 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
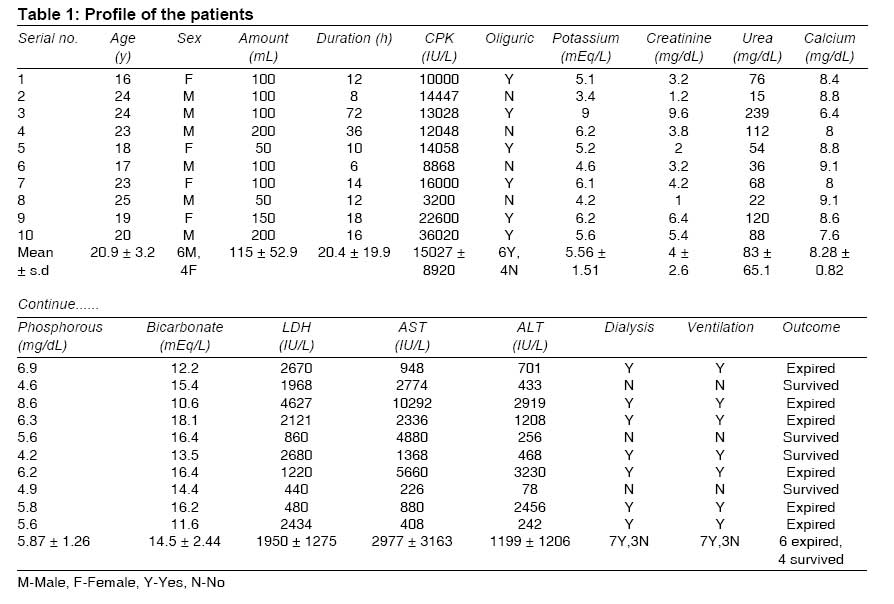
Indian Journal of Medical Sciences, Vol. 63, No. 4, April, 2009, pp. 164-166 Letter To Editor Systemic toxicity of paraphenylenediamine Soni SachinS, Nagarik AmitP, Dinaker Manjunath, Adikey GopalKishan, Raman Anuradha Department of Nephrology, Mediciti Hospitals, Hyderabad (AP) Code Number: ms09032 Sir, Paraphenylenediamine (PPD), a derivative of paranitroanaline, is commonly used in several industries like oxidizable hair dye, dyeing furs, photochemical processes and tyre vulcanization. The first documentation of systemic PPD poisoning in 1924 described the case of a hairdresser who developed toxicity from handling the dye. [1] Many reports have followed since then, mainly from developing countries. We report a series of 10 patients admitted over a period of 1 year at a tertiary care hospital in south India. Between January 2006 and February 2007, 10 patients (6 males, 4 females) of PPD (3.75%) ingestion in the form of hair dye, with suicidal intent, were admitted [Table - 1]. It accounted for < 0.1% of hospital admissions and 4.5% of acute renal failure (ARF) patients during the study period. Patients presented with features of severe hypersensitivity (itching, angioedema, asphyxia) and rhabdomyolysis (paresis of extremities, cola-colored urine, oliguria, markedly elevated creatinine phosphokinase and lactate dehydrogenase, hyperkalemia, hyperphosphatemia and hypocalcemia). ARF was observed in 8 (80%) patients. Patients were treated with gastric lavage, intravenous fluids, antihistaminics and steroids initially. Eight patients required emergency airway (tracheostomy or endotracheal intubation) within 3 hours of ingestion, of which 7 patients required ventilatory support. Urinary alkalinization with mannitol and sodium bicarbonate was done for 4 non-oliguric patients. Oliguric patients presented with higher azotemia and potassium levels as compared with non-oliguric patients. Requirement of ventilation and dialysis was higher in oliguric patients. Mortality was also higher (83.3%) in oliguric patients as compared to non-oliguric (25%) patients. Seven patients underwent hemodialysis for a median of 5 sessions (3-9). Six of the 10 patients died (mortality, 60%) in this study; of these 6 patients, 2 died of sudden cardiac death preceded by arrhythmias, 1 developed sepsis after hospitalization and 3 patients had progressive deterioration of their hemodynamic status. The patients who survived had completely normal clinical and biochemical profile at 1-month follow-up. PPD and its metabolites are allergenic, mutagenic and highly toxic. Clinical presentation of PPD intoxication is usually dominated by paresis, cola-colored urine, angioedema, asphyxia and oliguria. Our findings are consistent with those of published reports. [2],[3],[4] Asphyxia and respiratory failure are secondary to the upper respiratory tract and cervical edema and warrant urgent intervention. The demographic profile of the patients in our study compares favorably with that of the patients in earlier studies. A large cohort of 374 Moroccan patients was dominated by females belonging to the younger age group consuming PPD with suicidal intent. [5] The kidneys are particularly vulnerable to the toxic effects of PPD. Hemolysis, rhabdomyolysis, methemoglobinemia and direct tubular toxicity are possible mechanisms for ARF. [6] In animal model, PPD induces rhabdomyolysis leakage of calcium ions from the smooth endoplasmic reticulum, followed by continuous contraction and irreversible structural changes in the muscles. [7] Postmortem renal biopsy performed in one of our patients showed features of acute tubular necrosis; myoglobin cast was not demonstrated. Rare complications of PPD toxicity that are reported include chronic renal failure, severe myocardial rhabdomyolysis leading to cardiogenic shock and death, severe aplastic anemia, severe contact dermatitis and optic atrophy. [8],[9],[10],[11],[12],[13] Sudden cardiac death observed in 2 patients could be related to severe myocardial rhabdomyolysis, as reported earlier. [9],[10] There is no specific antidote for PPD and treatment is supportive. PPD is emerging as a suicidal poison. Primary care physicians, intensive care physicians and nephrologists need to be aware about the clinical manifestation and management of this condition. Role of hemoperfusion, hemoadsorption and continuous therapies need evaluation. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09032t1.jpg] |
| |||||||||


{kind=link}