 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
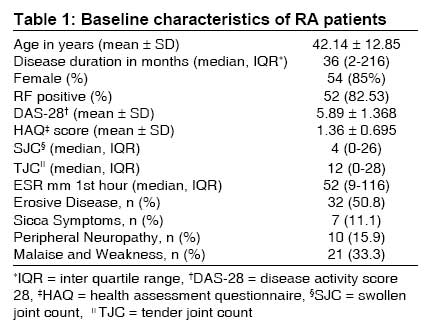
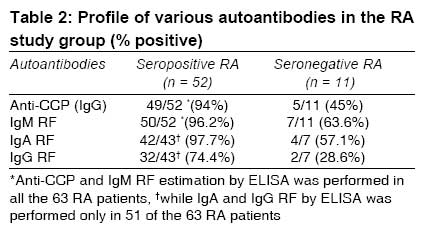
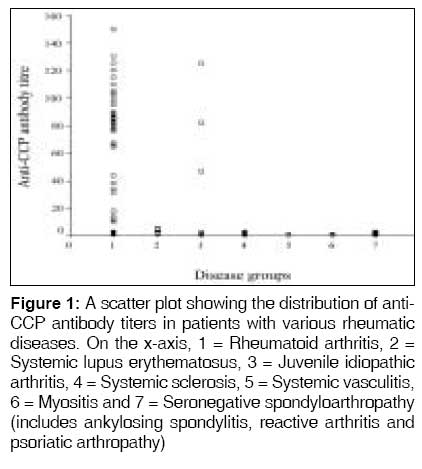
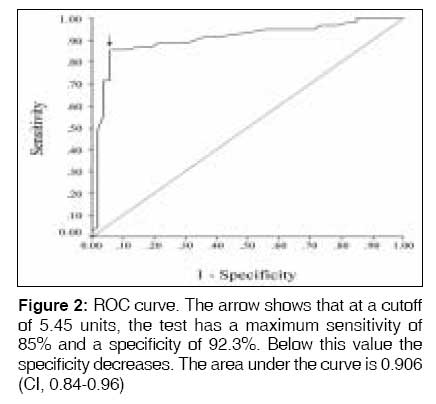
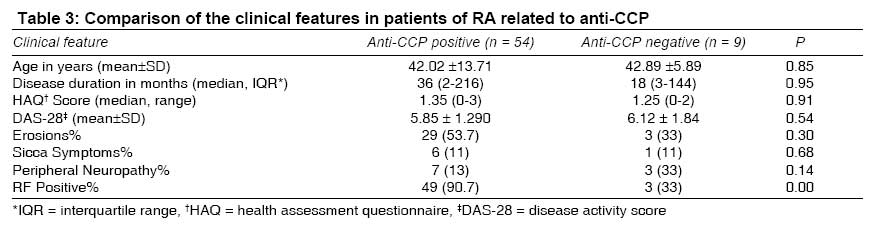
Indian Journal of Medical Sciences, Vol. 63, No. 3, March, 2009, pp. 92-100 Original Article Usefulness of anti -CCP antibodies in rheumatic diseases in Indian patients Gupta Rajiva, Thabah MollyM, Aneja Ritu, Kumar Ashok, Varghese Titus, Chandrasenan PJ Department of Medicine, All India Institute of Medical Sciences, New Delhi-110 029 Code Number: ms09019 Abstract Background: The usefulness of anti-cyclic citrullinated peptide antibodies (anti-CCP antibodies) to identify rheumatic arthritis (RA) from other rheumatic diseases presenting with joint pain is not well studied. Keywords: Anti-CCP antibodies, juvenile idiopathic arthritis, psoriatic arthritis, rheumatoid arthritis, rheumatoid factor, scleroderma, systemic lupus erythematosus Introduction Rheumatoid arthritis (RA) is a systemic inflammatory disease characterized by chronic and erosive polyarthritis with irreversible joint disability. Criteria in use for nearly two decades are not so useful in the diagnosis of early RA. [1] The early diagnosis of RA is essential, as it has been observed that progression occurs within 2 years of disease onset and if not aggressively treated early, joint destruction is irreversible. [2],[3] Therefore, the concept of window of opportunity is applied in the management of RA, where aggressive treatment during the early phase is more likely to succeed than when the same treatment is applied later in the course of disease. [4] However, RA patients are often difficult to diagnose early because they do not always show typical symptoms and signs and they may not fulfill the ACR (American college of Rheumatology) classification criteria. The ability to identify patients who will have progressive, erosive disease remains an objective because this subset will benefit the most from early aggressive treatment. In search for a marker to identify patients who will develop progressive, erosive disease, a system of various antibodies has been developed among which the rheumatoid factor (RF) has served both to support the diagnosis and as a marker of severity of disease since it was first recognized 50 years back. [5] The RF assay is 54% to 88% sensitive and 48% to 92% specific, and it is frequently detected in other disease states such as hepatitis and other connective tissue diseases. [6],[7],[8],[9] Therefore, even though the presence of RF remains one of the ACR classification criteria for RA, its diagnostic value is unsatisfactory, especially in early disease. Among the new antibodies described in the recent years in patients with RA, anti-cyclic citrullinated peptide (anti-CCP) antibodies are very specific for RA. These antibodies bind to antigenic determinant containing the unusual amino acid citrulline, formed by post-translational modification of arginine. [10],[11] Such determinants have been found in various proteins such as fillagrin, vimentin and fibrinogen. Although a number of studies have assessed the role of anti-CCP antibodies assay in the diagnosis of RA, the ability of this assay to differentiate an RA patient from another rheumatic disease patient has not been adequately addressed. [12],[13],[14] Because the usefulness of this assay largely rests in distinguishing RA from other rheumatic disorders, we aimed to assess the diagnostic accuracy of the anti-CCP antibodies assay to separate RA patients from a group of patients with diverse rheumatic diseases, and thus find the sensitivity and specificity of anti-CCP antibodies in RA. There are no published data on this issue from India. Second, we wanted to find out the prognostic value of anti-CCP antibodies and the serosubtypes of RF (IgA, IgM and IgG) in Indian patients with RA. Materials and Methods Study Design - This was a single center, cross-sectional case-control study. Patients - Patients with rheumatic diseases having joint pain as a symptom attending the Rheumatology Clinic of the All India Institute of Medical Sciences (AIIMS), a tertiary care center in North India, were invited to participate in the study. Their demographic details were recorded, which includes the diagnosis, duration of disease, age at onset, extra-articular manifestations and prior treatment. All patients provided written consent to participate in the study and the institute ethics committee approved the study protocol. Two groups of patients enrolled in the study. RA Group - Newly diagnosed RA patients as defined by the 1987 ACR criteria. [1] RA patients′ disease activity was assessed using Disease Activity Score-28 (DAS-28) and daily life function was assessed with the Indian version of Health Assessment Questionnaire (HAQ). [15],[16],[17] All patients with RA underwent nerve conduction studies (as part of another project). Non-RA Group - Patients with other rheumatic diseases, diagnosed by applying the respective ACR criteria; Ankylosing spondylitis (AS), n = 7; juvenile idiopathic arthritis (JIA), n = 10; psoriatic arthritis (PsA), n = 4; reactive arthritis (ReA), n = 2; systemic lupus erythematosus (SLE), n = 10; scleroderma (SSc), n = 8; systemic vasculitis, n = 3; myositis, n = 4 and others (adult onset Still′s disease, primary Sjogren′s syndrome and overlap syndrome), n = 3. The duration of disease did not affect the inclusion of patients in this study. All patients had joint pain and synovitis at presentation. Methodology - Sera were stored at -70° and tested for sero subtype of rheumatoid factor (IgG, IgM and IgA) and anti-CCP antibodies in one sitting after the recruitment of patients was complete. Anti-CCP antibodies were tested by a commercially available enzyme-linked immunosorbent assay (ELISA) kit (Euroimmun, Germany), which is a second-generation anti-CCP assay. A reading> 5 units was considered positive as per manufacturer guidelines. Rheumatoid factor was test by latex agglutination for the IgM isotype and also by ELISA (Euroimmun, Germany) for IgA, IgM and IgG isotypes. RA patients positive or negative for RF, as tested by latex agglutination are termed as seropositive and seronegative, respectively. Radiological assessment was done in radiographs of both hands and feet, using modified Larsen score in patients with RA. [14] Patients were classified as having erosive and non-erosive disease. Statistical Analysis Statistical analysis was performed using SPSS statistical software version 11.5. The sensitivity and specificity were calculated for anti-CCP. A receiver operating characteristic (ROC) curve was generated by plotting sensitivity (x-axis) against 1- specificity (y-axis) to calculate cutoff values for optimal sensitivity and specificity. In order to compare the clinical characteristics in subgroups of RA patients positive or negative for anti-CCP antibodies, χ2 test was used for categorical variables. Student t test was used to compare means. Non-parametric tests (Mann Whitney) were used to compare variables, which were not normally distributed, and P < 0.05 was considered significant. Correlation between quantitative variable was assessed by Pearson correlation coefficient. Results A total of 114 patients with various rheumatic diseases were included in the study between 2003 and the end of 2005. All these patients had joint pain as one of the clinical presentation. There were 63 RA patients and 51 patients with non-RA rheumatic diseases. The mean age of the RA patients was 42 years (±12.85) and median duration of disease was 36 months (range, 2 months-18 years). The clinical characteristics of RA patients are summarized in [Table - 1]. Radiographs of hands and feet showed erosions in 50.8% of the patients. Apart from erosions, other extra-articular features seen include Sicca symptoms (11.1%) and peripheral neuropathy (proven by electrophysiological studies) in 10 patients (15.9%). None of the patients had interstitial lung disease, pulmonary nodules, vasculitis, cutaneous nodules, Raynaud′s phenomenon, scleritis or lymphadenopathy. Profile of Various Autoantibodies in the RA Study Group Fifty-two of the 63 RA patients (82.53%) were rheumatoid factor positive (>32 IU/ml) by latex agglutination assay and 11 patients (17.47%) were seronegative. Among the seropositive group, almost all were positive for anti-CCP antibodies (IgG), IgA-RF and IgM-RF by ELISA. Among the seronegative group, antibodies to anti-CCP and the various RF isotypes could be demonstrated in 45% of patients. Details of the autoantibody profile are given in [Table - 2]. Diagnostic Accuracy of Anti-CCP in RA Fifty-four of 63 RA patients (85.71%) were positive for anti-CCP, while 9 patients tested negative for anti-CCP antibodies. In the non-RA group, anti-CCP antibody was positive in only 5 of 51 (9.8%) patients; these were 3 patients of JIA (2 polyarticular and 1 systemic onset) and 2 patients of SLE. The JIA patients were positive for anti-CCP with very high titers (46.5, 125 and 82 units), while the SLE patients were positive with low titers (5.1 and 5.8 units). The cutoff is 5 units [Figure - 1]. Our study found a sensitivity of 85% and a specificity of 90.19% with regard to the use of anti-CCP antibodies assay in patients with synovitis and joint pain to correctly identify RA. The optimal cutoff value was determined by means of the ROC curve [Figure - 2]. At a cutoff value of 5.45 units, the assay has a sensitivity of 85% and a specificity of 92.3%. Below this value it loses its specificity. The area under the curve was 0.906 (CI, 0.84-0.96). P With Clinical Features of RA We compared the clinical features including the presence of erosions and extra-articular manifestations (peripheral neuropathy, malaise and weakness and Sicca symptoms) of RA patients with respect to anti-CCP antibody positivity and found no significant differences [Table - 3]. In the RA patient group, the mean titers of anti-CCP antibody in the erosive and non-erosive group were comparable (69.44 vs 68.9 units, P = 0.9). The median duration of disease was significantly longer in the erosive group (23.66 months) compared with that in the non-erosive group (40.08 months, P < 0.001). There was no correlation between the titers of anti-CCP antibodies and duration of disease (r = 0.04) or DAS-28 scores (r = 0.038) and HAQ scores (r = 0.006). Association of the RF Sero Subtypes With Clinical Features of RA Similarly, there was no significant association between the IgA-RF and IgG-RF sero subtype positivity and clinical variables such as erosive disease; ESR; HAQ scores; DAS-28 scores; extra-articular manifestations such as peripheral neuropathy, malaise and weakness; and Sicca symptoms. However, there was a significant association found between IgM-RF positivity and erosions. Thirty-two of the 57 IgM-RF-positive patients (56.1%) had erosions, while no patient (0/6) had erosions in the IgM-RF-negative group (P < 0.01). There was no correlation between the age of patient, disease duration, DAS-28, HAQ scores with titers of anti-CCP antibodies and RF isotypes in RA. Discussion The diagnostic specificity of anti-CCP in RA has been shown. Anti-CCP antibodies are highly specific (>90%) in the diagnosis of RA even though the sensitivity ranges from 33% to 87%. [8],[9],[10],[11],[12],[18],[19] The second-generation assays for detecting anti-CCP antibodies increased the sensitivity to 80% while retaining the specificity. [12] Anti-CCP antibodies are important for diagnosis in RA because they are as sensitive as and more specific than the IgM RFs in early and fully established diseases. In addition, they may predict the eventual development into RA when found in undifferentiated arthritis and they may be detected in healthy individuals′ long before onset of clinical RA. [19],[20],[21],[22] Anti-CCP antibodies and RF are superior to several genetic markers in predicting the diagnosis of RA from undifferentiated arthritis in early arthritis patients. [23] Anti-CCP antibodies can be found at a very early stage in patients of RA and their presence correlates with the development of erosive disease. The combination of anti-CCP antibodies and IgM-RF has been found to have a high positive predictive value for RA. [19] Most of these studies had a normal group as the control population and a few other studies used patients with other rheumatic diseases as the control group. [8],[13] In this study, we compared the diagnostic specificity of anti-CCP antibodies in RA with respect to patients who have rheumatic diseases other than RA. Bizzaro et al. found anti-CCP antibodies to be 41% sensitive and 97% specific in diagnosing RA compared to patients with other rheumatic diseases. The diagnostic specificity of anti-CCP antibodies in RA found in our study is comparable to figures from previous studies. [8],[9],[12],[19] We found a much higher sensitivity when compared to other studies probably because our patients already had established RA at diagnosis, as opposed to previous studies where the test had been performed in patients with early arthritis. The low frequency of anti-CCP antibodies in the non-RA group, leads us to conclude that a patient with joint pain with anti-CCP antibodies positivity is most likely to have RA rather than a different rheumatic disease. It is worth noting that among the patients positive for anti-CCP antibodies in the non-RA group, patients with JIA were positive with very high titers. All these patients had polyarticular JIA, erosions and were also seropositive. Therefore, they behaved like adult RA patients. [24] Five of the 11 seronegative patients were also positive for anti-CCP antibodies. Therefore, a positive anti-CCP antibody supports the diagnosis of RA when RF is negative in the appropriate clinical setting. Thus, anti-CCP antibody serves as a better diagnostic marker in the diagnosis of RA, especially to detect the seronegative group. The determination of anti-CCP antibodies is important for prognosis. Previous studies have found that anti-CCP antibody positivity is associated with higher probability of erosive disease in long-term follow-up studies. [25],[26],[27] Kroot et al reported anti-CCP positivity in 70% of 273 RA patients and after 6 years of follow-up, patients who were anti-CCP positive at entry had more radiological damage. Similarly, Schellekens et al. found that both anti-CCP antibodies and IgM RF positivity at first visit predicted erosive changes after 2 years of follow-up. [11] Some studies have shown that anti-CCP antibodies were not associated with severe disease (erosions on radiographs). In a study of 106 patients with early arthritis, patients with anti-CCP antibodies positivity did not have significant erosions, while anti-Sa-positive patients had a higher incidence of erosions. [28] In our study, we found that anti-CCP antibody positive patients did not have any significant erosion on plain radiograph when compared with the anti-CCP antibodies seronegative group. This is probably because our study is cross-sectional and the sample size is small; patients need to be followed up to see how they behave in the long run. A recent cross-sectional study of 211 predominantly seronegative established RA subjects from our institute did find more erosion in the anti-CCP antibody-positive RA patients, and anti-CCP antibody-positivity was found to be an independent predictor of erosive disease in the seronegative group. [29] The reason for this discrepancy could be due to a selection bias. Most of our patients (84%, i.e., 53 patients) had disease duration of < 5 years. Four patients had disease duration between > 5 to 10 years, and in 6 patients disease duration was > 15 years. However, we did find that IgM-RF-positive patients had significant erosions on plain radiographs of hands and feet compared to the IgM-RF-negative group. But, IgM-RF is well known to be associated with erosions and more severe extra-articular manifestations. [13] In conclusion, a positive anti-CCP antibody is highly specific and moderately sensitive for RA in Indian patients. A positive anti-CCP antibody results in seronegative RA patients, and strongly supports the diagnosis of RA serologically. Anti-CCP antibodies were not useful in predicting clinical features and severity in RA patients in this study. However, a significant association was found between IgM-RF isotype and erosions. Anti-CCP antibodies may serve as a better diagnostic marker than RF in Indian population, especially in patients with synovitis of unclear etiology. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09019t3.jpg] [ms09019f1.jpg] [ms09019f2.jpg] [ms09019t2.jpg] [ms09019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}