 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
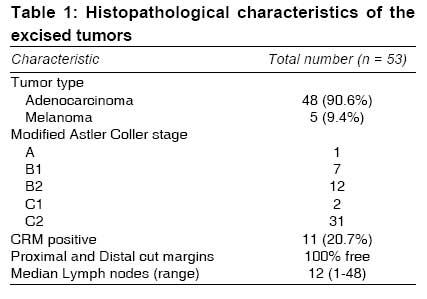
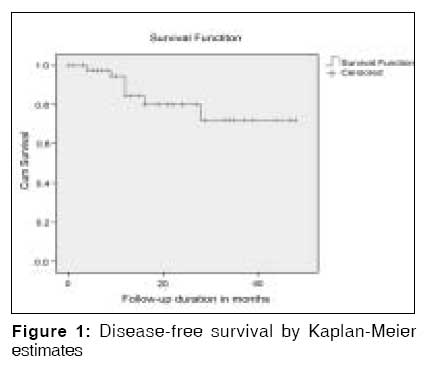
Indian Journal of Medical Sciences, Vol. 63, No. 3, March, 2009, pp. 109-114 Original Article Feasibility of laparoscopic abdomino - perineal resection for large - sized anorectal cancers : A single - institution experience of 59 cases Shukla ParulJ, Barreto SavioG, Hawaldar Rohini, Nadkarni Mandar, Kanitkar GajananA, Kerkar Rajendra, Shrikhande ShaileshV Department of Gastrointestinal Surgical Oncology, Tata Memorial Hospital, Mumbai Code Number: ms09021 Abstract Background: Laparoscopic surgery for anorectal carcinoma is steadily gaining acceptance. While feasibility has already been reported, there are no reports addressing the impact of the actual size of large tumors on laparoscopic resectability . Keywords: Circumferential resection margin, laparoscopy, rectal cancer Introduction Heald et al.[1],[2] have stated that total mesorectal excision (TME) is probably the most important factor determining better outcomes. The ability to perform a complete TME has been shown to be technically easier in case of laparoscopy. [3] However, laparoscopy for rectal cancer has been accepted the world over with less enthusiasm than for colon cancer. The reason for this has been the fear of high circumferential resection margin (CRM) positivity encountered with rectal cancers during anterior resection. [3] However, in the case of LAPR, Baker et al.[4] have claimed that there was no difference when open surgery was compared with laparoscopy with regard to CRM positivity. It is known that the absence of mesorectum in the lowest 3 cm of the rectum renders the prognosis associated with such tumors to be poorer as compared to higher rectal tumors. This is the exact reason why in low-lying tumors, especially those reaching the anal canal, the performance of a more precise sharp dissection from the abdomen is of utmost importance. The anterior sharp dissection reduces the amount of dissection required to be performed from the perineal side, reducing the tearing of the perirectal fascia and the associated dissemination of cancer cells into the perineum. [1],[2],[5],[6] While studies have been published on the feasibility of the procedure, addressing issues such as laparoscopic surgery in the complicated patient, [7] a factor that has not been given much importance in relation to the outcome of the procedure is the size of the lesion. While most published manuscripts do comment on the stage of the tumor, the actual size of the tumor is not mentioned. This determinant may play a role in defining the feasibility and the outcome of the surgery. We have reviewed our own data to address this issue. Materials and Methods The records of all patients who underwent LAPR for very low rectal cancers at the Department of Gastrointestinal Surgical Oncology between 1 st January 2003 and 31 st December 2006 were included in the study. Preoperatively, all patients were investigated in the same manner with routine blood investigations, including blood counts, liver and renal functions, ECG and tumor marker (CEA). Preoperative evaluation included a digital rectal examination and colonoscopy. All patients underwent a contrast-enhanced multi-detector CT (MDCT) imaging for tumor staging preoperatively. All patients had bowel preparation with polyethylene glycol and were given prophylactic antibiotics on induction of anesthesia. The LAPR was performed as described by Pikarsky et al.[8] A circumferential resection margin (CRM) of ≤ 2 mm was considered positive. [9] Perioperative mortality was defined as deaths taking place while the patient was still hospitalized. Deaths were included irrespective of whether they arose as a result of the surgery or other causes (i.e., to include cardiac-related deaths). The total hospital course was defined as the entire period of hospitalization from the date of surgery until the patient was discharged. Patients were discharged only if they satisfied the following criteria: adequate pain control with oral analgesics, no nausea, ability to take solid foods, passage of flatus and / or stool, mobilization and self-support comparable to the preoperative level. Our postoperative follow-up consisted of history and clinical examination (scar, supraclavicular lymph nodes, per abdominal examination, perineal examination [for patients having undergone APR]) every 3 months for 2 years, then every 6 months for a total of 5 years. Serum CEA levels were measured at every visit stated above. Chest/abdominal/pelvic CTs were considered annually for 3 years for patients at high risk of recurrence. Colonoscopy was performed in 1 year. In patients in whom a preoperative colonoscopy was not performed due to an obstructing lesion, colonoscopy was performed within 3 to 6 months of surgery through the end stoma. PET scan was performed in patients with rising titers of CEA or in whom radiological evidence of recurrence was determined by chest x-ray or CT scan. All statistical analyses were performed using SPSS version 14.0 for Windows. Continuous data are expressed as mean ± standard deviation. The median has been used wherever applicable. Pearson′s correlation was used to assess correlation between tumor area and T-stage. One-way ANOVA was performed to find an association between tumor area and CRM positivity. The Kaplan-Meier method was used to estimate survival curves. Ninety-five percent confidence intervals (95% CIs) were calculated for the survival estimates. Results During the period between 1 st January 2003 and 31 st December 2006, 59 patients were taken up for LAPR. Patient Characteristics A total of 45 patients were classified as grade I; and 14 patients, as grade II by the American Society of Anesthesiologists (ASA) grading. These included 33 (55.9%) males and 26 (44.1%) females. The mean patient age was 46.8±15 (24-80) years. The average distance from the anal verge was 1.4±1.97 cm. Operative Factors Complete laparoscopic resection could be completed in 53 (89.8%) patients. The reasons for conversion included 1 case of bleeding from vaginal wall; 1 case of dense adhesions following a previous hysterectomy; and 3 cases of bulky disease involving adjacent structure, including the vagina and parametra and bladder (not predicted on preoperative imaging). In 1 case, conversion had to be resorted to due to technical difficulties with the equipment resulting in poor vision. The median operating time was 255 (45-470) minutes, with a median blood loss of 300 (20-1200) mL. Tumor Characteristics The mean tumor area measured at the time of histopathological examination as the length (craniocaudal axis) multiplied by the breadth (lateral margin to lateral margin) of the tumor, was 24±17.5 (4-83) cm 2 . The histopathological characteristics have been tabulated in [Table - 1]. Applying Pearson′s correlation, there was no correlation between area of the tumor and tumor T-stage (R=0.056, P = 0.713) Postoperative factors The morbidity rate was 9.4% (5/53). This included 2 cases of superficial perineal dehiscence necessitating secondary suturing, 1 case of complete perineal wound dehiscence with bowel evisceration necessitating emergency repositioning of the bowel and closure, 1 case of stomal retraction managed by local stomal refashioning, and 1 case of bleeding from the prostatic capsule requiring an emergency exploration via the perineal wound and hemostatic suture on the offending vessel. There was no mortality in the entire group. The mean duration of hospital stay was 10.0±1.9 days. Survival Data There were 7 recurrences - 2 local, 2 liver metastases, 1 case each of lymph nodal, peritoneal and cutaneous recurrences. As a result, the 48-month disease-free survival was 72% [Figure - 1]. There was no significant correlation between either the patient sex, tumor type (including degree of differentiation, T- or N-stage) or circumferential resection margin and disease-free survival. There was no significant correlation between tumor surface area and CRM positivity (P < 0.707). Discussion The advantage offered by laparoscopy has always centered on improved vision. This advantage seems to be put to best use in the case of rectal cancer surgery, where logistic impediments, viz., narrow pelvis and impaired visibility as the dissection proceeds caudad, have proved to be obstacles to colorectal surgeons during open surgery. Rectal cancer is seen to occur around a decade earlier in Indians, [10] the reasons for which are still uncertain. Our lymph nodes yield compares favorably to a worldwide series reporting yields of 11.5 to 14 lymph nodes per case. [6],[11],[12],[13] Our operating time (255 minutes), as well as average duration of hospital stay (10 days), is also comparable to other similar studies. [4],[6],[12],[13],[14],[15] Our morbidity rate of 9.4% is better than the reported morbidity rates following laparoscopic surgery for rectal cancers in other series. [13],[14],[15],[16] Similarly, our conversion rate of 9.4% is comparable to most studies (10%-21%). [14],[15],[16] The above data clearly reflect the technical feasibility of laparoscopy for very low rectal cancers in our setting. The factor that we wish to highlight, though, is not the technical feasibility but the oncological safety. We would like to consider for the first time the average surface area (size) of the tumor. In different parts of the world, patients present with advanced disease status the reasons of which are varied. Some common reasons for delayed presentations are misdiagnosis of bleeding per rectum as being hemorrhoidal in origin; and among patients who are diagnosed correctly, a substantial subset of patients seek alternative forms of therapy before presenting for surgery. As can be seen from the current study, our patients presented with large (average surface area of 24 cm 2 ) and often advanced malignancies (58.4% of the patients with C2 disease, in our study). These tumors pose a serious challenge to surgeons. The recommended surgical standards include clear margins, not only along the luminal length but also along the circumferential margin (CRM). This issue was briefly addressed in the MRC CLASICC trial. [1] Unfortunately, Korolija et al.[17] in their meta-analysis had compared, mainly, distal margins. Similarly, Pugliese et al.[6] only concentrated on the distal margins. The CRM seemed to have been ignored. The significance of radial clearance was first addressed by Quirke et al.[18] They claimed that recurrence was directly influenced by the involvement of the edge of mesorectal excision. This view was further supported by de Haas-Kock et al.[19] To prove that laparoscopy is as safe as open surgery for cancer of the rectum, we must be able to prove beyond doubt that margins of resection are comparable, if not better. [20] In our series, the CRM positivity was 20.7% - a value that is well within reported rates of CRM positivity (up to 25%) for curative resections. [9],[21] This, as has been explained in previous studies, is probably an indicator of the large size of the tumors as well as their advanced stage. It is important to note, though, that the oncological safety is not only dependant on the abdominal procedure but also on the adequacy of the perineal part of the operation. Besides, should tumor injury be detected intraoperatively, it is advisable to convert to open surgery to control the amount of contamination and complete the rest of the procedure. We have been gradually shifting towards the introduction of neoadjuvant chemo-radiotherapy protocols. [22] This has been difficult because our patient referral base is mainly from outside Mumbai. Conclusion The size of the tumor does not hamper the feasibility of performing LAPR. We need to consider the possibility of an increased CRM rate for large-size tumors. This may be addressed by preoperative radiotherapy and chemotherapy before undertaking surgery on these large tumors.Acknowledgment Ann Schloithe for help with the statistics. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09021t1.jpg] [ms09021f1.jpg] |
| |||||||||


{kind=link}
{kind=link}