. [7],[11] The incidence of type I post-obstructive pulmonary edema in all general anesthetic procedures varies from 0.05% to 0.1%. [12] Judicial hanging causes fatal injury to the cervical spine, brain stem and the larynx [13] ; while suicidal attempts usually result in compression of the internal jugular veins and the carotid arteries, leading to cerebral hypoxia and airway compression, finally resulting in global hypoxia. [14] In contrast to previous thinking of airway compression being the common cause of immediate death in such cases, it is now believed that jugular veins and carotid arteries are compressed much earlier in the course of events, even with lesser pressure exerted and leading to hypoxic circulation and reduced arterial cerebral supply. The potential complications thus arising are pulmonary and cerebral edema, seizures, ARDS and multi-organ failure. [15],[16],[17],[18],[19] The absence of any spinal cord injury in this series is similar to an earlier series published from the same institute and to the observations made by several other authors. [20],[21],[22] This study for the first time draws attention to the fact that pulmonary distress is a comparatively common complication of hanging, and demonstrates that it is an independent predictor of mortality. The P/F ratio has not previously been used to quantify the severity of post-hanging pulmonary distress, and it was found to be an accurate indicator of prognosis in these patients, with a P value of < 0.001. If we consider the fact that of the 3 deaths in the group with mild pulmonary distress, 1 was due to a myocardial infarction and 1 due to a severe critical illness myopathy and acute renal failure, the influence of the severity of post-hanging pulmonary distress becomes even more apparent. The severity of pulmonary distress did not correlate with other outcome variables such as ICU and hospital stay even after accounting for early mortality. This study highlights the still quite high incidences of attempted suicidal hanging in the developing world and its varied demographics in contrast to the developed world (more in the young age group and among females). The increased likelihood of pulmonary injury in survivors of such attempts is a revelation. Assessing the severity of pulmonary distress based on P/F ratio on ABG enabling prognostication of the final outcome is unique to this study. However, the small size of the study cohort limited a reliable multivariate evaluation, which in turn limits the significance of the observations made. A larger and longer study is warranted in future to further evaluate the importance of post-obstructive pulmonary distress in hanging. Nevertheless, this study emphasizes the importance of pulmonary evaluation in patients of hanging and the influence of post-hanging pulmonary distress on the outcome. Conclusion The incidence of pulmonary distress in survivors of nonlethal hanging is much higher than that reported in existing literature. The P/F ratio at presentation can help determine prognosis and decision making on further clinical and resource management. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09010t1.jpg] |
| |||||||||

{kind=link}