 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
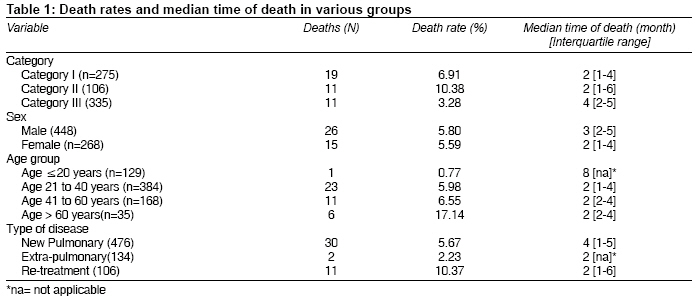
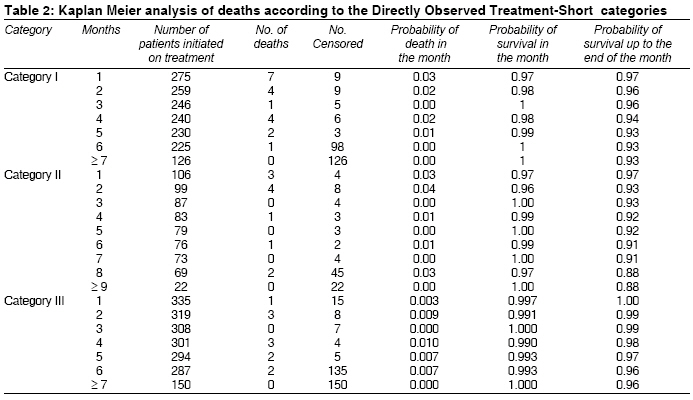
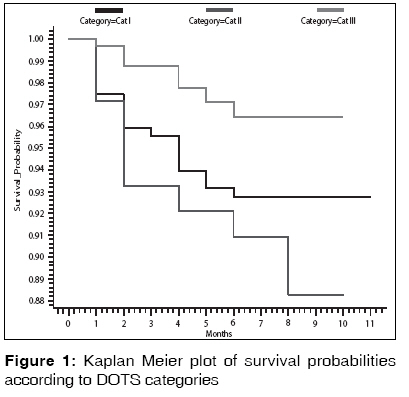
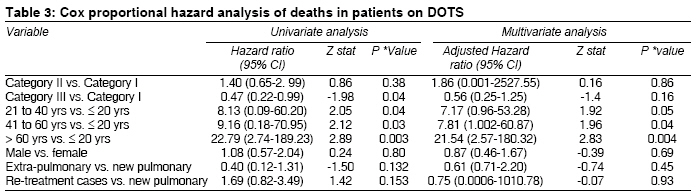
Indian Journal of Medical Sciences, Vol. 63, No. 5, May, 2009, pp. 180-186 Original Article Survival analysis and risk factors for death in tuberculosis patients on directly observed treatment-short course Pardeshi Geeta Department of PSM, Dr. Shankarrao Chavan Government Medical College, Nanded Code Number: ms09035 PMID: 19584488 Abstract Background : Tuberculosis is a disease with a high case fatality of 4.65%. Keywords: Tuberculosis, death, directly observed treatment-short course, revised National Tuberculosis Control Programme Introduction In India, which accounts for 30% of the global burden of tuberculosis (TB), the Directly Observed Treatment-Short course (DOTS) program has undergone massive expansion as treatment success rate has doubled and death rate has fallen. [1] With an approximate 18 additional lives saved per 100 patients treated under the Revised National Tuberculosis Control Programme (RNTCP), the program has substantially reduced deaths amongst patients treated and saved an estimated over 1.4 million additional lives since its inception. [2] Reducing the morbidity and mortality due to tuberculosis is one of the major goals of RNTCP. The death rate amongst the new smear-positive patients has been reduced to less than 5%. [3] Yet amongst the infectious diseases, TB continues to be a disease with a high case fatality, viz. 4.27%. [4] The aim of the study is to describe the survival probability with respect to the DOTS category, type of disease, age and sex of the patient. Materials and Methods RNTCP was initiated in Yavatmal district in August 2002. By the end of the year 2004, the entire district was covered under DOTS. The district has an annualized total case detection rate of 134 per 100,000 of the population and a cure rate of 85%. Kaplan Meier analysis was used to study survival pattern, in which the probability of survival in each month after treatment initiation was calculated followed by calculation of cumulative probability of survival by the end of that particular month. The group variables studied included category of DOTS, age and sex of the patients. The end point studied was death. The time of death was ascertained by calculating the difference between the date of initiation and date of outcome. The difference was divided by 30 to determine the month in which the event occurred. For example, if the difference was 100 days, it was divided by 30 to get the figure 3.33, the inference being that the outcome occurred in the fourth month. The events which were censored were default, treatment completion, cure, failure and transfer. The Kaplan Meier curve was drawn to arrive at the overall estimate of patients surviving at the end of each month. The difference in the survival patterns over time between different groups was studied using the log rank test. The Cox proportional hazards model was used for multivariate analysis to identify the risk factors for death. Results A total of 716 patients were registered at the DTC during the year 2004. Of these, 275 belonged to category I, 106 to category II and 335 to category III. Amongst the 235 new smear-positive cases, the treatment success rate was 86.06%, default rate was 6.3%, death rate was 4.7% and failure rate was 2.94%. The median time of death was 2 months for majority of the groups. The death rate in category I was 6.8%; in category II, 10.38%; and in category III, 3.28%. The death rate was more than 10% in category II (re-treatment group) and in the age group ′more than 60 years′ [Table - 1]. Out of the 19 deaths in category I, 11 occurred in smear-positive cases, 6 in smear-negative cases and 2 in extra-pulmonary tuberculosis cases. All the 11 deaths in category III occurred in smear-negative tuberculosis cases. The Kaplan Meier analysis of the data [Table - 2] showed that in category I the probability of survival at the end of the intensive phase was 96%. The probability of survival at the end of 6 months and till the time all patients were censored remained at 96%. In category II the probability of survival at the end of the intensive phase was 93%; and by the end of the 10 th month, by which time all patients were censored, it was 88%. In category III, probability of survival was 99% at the end of the intensive phase and 96% by the time all patients were censored. Of the total deaths, 57.89% (11/19) in category I, 63.63% (7/11) in category II and 36.36% (4/11) in category III occurred at the end of the intensive phase. These findings are represented in the Kaplan Meier plot in [Figure - 1], which describes the survival curves of the three DOTS categories. There was a significant difference in the survival curves for the three DOTS categories (log rank statistic= 7.26, d.f.= 2, P= 0.02). A high proportion of deaths in category II and I occurred in the intensive phase. A similar type of analysis was done for sex, age and type of disease. There was no significant difference in the survival curves between the male and female patients (log rank statistic= 0.05, d.f.= 1, P= 0.80). Survival rates at the end of intensive phase in males was 97%; and in females, 96%. The cumulative survival rate at the end of the treatment period was 92% in males and 93% in females. The difference in survival curves amongst the four age groups studied was statistically significant (log rank statistic= 14.08, d.f.= 3, P= 0.002). Survival rate at the end of the intensive phase was 100% in the patients in the age group ′up to 20 years,′ while it was 96%, 97% and 91% in the patients in the age groups ′21 to 40 years,′ ′41 to 60 years′ and ′more than 60 years,′ respectively. The cumulative survival rates were 95%, 94%, 93% and 86% in the four age groups, respectively. There was no significant difference in the survival curves of the different types of the disease (log rank statistic= 5.63, d.f.= 2, P= 0.05). The survival rates at the end of the intensive phase were 97%, 98% and 93% in the new pulmonary, extra-pulmonary and re-treatment groups, respectively. The cumulative survival rates at the end of the treatment period were 94%, 98% and 88% in these three groups, respectively. On multivariate analysis [Table - 3], age was identified as a risk factor for mortality. The patients aged 41 to 60 years were 7.8 times more at risk of death as compared to patients aged less than 20 years, and patients aged above 60 years were 21.54 times more at risk of death as compared to the patients aged less than 20 years. Discussion The survival rates in this study were found to be 93%, 88% and 96% in categories I, II and III, respectively. The survival rates reported in another study were 96%, 94% and 97% in categories I, II and III, respectively. [5] Age has been identified as an important risk factor for death in tuberculosis patients. Higher death rates have been noted in the elderly patients. [6],[7],[8],[9] Apart from the increased physiological risk of death, the vague symptoms in the elderly, diagnostic problems and concomitant illness could be some of the contributing factors for the increased death rate in the elderly. [7],[10] Concomitant diseases like cardiovascular diseases, COPD, diabetes mellitus and malignancy have been found to be frequently present in the older patients with tuberculosis. [10],[11] Screening the patients for these diseases and managing them appropriately will be important. In this study, out of the total 41 deaths in patients of tuberculosis, 11 deaths occurred in smear-positive patients; and remaining 30 deaths, in other groups of patients. In another study conducted in the state of Delhi, mortality due to tuberculosis was considerably reduced among new sputum-positive cases with the implementation of RNTCP. However, mortality among smear-negative and new extra-pulmonary and re-treatment cases did not show any significant decline. [12] This is presumably because the emphasis during phase I of RNTCP had been mainly on new smear-positive cases. As these goals are achieved, it is necessary to look at the treatment outcomes in other groups of patients and study the underlying causes of death and effect of HIV co-infection in these groups. In a study on extra-pulmonary tuberculosis it was noted that 47% patients had co-morbidities, and death was related to tuberculosis in 48% of the patients. [13] In a study on extra-pulmonary tuberculosis, HIV co-infection was associated with high mortality rates. [14] In another study HIV infection was found to significantly increase the risk of death in smear- negative tuberculosis. [15] As secondary data was utilized for our study, a number of other factors such as addictions, co-morbidities, HIV status could not be studied. A lower survival rate at the end of the intensive phase was noted in re-treatment cases (category II) and in patients with age above 60 years. More than half of the total deaths in categories II and I occur in the intensive phase of treatment. Category II includes patients receiving re-treatment after default, failure or relapse. Incomplete treatment is a known risk factor for mortality in tuberculosis patients. [16],[17] It would be interesting to study whether old age and incomplete treatment, which are known risk factors for mortality in tuberculosis, also result in early deaths during the course of treatment. It is important to study the characteristics of patients who die within two months of treatment and those who die later in the continuation phase. This will help in planning effective interventions to prevent deaths due to tuberculosis. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09035t3.jpg] [ms09035t1.jpg] [ms09035t2.jpg] [ms09035f1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}