 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
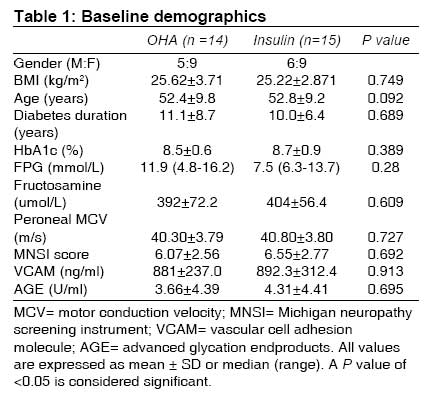
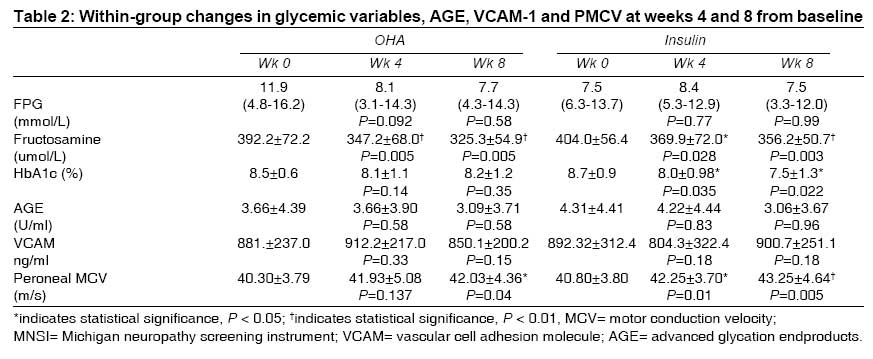
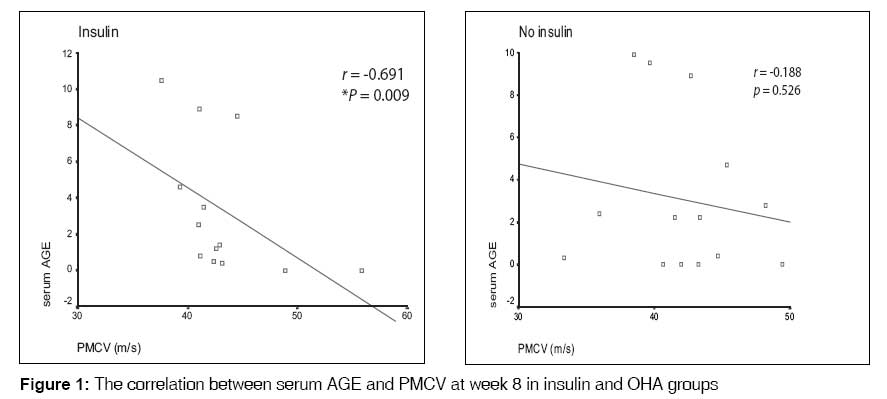
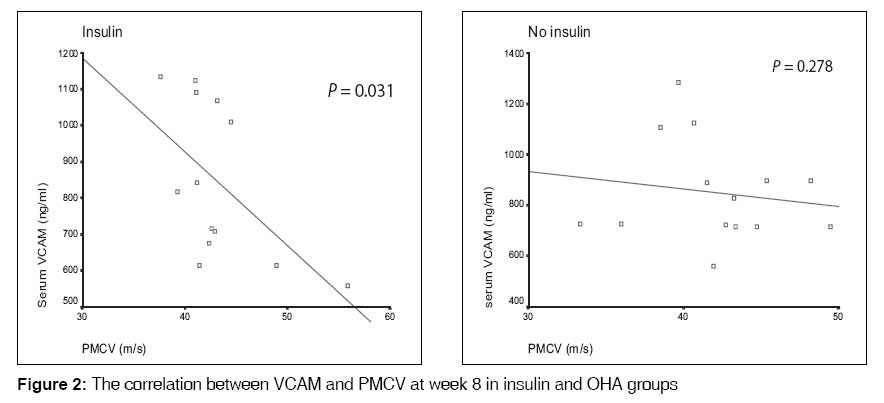
Indian Journal of Medical Sciences, Vol. 63, No. 4, April, 2009, pp. 131-138 ORIGINAL CONTRIBUTION The effects of short-term, rapid glycemic control on the peroneal nerve function and serum VCAM-1 and AGE in type 2 diabetic patients in Malaysia Norlinah MI, Hamizah R, Md Isa SH, Wan Nazaimoon WM, Khalid B.A.K Department of Medicine, Universiti Kebangsaan Malaysia Medical Center (UKMMC), Kuala Lumpur Code Number: ms09027 Abstract Background : The role of endothelial injury and circulating adhesion molecule in the development and progression of diabetic peripheral neuropathy in the long-term has been established previously. Aims:0 To study the effects of short-term glycemic control using insulin and oral hypoglycemic agent therapy (OHA) on the peroneal nerve function and vascular cell adhesion molecule-1 (VCAM-1) and advanced glycation endproducts (AGE) levels in type 2 diabetic patients. Keywords: Cell adhesion molecules, diabetic nephropathies Introduction Diabetic peripheral neuropathy (DPN) is an important microvascular complication of diabetes mellitus. Its prevalence among Malaysians is 50.7%, [1] which rises with age, the duration and severity of hyperglycemia. [1],[2],[3],[4] The pathogenesis of DPN is complex. [6],[7],[8],[9],[10] Endothelial injury, and the release of inflammatory mediators such as circulating cell adhesion molecules (CAMs) due to poor glycemic control have been implicated. [8],[9],[10],[11],[12],[13],[14] One study showed that these adhesion molecules were important long-term predictors of DPN. [15] Effects of glycemic control on the peripheral nerve function and these inflammatory markers in the short-term have not been well studied. We therefore conducted a study to compare the short-term effects of rapid glycemic control with insulin and conventional oral therapy on the peroneal nerve function and vascular cell adhesion molecule-1 (VCAM-1) and advanced glycation endproducts (AGE) levels in type-2 diabetic patients. Materials and Methods This was an 8-week prospective, single-blind study on poorly controlled type 2 diabetic patients attending a tertiary endocrinology outpatient center in Kuala Lumpur. Inclusion criteria included the following: age of 18 to 70 years inclusive; a body mass index (BMI) between 23 and 30 kg/m 2 ; and HbA 1c levels of 7.5% to 11.5% inclusive. Patients were excluded if they had compression neuropathy of the peroneal nerve at the fibula head or severe neuropathy such as Charcot joints or comorbidities such as cerebrovascular accident in the preceding 3 months. An informed written consent was obtained from all patients prior to enrolment. Randomization and treatment At baseline visit, patients were randomized by an endocrinologist to receive either insulin therapy using a combination of multiple daily injections of short-acting insulin (Actrapid) and long-acting insulin (Insulatard) (Novo Nordisk) or to continue on OHA therapy (sulphonylureas, metformin and/or acarbose) at maximal doses. Patients were followed up at 4-week intervals by an endocrinologist and a neurologist, for 8 weeks. Advice on diet and exercise was given to both groups at each visit. The assessing neurologist was blinded to treatment assignment. Patients were withdrawn from the study if they developed an acute, severe illness and/or if their blood sugar levels were found deteriorated to fasting plasma glucose (FPG)> 15 mmol/L on two consecutive visits. Laboratory assays Blood samples were taken at baseline, weeks 4 and 8 for FPG, fructosamine, HbA 1c , AGE and VCAM-1. The HbA 1c was measured using Bio-Rad VARIANT hemoglobin testing system. The FPG and fructosamine were measured using Cobas Integra 700. VCAM-1 was measured using the enzyme-linked immunoabsorbent assay (ELISA) technique from Bender Medsystems, Austria. The normal range for VCAM-1 was 395-714 ng/mL, and inter-assay coefficient of variation at 2043 ng/mL was 7.3%. The sensitivity of the assay was 2.0 ng/mL. Serum AGE was measured by an in-house immunoassay developed in our laboratory, which is similar to the method developed by Nakayama et al. [16] The inter-assay CV at 14.8 U/mL was 7%. Nerve conduction tests The right and left peroneal nerve motor conduction velocities (PMCVs) were measured at baseline and 4-week intervals. We used standard surface electrodes using a Medelec neurophysiology system (Medelec, Woking, UK). Proximal nerve stimulation was performed at the head of fibula; and distal stimulation, at the ankle. The compound motor action potential (CMAP) was recorded from the extensor digitorum brevis (EDB). The distance between the 2 stimulation points was kept constant at every visit. The mean PMCV was obtained from the average of the right and left PMCVs. Peripheral neuropathy was diagnosed if the PMCV was less than 39.5 m/s. The Michigan neuropathy screening instrument (MNSI) [17] was administered to all patients at each visit to determine the overall score of neuropathy. A higher score reflects a more severe neuropathy. Ethical considerations The study was approved by the Ethics Committee of our institution. Statistical analysis Data were analyzed using the statistical package for social sciences version 10.0 for Windows (SPSS, Inc., Chicago, IL). All data were tested for normality, and comparison within groups was done using paired t test and Kruskal Wallis test for parametric and nonparametric data, respectively. Comparison between groups was done using the unpaired t test or Mann-Whitney U test. Correlation was analyzed using Spearman′s correlation coefficient. A P value of < 0.05 was considered statistically significant. Results Twenty-nine patients were recruited; 15 received insulin and 14 received OHA. Twenty-seven patients received treatment up to week 8. Two patients on insulin withdrew after visit 1. Baseline characteristics At baseline both groups were comparable for age, duration of diabetes, HbA 1c , FPG, serum fructosamine, mean PMCV, serum AGE, serum VCAM-1 and MNSI scores [Table - 1]. Glycemic variables There were no significant changes in the FPG in both the treatment groups at weeks 4 and 8. The HbA 1c improved significantly in the insulin group at both weeks 4 (P = 0.035) and 8 (P = 0.022) compared to baseline. No significant changes were observed in HbA 1c levels in the OHA group at weeks 4 and 8. Serum fructosamine levels improved significantly in both insulin and OHA groups at weeks 4 and 8 compared to baseline [Table - 2]. Between-groups comparison showed no significant difference in all the glycemic variables measured. VCAM and AGE There were no significant changes in the plasma VCAM-1 or AGE levels at weeks 4 and 8 compared to baseline or when compared between the two treatment groups [Table - 2]. Peroneal nerve motor conduction velocity (PMCV) At baseline, 13 (44.8%) patients had neurophysiological evidence of peroneal neuropathy, with a mean PMCV of 37.3 m/s. Patients with neuropathy had higher serum VCAM-1 levels at baseline (993.25 ± 340.59 ng/mL vs. 811.76 ± 192.03 ng/mL), which was not significant. There were no significant differences in age, duration of diabetes, HbA 1c or serum AGE in those with or without neuropathy. The mean BMI in patients with neuropathy (23.9 ± 3.55 kg/m 2 ) was significantly lower than in those without neuropathy (26.53 ± 2.54 kg/m 2 ) (P = 0.011). Following treatment, there was a significant improvement in the PMCV in both insulin (P = 0.005) and OHA (P = 0.04) groups at week 8. However, the improvement in the insulin group was seen as early as week 4 (P = 0.01). There were no significant differences in the PMCV between the two treatment groups at weeks 4 and 8 [Table - 2]. Correlation between VCAM, AGE and PMCV Significant correlations between PMCV and AGE (r = -0.406; P = 0.009) [Figure - 1] and between PMCV and VCAM-1 (r = -0.443; P = 0.031) [Figure - 2] were observed at week 8. VCAM-1 correlated significantly with AGE at week 8 (r = 0.451; P = 0.016). Discussion This study showed that 44.8% of our patients had electrophysiological evidence of peroneal neuropathy at baseline. The mean MNSI score was 6.26 (±2.60), implying a moderate degree of neuropathy. This finding is not surprising as patients recruited had suboptimal glycemic control, with a mean HbA 1c of 8.6±0.75%. It must be emphasized that although this was a comparative study on the effects of 2 different treatment regimes, there were no significant between-group differences in glycemic control or peroneal nerve function. However, significant improvement in glycemic control was observed within each group following treatment. In both groups, the serum fructosamine levels improved significantly at week 4 of treatment as compared to the baseline levels. The HbA 1c , however, improved significantly only in the insulin group by week 4 and continued to improve over the 8-week period. One explanation is serum fructosamine may be a more reliable indicator of short-term glycemic changes in view of its shorter half-life compared to HbA 1c . [18] Alternatively, the degree of glycemic improvement in the OHA group may not have been substantial enough to result in significant changes in the HbA 1c . The lack of treatment-related differences in the glycemic indices between the two groups over the treatment period could be partly attributed to the small sample size, or alternatively may indicate that both treatments were equally effective in achieving glycemic control. Importantly, in line with the glycemic improvement within each group, the PMCV also improved progressively in both groups over the 8-week period when compared with baseline. However, in the insulin group, improvement in the PMCV occurred earlier, at week 4; while in the OHA group, it was observed only at week 8. This observation proves that improvement in PMCV parallels the improvement in glycemic control as patients on insulin achieved significantly better glycemic control by week 4 of treatment. Similarly, a previous short-term study on peroneal nerve function using intensive insulin therapy showed that rapid glycemic improvement over 35 days resulted in significant improvement in PMCV. [5] The role of circulating cell adhesion molecules (CAMs) in the development of diabetic microvascular complication has been established previously. An increase in the level of CAMs has been demonstrated in diabetic patients with microvascular disease. [13],[14],[15] In particular, a previous study on peroneal nerve function showed significant association between increasing levels of VCAM and worsening peroneal nerve function. [15] In our study, despite the lack of significant changes in the serum VCAM-1 levels with glycemic improvement in either group, patients with neuropathy had significantly higher VCAM-1 values at baseline compared to those without. [8],[9],[10],[11],[12],[13],[14],[15] We also found that an increase in VCAM-1 levels correlated with an increase in AGE, supporting findings from other studies which showed that AGE products result in the release of CAMs through interaction with the receptors for AGE (RAGE). [19] Interestingly, improvement in PMCV correlated significantly with improvement in serum VCAM-1 and AGE only in the insulin group. This is most probably due to the significantly better glycemic control achieved in the insulin group, rather than a unique insulin effect; although previous studies have suggested that insulin may have a protective effect on neurons independent of glycemic control. [20],[21],[22] However, we are unable to ascertain this on the basis of our study. One of the important limitations of this study is the small sample size, which may have affected some of the results. The short duration of study may also have affected some of the results, in particular the VCAM-1 levels. Additionally, only serum VCAM-1 was measured, which may be less sensitive than other soluble CAMs in predicting in vivo endothelial dysfunction. [23] This could partly explain the lack of significant changes in the VCAM-1 levels despite significant improvements in glycemic control and peroneal nerve function following treatment. In summary, this study found a high prevalence of subclinical peroneal neuropathy in diabetic patients with suboptimal glycemic control. Importantly, aggressive treatment of diabetes improves the peroneal nerve function, as early as 4 weeks. Therefore, all diabetic patients with suboptimal glycemic control should be screened for diabetic neuropathy and patients with subclinical neuropathy should be treated aggressively in the early stages, to prevent further progression of neuropathy. This study also showed that VCAM-1 may play a role in development of diabetic microvascular complications, in particular diabetic neuropathy. Perhaps, the use of VCAM-1 or other adhesion molecules as potential biomarkers in the progression and development of diabetic microvascular complications, coupled with proper cost-effectiveness analysis, could be explored in the future. Acknowledgment The authors are thankful to the dean of the medical faculty, Universiti Kebangsaan, Malaysia, for the funding provided. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09027t1.jpg] [ms09027f1.jpg] [ms09027t2.jpg] [ms09027f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}