 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
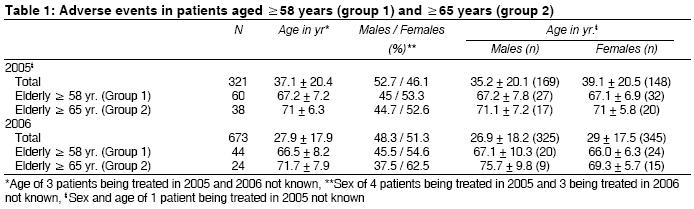
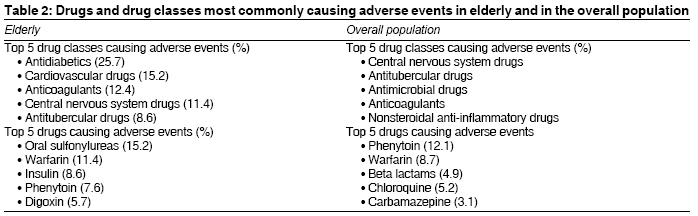
Indian Journal of Medical Sciences, Vol. 63, No. 5, May, 2009, pp. 167-173 Original Article A retrospective analysis of adverse events in the elderly in a tertiary referral center in Mumbai (Bombay), India Rupawala AbbasH, Kshirsagar NilimaA, Gogtay NithyaJ Department of Clinical Pharmacology, Seth G.S. Medical College and K.E.M. Hospital, Mumbai Code Number: ms09033 PMID: 19584486 Abstract Background : Adverse events (AEs) account for significant morbidity and mortality in elderly. Inappropriate medication usage has been regarded as an important factor contributing to AEs in them. Beers criteria are a set of standard criteria for guiding drug prescription in elderly. Keywords: Adverse events, beers criteria, elderly, inappropriate medications Introduction Although appropriate drug therapy can reduce morbidity, at times the use of a drug in a specific situation may be considered inappropriate - when the risks associated with the drug usage outweigh the benefits. Adverse events (AEs) negatively impact the quality of life and can at times be fatal. They cause clinically significant morbidity and mortality and are associated with large economic costs. [1],[2] AEs are common across age groups, though the predominant drug class causing the AE in a particular age group may vary. Several studies have shown that the incidence of AEs is higher in elderly [3],[4],[5] and is associated with several factors, one of which is polypharmacy. A study in 1997 found that 35% of ambulatory older adults experienced an AE, and 29% required health care services (physician, emergency department visit or hospitalization) for the same. [6] Polypharmacy is associated with an increase in drug interactions, noncompliance and adverse events, which in turn leads to increase in hospital admissions and thus increased expenditure on health care. [7],[8] Several studies have attributed polypharmacy in elderly to factors such as age, multiple diseases, recent hospitalization, female sex, depression and the number of physicians prescribing drugs to the elderly. [9] Another important factor accounting for higher incidence of AEs in elderly is the use of drugs that may be inappropriate for them. AEs occurring as a result of inappropriate medication (IM) usage are increasingly becoming the focus of researchers. In 1992, Lindley et al. demonstrated the relation between inappropriate drug prescribing and AEs in elderly. They found that nearly 50% of the AEs in elderly were due to drugs that were contraindicated for use in them. [10] Around the same time, Beers et al. prepared a list of drugs inappropriate for use in elderly. A panel of experts consisting of geriatricians and pharmacologists headed by Mark Beers used a two-round survey based on the modified Delphi technique and prepared the original Beers criteria in 1991. [11] The original list was only for elderly residing in nursing homes. It was later updated twice, in 1997 and 2003, to include all elderly. [12,13] Over the years, authors have demonstrated a positive correlation between inappropriate medication use as per Beers criteria and increased utilization of health care services, [14],[15],[16],[17] leading to increased health care expenditure. [14],[18] Studies on AEs and adverse drug reactions (ADRs) from India mostly assess their nature, incidence, severity, causality, preventability and economic burden. [19],[20],[21],[22] None of the reports have any special focus on AEs in elderly and their correlation with inappropriate drug prescribing. This paper is a retrospective analysis of AE data collected at Seth G.S. Medical College and K.E.M. Hospital, Mumbai (Bombay), a tertiary care hospital in western India. The data was evaluated for the number of AEs in elderly, and the Beers criteria were applied to assess appropriateness of medication prescription in them preceding the AE. Materials and Methods Definitions Study methodology Elderly was defined as those aged ≥58 years. Since our life expectancy is lesser than that in developed countries, a cutoff of 65 years would considerably decrease the size of our study population. Thus, we did not use the cutoff of ≥65 years. Results There were a total of 321 AEs reported in the year 2005; and 673 AEs, in 2006. The elderly above 58 years constituted 18.9% (60) of the total number of patients in 2005 and 6.5% (44) of the total number of patients in 2006, whereas 11.8% (38) of the patients in 2005 and 3.5% (24) in 2006 were in the ′above 65′ age group. [Table - 1] gives AEs in patients aged ≥58 years (group 1) and ≥65 years (group 2). As seen from the table, there is a difference between the two genders in the occurrence of AEs. However, on further analysis, the difference was found to be statistically insignificant. It was observed that in 2005, 7/60 (11.6%) AEs in group 1 were due to drugs considered inappropriate for use in elderly as per Beers criteria, whereas in 2006 there was no such AE reported. Of the 7 AEs in 2005, 6 were due to digoxin (4, alone; and 2, in combination) and 1 due to chlordiazepoxide. In group 2, 3/38 (7.8%) AEs in 2005 and none in 2006 were, again, due to drugs not fulfilling Beers criteria. The major drug classes causing AEs across all age groups in both 2005 and 2006 were central nervous system drugs, followed by antitubercular drugs and antimicrobial agents. In elderly above 58 years, it was observed that almost one fourth of the AEs in both the years were caused by antidiabetic drugs. The predominant drugs in that class were sulfonylureas and insulin, manifesting mainly as hypoglycemia, hypoglycemic coma and seizures. The second and third major drug classes were cardiovascular drugs (mainly antihypertensives, diuretics and digoxin) and anticoagulants (warfarin), respectively. List of drugs and drug classes most commonly causing AEs in elderly and in the overall population is given in [Table - 2]. In 2005, 25% of the AEs could be attributed to one of the three drugs, namely, insulin, digoxin and warfarin; and in 2006, 26.67%, to just insulin and warfarin as there were no cases of digoxin toxicity. Cases of digoxin toxicity mainly presented with nausea, vomiting, anorexia and ECG changes; warfarin toxicity, with bleeding episodes; and insulin, with episodes of hypoglycemia. As many as 57.7% of the AEs could be attributed to cardiovascular, antidiabetic and anticoagulant drugs. Another important class of drugs causing AEs is the antitubercular drugs, accounting for nearly 6.6% of the AEs in 2005; and 11.3%, in 2006. The findings in group 2, i.e., ′65 years and above′ age group, were similar to those in group 1. Phenytoin and warfarin were also commonly involved in AEs in the overall population. Another drug commonly causing AEs in the general population is chloroquine, which is also a very commonly used drug in India. Discussion Review of the data collected at our center showed that in 2005, approximately 12% of AEs in the age group of 58 years and above and approximately 8% in the age group of 65 years and above were due to drugs not fulfilling Beers criteria. A study by Budnitz et al.[26] found that 3.6% of the AEs leading to emergency department visits in elderly aged 65 years and above were due to drugs not fulfilling Beers criteria. Thus, a small proportion of the AEs in elderly were due to medications not fulfilling Beers criteria. Furthermore, Budnitz also showed that although the medications not fulfilling Beers criteria caused 3.6% of the AEs, nearly 10.5% of the elderly were prescribed drugs inappropriate for them. [26] Numerous studies from various countries have similarly attributed AEs in elderly to IM usage. [26],[27],[28] Researchers over the last 15 years have documented widespread IM use by elderly persons in hospitals, [28] nursing homes, [29] board and care facilities, [30] physician office practices, [31] hospital outpatient departments [32] and by homebound elderly, [33] with an estimated prevalence of potentially IM use of 12% to 40%. IM usage is ultimately a function of the number of drugs used. Thus, polypharmacy is the main risk factor for both IM usage and AEs in elderly. [34] In fact, Laroche et al. were of the opinion that polypharmacy is the main AE-facilitating factor, whereas IM usage is a subordinate factor. [35] In our study, there was no data available on drug prescriptions of elderly patients developing the reported AEs, as a result of which we are unable to produce data of the number of drugs used and IM usage by them. Due to the retrospective nature of this study, we are unable to compute prevalence of AEs in elderly. Also, the Beers criteria define elderly individuals as those aged 65 years and above. [13] However, the United Nations have not put forth any standard criterion for defining elderly. In most countries, the age at which an individual retires and is eligible to receive pension benefits is considered as the cutoff for defining elderly individuals. Thus in our study, we used a cutoff of 58 years. [36] In 2005, 6 of the 7 AEs attributed to drugs not fulfilling Beers criteria were due to digoxin. As per Beers criteria, Digoxin is considered inappropriate for use in elderly only in specific circumstances, i.e., when it is used above a dose of 0.125 mg/day except when it is used to treat atrial arrhythmias. [16] Certain drug classes like antidiabetics, oral anticoagulants and antiplatelets and narrow-therapeutic index drugs accounted for almost two thirds of the AEs in elderly; and of them, warfarin, digoxin and insulin causing a fourth of the AEs in elderly, which is, again, quite similar to the findings of Budnitz et al. Considering the extensive usage of these medications, it would be safe to assume that greater care observed while prescribing them would translate into a much greater decrease in AEs in elderly, leading to a substantial decrease in morbidity and mortality and thus a decrease in health care expenditure. Antitubercular drugs, which are used a lot more often than in western countries, are also important contributors to AEs in elderly, considering their weaker bodies and decreased organ reserve. However, this study has several limitations. Data has been collected from a tertiary referral center, where on an average, more serious patients are seen. Secondly, due to lack of data on drug prescriptions, we cannot comment on the prevalence of inappropriate drug prescription in elderly and AEs resulting from inappropriate medications. Also, data regarding number of drugs used in a person are not available. Third, according to our understanding, the number of AEs is grossly under-reported. Fourth, the data was collected from the single-page AE form of the CDSCO, which is filled in by the physicians. So the completeness of the data in terms of the indication for drug use, dosage and route was dependent on the data filled in by them. The identification and reporting of an AE is also dependent to a huge extent on information shared by the patient regarding drug usage. To conclude, adverse events are a major cause of morbidity in the elderly. Some of the commonly used medications in elderly account for a significant proportion of AEs in them. While medications considered inappropriate on the basis of Beers criteria may not be accounting for a significant proportion of the AEs, it must be realized that simply a knowledge of such medications and avoiding their usage would finally contribute to decreased AE-related health care outcomes. Prospective studies of a similar nature from India would help us quantify the extent of IM prescription and AE burden in elderly. It would also help in the establishment of criteria guiding drug prescription in elderly in a developing country like India. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09033t2.jpg] [ms09033t1.jpg] |
| |||||||||

{kind=link}
{kind=link}