 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
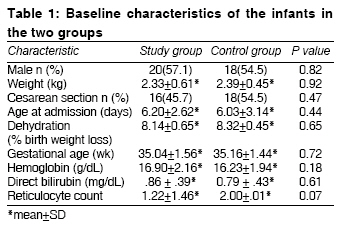
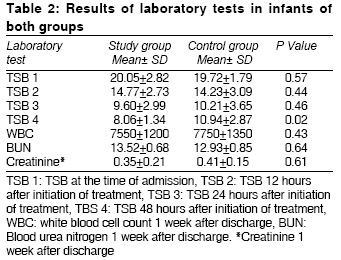
Indian Journal of Medical Sciences, Vol. 63, No. 5, May, 2009, pp. 174-179 Original Article The effect of clofibrate with phototherapy in late pre-term newborns with non-hemolytic jaundice Sakha Sedigheh HosseinPour, Gharehbaghi ManizhehMostafa, Rahbani MohammadEbrahim Department of Pediatrics, Tabriz University (Medical Sciences) Code Number: ms09034 PMID: 19584487 Abstract Background : Despite an understanding of the enzymatic pathways leading to bilirubin production and degradation, very few pharmacologic interventions are utilized and the mainstay of treatment remains phototherapy.Aims : To evaluate the efficacy of clofibrate in reducing total serum bilirubin levels in late pre-term neonates with non-hemolytic jaundice. Design and Setting : Double-blind, placebo-controlled, randomized trial; tertiary level neonatal unit. Materials and Methods : A randomized controlled study was carried out in the neonatal ward of Children's Hospital, Tabriz, Iran, over a 1-year period. Sixty-eight healthy late pre-term infants readmitted with non-hemolytic hyperbilirubinemia were randomized to receive phototherapy and clofibrate (n= 35) or phototherapy and placebo (n= 33). Statistical Analysis Used : Chi-square test and independent sample 't' test. Results : There were no significant differences in the weight, gender, modes of delivery and age of neonates between the two groups. Similarly the mean total serum bilirubin (TSB) level at the time of admission was not significantly different between the two groups [mean± SD: 19.72 ± 1.79 (95% confidence interval: 19.12-20.54 mg/dL) vs. 20.05 ± 2.82 (95% confidence interval, 19.54-22.04 mg/dL), P= 0.57]. The mean TSB 48 hours after phototherapy [mean± SD: 8.06± 1.34 (95% confidence interval: 7.94-10.18 mg/dL) vs.10.94 ± 2.87 (95% confidence interval: 9.92-12.16 mg/dL), P= 0.02] and the mean duration of phototherapy [mean± SD: 64.32 ± 12.48 (95% confidence interval: 60-81.6 hours) vs. 87.84 ± 29.76 (95% confidence interval: 79.2-108 hours), P< 0.001] were significantly lower in the clofibrate-treated group. Conclusions : Clofibrate is an effective adjunctive drug in neonatal hyperbilirubinemia, which results in decreased TSB level and reduced duration of phototherapy in late pre-term newborns. Keywords: Clofibrate, late pre-term neonate, non-hemolytic jaundice, phototherapy Introduction Most newborns experience benign hyperbilirubinemia. Severe elevation of serum bilirubin levels can result in brain damage, known as kernicterus. [1],[2],[3],[4],[5] It is important to promptly initiate appropriate therapy. The intensity and invasiveness of therapy is determined by many factors such as gestational age, relative health of the neonate, the current level of total bilirubin and the etiology of jaundice. In the neonates, hyperbilirubinemia is usually due to a combination of an increased bilirubin load and decreased bilirubin elimination. [1],[2],[3],[4],[5] Phototherapy and exchange transfusion are two main interventions that are used to decrease total serum bilirubin (TSB). [2],[3] Pharmacologic agents used in the management of hyperbilirubinemia can accelerate bilirubin clearance via the normal metabolic pathways, inhibit the enterohepatic circulation of bilirubin or interfere with bilirubin formation by either blocking the degradation of heme or inhibiting hemolysis. [2],[3],[6] Clofibrate as a hypolipidemic drug is a glucuronosyltransferase inducer which accelerates bilirubin elimination. [7],[8] Hyperbilirubinemia is a common problem in Iranian newborns and constitutes approximately one third of admissions to our neonatal ward. The efficacy of clofibrate has been shown in term neonates in several studies. [9],[10],[11],[12] Little is known about the usefulness of this drug in pre-term infants. We hypothesized that near-term infants are not very different from term neonates. So we conducted this study to assess the efficacy and safety of clofibrate in the treatment of non-hemolytic jaundice in late pre-term infants. Materials and Methods This study was a prospective randomized clinical trial conducted in the period from January to December 2008 in the neonatal ward of Tabriz Children Hospital, which is a major teaching and referral center in northwest Iran. Ethical committee of the institute approved the study protocol. Our hospital does not have nursery, and neonates that need readmission after discharge from birth hospitalization would be referred to this hospital. Criteria for enrollment in this study included healthy late pre-term newborns (gestational age, 34-37 weeks) with non-hemolytic jaundice and neonates that did not need urgent exchange transfusion. It is routine to use 2004 AAP hyperbilirubinemia guidelines, [1] for management of admitted newborn infants in our neonatology department. Neonates with major congenital anomalies; hemolytic disorders; glucose-6-phosphate dehydrogenase deficiency (G6PD) that was diagnosed by qualitative, visual, colorimetric test; sepsis or significant accompanying illness requiring NICU admission were excluded. Healthy late pre-term infants admitted for non-hemolytic jaundice were eligible for the trial. Sixty-eight neonates were enrolled in this study. They were randomized into study and control groups by a random-number table sequence after informed parental consents were obtained. The allocation notes were kept in opaque sequentially numbered sealed envelops. Study group received phototherapy and clofibrate (n= 35), and control group received phototherapy and placebo (n= 33). Based on the numerical order of sealed envelopes clofibrate or placebo was administered to patients by a nurse who was not involved in the care of the infant. A single dose of clofibrate 100 mg/kg was administered orally to infants in the study group within 12 hours of admission. Phototherapy was started immediately on admission for all studied patients until total serum bilirubin decreased to a safe level depending on the infant′s gestation and postnatal age. Each phototherapy unit contained 8 special blue fluorescent tubes labeled TL 52/20w (Philips, Eindhoven, the Netherlands) adjusted at a 20-cm distance above the infant. Lamps of phototherapy units were changed regularly after 1500 hours of usage. Total and direct serum bilirubin levels were measured 12, 24, 48 hours after admission and then daily until phototherapy was discontinued. TSB measurement was performed on the basis of spectrophotometric principles by using Bilimeter 3, Pfaff Medical GmbH, Germany; and direct bilirubin measurement, by using Autoanalyser Random Access (Selectra E, Vital Scientific, Netherlands), respectively. The equipments were standardized periodically. Laboratory tests, including complete blood count, total and direct serum bilirubin, reticulocyte count; and direct Coombs agglutination test, maternal and neonatal blood group, glucose-6-phosphate dehydrogenase determination and peripheral blood smear were performed for all jaundiced infants in both groups. Our criterion for discharge was TSB less than 50% of exchange level, which was ordered by a physician who did not know the infant′s group allocation. Duration of phototherapy was recorded by a nurse who was not involved in drug administration. All infants were examined 48 hours and 1 week after discharge, with a careful physical examination for side effects of treatment, including vomiting, loose stools; and laboratory tests including complete blood count, total serum bilirubin, blood urea nitrogen (BUN) and creatinine were carried out for detection of leucopenia, rebound hyperbilirubinemia and renal failure 1 week after discharge. All data were analyzed using statistical package of social sciences (SPSS) software for windows version 14. Statistical analysis of data was performed by chi-square and independent sample t test, and P values less than .05 were considered significant. Results During the study period, the main cause of admission in 144 (32%) neonates of the 446 admitted neonates was hyperbilirubinemia. Seventy neonates fulfilled inclusion criteria. Two patients were excluded from the study because of subsequent positive blood culture and refusal by parents for blood sampling. Remaining 68 newborn infants were assigned randomly to the two groups. Of the 68 neonates enrolled in this study, 33 patients in the control group received phototherapy and placebo, while 35 neonates in the study group received phototherapy and clofibrate. There was no significant difference in gender, weight, age at admission and cesarean section rate between the two groups [Table - 1]. Sixty-five percent of neonates were first offspring. Ninety-seven percent (66 newborns) of the studied newborns were exclusively breast-fed. Mean total serum bilirubin levels at the time of admission were as follows (mean± SD): 20.05 ± 2.82 mg/dL (95% confidence interval: 19.54-22.04 mg/dL) in the study group and 19.72 ± 1.79 mg/dL (95%confidence interval: 19.12-20.54 mg/dL) in the control group (P= 0.57). Mean duration of phototherapy was significantly shorter in the study group in comparison with control group [mean ± SD: 64.32 ± 12.48 hours (95% confidence interval: 60-81.6 hours) vs. 87.84 ± 29.76 hours (95% confidence interval: 79.2-108 hours), P< 0.001]. The results of laboratory tests of patients in the two groups are shown in [Table - 2]. None of the patients in the present study required exchange transfusion. None of the babies receiving clofibrate developed vomiting or diarrhea. We noted only one case of rebound hyperbilirubinemia, which was from the control group, during the follow-up of neonates. White blood cell count, BUN and creatinine levels were normal 1 week after discharge [Table - 2]. Discussion Despite an understanding of the enzymatic pathways leading to bilirubin production and degradation, very few pharmacologic interventions are utilized and the mainstay of treatment remains phototherapy. In our study, the duration of phototherapy and hospitalization was shorter in late pre-term infants that were treated with clofibrate in addition to phototherapy in comparison with those treated with placebo in addition to phototherapy. No important side effect was determined during the short-term follow-up of patients. Clofibrate has been used for many years in adults. It is an activator of peroxisome proliferator-activated receptors (PPARs), which decrease serum cholesterol and triglyceride levels. [7] Liver fatty acid-binding protein expression is known to be regulated by PPAR agonists, such as clofibrate. In the study by Wang, the up-regulation of liver fatty acid-binding protein was associated with a significant decrease in serum bilirubin and alanine aminotransferase by reduction of hepatic oxidative stress and improvement of hepatic function in bile duct-ligated rats. [8] The results of our study are comparable with those of reported trials in term infants [9],[10],[11],[12] and a few studies in pre-term infants. [13],[14] One study showed the usefulness of clofibrate in neonates with G6PD deficiency. [15] In a double-blind controlled study of infants without ABO incompatibility, 47 infants treated with a single dose of clofibrate demonstrated significantly lower bilirubin levels after 16 hours of treatment compared to 46 controls given corn oil alone. [9] An interval of 24-48 hours for achieving bilirubin reduction was observed in studies on efficacy of clofibrate in the treatment of hyperbilirubinemia in premature neonates. [13],[14] In our study, serum bilirubin was found significantly decreased in the clofibrate group after 48 hours. A common side effect of clofibrate is nausea. Other GI disturbances, including vomiting and loose stools, have been reported. Although complications such as muscle cramping, fatigue, pruritus, alopecia, leukopenia, renal failure and peripheral neuropathy have been described, yet their occurrence is very rare with a single dose of this drug. [7],[11],[16] We did not find gastrointestinal and renal side effects on administration of clofibrate in the studied neonates during hospitalization and until 1 week after discharge. The limitation of this study was the small number of patients studied and a short term of their follow-up. Because of non-availability of new pharmacologic medications such as metalloporphyrins for management of hyperbilirubinemia in developing countries, addition of clofibrate to phototherapy would be financially beneficial as it would reduce costs of treatment and duration of hospitalization. The long-term safety of clofibrate is debated, and more studies with larger number of patients and longer period follow-up are needed before recommending widespread use of this drug as adjunctive therapy for neonatal hyperbilirubinemia. Hence there is need for systematic review of the efficacy of clofibrate in neonatal hyperbilirubinemia, as well as its side effects. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09034t2.jpg] [ms09034t1.jpg] |
| |||||||||

{kind=link}
{kind=link}