 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
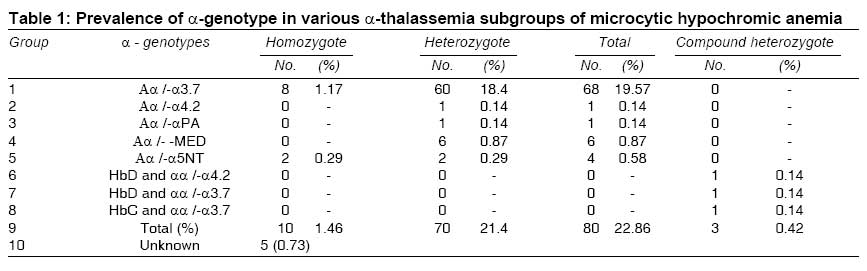
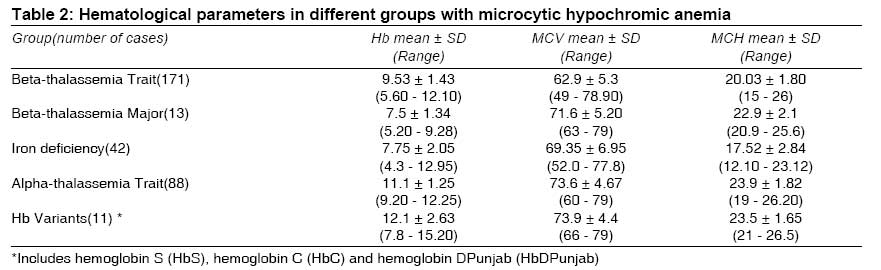
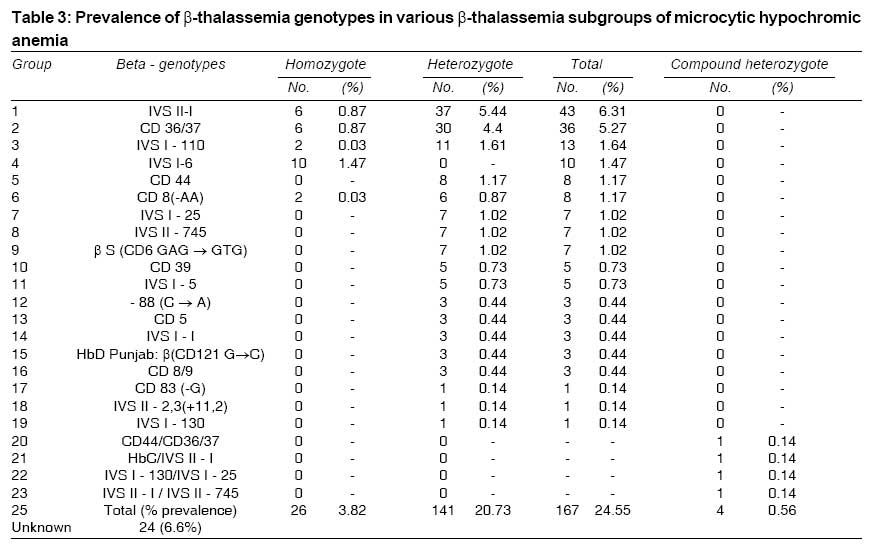
Indian Journal of Medical Sciences, Vol. 63, No. 3, March, 2009, pp. 101-108 Original Article Microcytic hypochromic anemia patients with thalassemia : Genotyping approach Rahim Fakher Research Center of Thalassemia and Hemoglobinopathies, Physiology Research Center, Ahwaz Jondishapur University of Medical Sciences, Ahwaz Code Number: ms09020 Abstract Background: Microcytic hypochromic anemia is a common condition in clinical practice, and alpha-thalassemia has to be considered as a differential diagnosis. Keywords: Alpha-gene deletions, beta-gene mutations, evaluation of anemia, microcytic hypochromic anemia Introduction Iran, a country 1,648,000 km 2 in area, has a large number of thalassemia patients like many other countries in the region. [1] Iranian population is a mixture of different ethnic groups; hence frequency and distribution of a-globin mutations in various regions of the country need to be clarified. In a country like Iran, with a remarkable prevalence of α- and β -globin mutations, the increased likelihood of co-inheritance of α- and β -thalassemia may result in a large variety of phenotypes. [2] The gene frequency of β -thalassemia, however, is high and varies considerably from area to area, having its highest rate (of more than 10%) around the Caspian Sea and Persian Gulf. Unlike β -thalassemia trait and iron deficiency, no simple biochemical test can detect α-thalassemia. There is a paucity of data on α- and β -genotyping in Iran. The key to successful detection and characterization of the hemoglobinopathies, particularly the thalassemias, is the initial hematological data. The clue for thalassemia is low mean corpuscular volume (MCV) or low mean corpuscular hemoglobin (MCH). Although iron deficiency is the other explanation for a low MCV or a low MCH, it is likely that this finding will point to thalassemia in regions of countries with at-risk ethnic populations. There are several causes of the anemia produced by different abnormal hemoglobins. In general, the anemia is both dyserythropoietic and hemolytic. In some, like HbS, the cause is apparent as lowering of oxygen tension leads to a process known as ′sickling′ of the red cells, making them more susceptible to destruction by the spleen. Red cell indices are taken to be the differentiating factor in anemias due to thalassemias and those from iron deficiency and are very necessary as both occur in the same areas. Relative increase in red cell count in thalassemias gives reduced MCH and MCV values. Microcytic hypochromic anemia is a common hematological abnormality in clinical practice and usually is caused by iron deficiency and thalassemia trait. The degree of microcytosis and type of mutation in thalassemias have shown wide variations in ranges of MCV. There is limited data reported in the literature for prevalence of α-gene deletion in patients with microcytosis. [3],[4] Carriers of a-gene deletion have mild microcytosis with or without anemia. Although anemia is absent or unremarkable, it is important to diagnose a-thalassemia in order to diagnose the cause of microcytosis and to avoid repeated expensive analysis and/or prolonged iron therapy. The coexistence of a-deletions in β -thalassemia patients modifies the phenotype. So far, no biochemical diagnostic test is available for detection of α-thalassemia carriers. Globin chain synthesis studies are time-consuming and expensive, and require radioactive amino acids for analysis. Molecular methods like southern blot hybridization and sequencing are conventionally used for diagnosis of α-thalassemia. However, molecular diagnosis by PCR has proven to be less time-consuming and less expensive, with a more definite outcome in the clinical setup. [5],[6] The most widely used method in detection of β -thalassemia′ mutation is the amplification refractory mutation system (ARMS). [7],[8],[9] Unlike the β -thalassemias, deletions are a common cause of α-thalassemia. The common α-thalassemia deletions and rearrangements can be routinely detected using gap-PCR. [10],[11] The present study was aimed to identify the prevalence of thalassemia mutation and hemoglobin variants in unexplained microcytic anemia cases and its utility in clinical practice, with special reference to genetic counseling. Materials and Methods Blood samples of volume 2 mL each were collected in EDTA vials and in plain vials from 340 patients (4 mL per patient) referred to the Research Center of Thalassemia and Hemoglobinopathies (RCTH), which is the only center working on hematology and oncology in the southwest (Khuzestan) region of Iran, between January 2004 and April 2007. Written consent was obtained from all the patients before collecting blood, which is a part of the procedure for obtaining ethical clearance from the institute. Red cell indices were measured on an automated cell counter (Sysmex Kx-21, Japan). Hb A2 and Hb F were measured in the Hb variant [Bio-rad, USA] system by using the thalassemia short program. The serum iron binding capacity and total iron binding capacity (TIBC) were measured by using kits (Span Diagnostics Ltd.) and percent saturation was calculated accordingly. The patients with iron saturation < 16% were considered iron-deficient. For α- and β -genotyping, genomic DNA was prepared from peripheral blood by the standard phenol chloroform extraction method. We analyzed all 88 patients who were suspected of having α-thalassemia on the basis of direct mutation analysis of α-globin gene by gap-PCR. We also analyzed all 171 patients who were suspected of having β -thalassemia on the basis of direct mutation analysis of β -globin gene by amplification refractory mutation system (ARMS). In case of some mutations such as poly A and -α5NT , the genotyping was done with the help of other techniques such as RFLP and ARMS-PCR. Documentation of the results was done on the gel documentation system (Alpha Innotech Corporation, USA). The protocol followed for the detection of -α3.7 deletion and -α4.2 deletion was as described by Agarwal et al.[6] For detection of other deletions, Liu et al.[12] method was followed. The amplified products were electrophoresed on 1.5% agarose gel (Sigma) and stained with ethidium bromide. Statistical Analysis Statistical analysis was carried out using Statistical Package for Social Sciences version 11.5, and an independent-sample t test was used for comparison of hematological parameters. Genotypic and allelic frequencies were also calculated. Results The initial analysis of hematological parameters was done on 340 samples. Following the initial evaluation based on the previous described hematological parameters, out of the total 340 samples, 325 were diagnosed as microcytic [MCV < 80 fl] hypochromic [MCH < 27 pg mL-1] anemia and subjected to a thalassemia study. These included 171 with beta-thalassemia trait, 88 with alpha-thalassemia trait, 13 with thalassemia major, 11 with hemoglobin variants (HbS, HbC and HbD Punjab ), 42 with iron deficiency anemia and the remaining 15 patients with no definite etiology, listed in [Table - 1]. In 283 samples, hemoglobinopathy was found. Of the remaining 57 samples, 42 showed iron deficiency anemia, which was diagnosed by "percentage of saturation" technique. However, no definite etiology was confirmed in 15 patients. Hematological parameters of patients in different groups are shown in [Table - 1]. Only, there was a statistically significant difference between beta-thalassemia trait and beta-thalassemia major with regard to MCV (P < 0.05) and MCH (P < 0.05) indices, and also MCH index between beta-thalassemia trait and Hb variants (P < 0.05). There was no statistically significant difference in the red cell indices in the remaining hemoglobinopathies. We analyzed all 88 patients who were suspected of having a-thalassemia and found the types of mutations, which are listed in [Table - 2]. We also analyzed all 171 patients who were suspected of having β -thalassemia and found the types of mutations, which are listed in [Table - 3]. Among the 88 patients with microcytic hypochromic anemia, 60 patients had heterozygous -α3.7 deletion [-α3.7 / α α] whereas 4 patients had homozygous -α3.7 deletion [-α3.7 / -α3.7 ]. Allele frequency for -α3.7 deletions was calculated as 0.10 (70 in 680 chromosomes). All 195 samples were analyzed for β -gene number by amplification refractory mutation system (ARMS). The most frequent mutations were IVS II-I, CD 36/37 and IVS I-110 with frequencies of 6.31%, 5.27% and 1.64%, respectively. The percentage of unknown genotypes was found to have a value of 0.73% for α-globin and 6.6% for b-globin. Discussion Alpha- and beta-thalassemia are the commonest single-gene hemoglobin disorders in the world. [13],[14],[15] The commonest type of α-thalassemia seen in Iran is -α3.7 deletion. At our hospital, the overall frequencies of α-thalassemia and β -thalassemia among microcytic, hypochromic anemia patients are 57% and 25.8%, respectively Hadavi et al.[16] have reported the prevalence of -α3.7 deletion to be 30.2% in the population of Iran (87 million). Our data showed the prevalence of -α3.7 deletion to be 20% in the population of southwest (Khuzestan) region of Iran (4.3 million). Also, in our search, we found only 2 cases of -α4.2 deletion and few cases of other deletions reported so far. Hadavi et al.[16] have reported -α4.2 deletion in Iranian subjects, with a prevalence of 3.5%. Najmabadi et al.[17],[18] have reported the prevalence of IVS-II-I (G > A) beta-thalassemia mutation to be 34% in the population of Iran. Our study showed most frequent mutations were CD 36/37, IVS II-I and IVS I-110 with frequencies of 9.7%, 11.7% and 3.5%, respectively, followed by cases of other mutations reported so far. Hematological parameters in patients with a-thalassemia were compared with those in patients with iron deficiency anemia and β -thalassemia. Individuals with the single-gene deletion (-α3.7) have lower levels of hemoglobin, MCV and MCH as compared to normal controls. The carriers of a-thalassemia and Hb variants have a mild microcytic hypochromic anemia. However, their MCV and MCH are better than those of patients with iron deficiency anemia. MCH is a better discriminator than other red cell indices in the diagnosis of α-thalassemia, which is usually less than 26 pg. Since there is no definitive hematological marker that can give the diagnosis of a-thalassemia, molecular analysis remains the only diagnostic approach in microcytic hypochromic anemia patients. Our findings are in concordance with previous reports, where microcytosis was explained on the basis of α-gene number. [3],[19],[20],[21],[22] The identification of α- and β -thalassemia carrier status is important to prevent erroneous and expensive investigations to define the etiology of anemia, as well as prevent unnecessary prolonged iron supplementation. The knowledge of α- and β -gene numbers in α- and β -thalassemia traits in any population is necessary, as it modifies the phenotype of thalassemia by altering the ratio of α- and β -chains of hemoglobin. Thus screening for thalassemia should be considered during genetic counseling of couples at high risk of thalassemia, for prenatal diagnosis. Recently, Li et al.[23] have described a simple and reliable method that can meet the requirements of direct genotyping of known β -thalassemia mutations and/or polymorphisms in the clinical setting for Chinese population and, in general, as a model for other populations. They categorized a total of 61 amplicon-based DHPLC patterns from 795 blood samples and prenatal archival samples with various Chinese β -thalassemia mutations and/or normal β -globin polymorphic variations. They showed that all 20 β -thalassemia heterozygous mutations and 9 β -thalassemia compound heterozygous mutations or homozygous mutations, which were contributed by 13 patterns of disease-causing mutations alone and 36 patterns of disease-causing mutations in combination with polymorphisms, existed in 3 fragments; they were identified by using heteroduplex analysis. Glynou et al.[24] have genotyped the β -gene mutations using a method that comprises of the duplex PCR that produces fragments encompassing with unpurified amplicons, and microtiter well-based assay of extension products with a peroxidase-antifluorescein conjugate and a chemiluminogenic substrate. They standardized the method by analyzing 60 samples with known genotypes and then validated the same by blindly genotyping 115 samples with 45 genotypes. They claimed that the results were fully concordant with sequencing, and the method is accurate, reproducible and cost-effective in terms of equipment and reagents. Hung et al.[25] used 2 highly-specific mutation-screening methods - mismatch-specific endonuclease and denaturing high-performance liquid chromatography - to identify mutations in the hemoglobin gene. They successfully distinguished mutations in the hemoglobin gene by the mismatch-specific endonuclease method without need for further assay. This technique had 100% sensitivity and specificity for the study sample. The most widely occurring single-gene deletions are the -α3.7 and the -α4.2 . The double α-gene deletions in cis, such as the -- SEA, -- FIL and - THAI, are most common in Southeast Asia, while the -- MED and the --20.5 double-gene deletions occur most frequently in the Mediterranean area. [3] Inheritance of 2 functional gene deletions such as - MED is very rare, especially in our area. We could determine many cases that show these mutations in our study. In conclusion, identification of rare thalassemia gene mutations in our population is necessary because of the country′s multiracial population and high frequency of interracial marriages. Obviously the commonly used methods were not sufficient to detect the entire spectrum of globin gene mutations occurring in this area, which led to a fairly high percentage of unknown genotypes. The use of more comprehensive diagnostic tools (as DNA sequencing or commercially available strip assays) would have shed more light on the unresolved cases. Although traditional molecular techniques, such as RDB, ASO, LCR and ARMS, give unequivocal results, they are only useful for identifying a limited number of known mutations and require careful optimization, especially in cases of unknown mutations. Drawbacks of using traditional detection techniques in routine diagnosis are instrument cost, time of analysis and disability to detect unknown and rare mutations. However, modern DNA-sequencing technology has increased read length and throughput, with reduction of cost to support their application in hematogenetics and gene function study. [26],[27] Acknowledgment This work was supported by the director of Shafa Hospital and the Department of Hematology and Oncology. The author thanks the patients and their families. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09020t1.jpg] [ms09020t2.jpg] [ms09020t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}