
|
Indian Journal of Medical Sciences
Medknow Publications on behalf of Indian Journal of Medical Sciences Trust
ISSN: 0019-5359 EISSN: 1998-3654
Vol. 63, Num. 5, 2009, pp. 187-194
|
Indian Journal of Medical Sciences, Vol. 63, No. 5, May, 2009, pp. 187-194
Original Article
Vitamin D receptor (FokI, BsmI and TaqI) gene polymorphisms and type 2 diabetes mellitus : A North Indian study
Bid HemantKumar, Konwar Rituraj, Aggarwal CG, Gautam Sunaina, Saxena Madhukar, Nayak VLakshma, Banerjee Monisha
Department of Zoology, University of Lucknow
Correspondence Address:Molecular and Human Genetics Laboratory, Department of Zoology, University of Lucknow, Lucknow - 226 007
banerjee_monisha30@rediffmail.com
Code Number: ms09036
PMID: 19584489
DOI: 10.4103/0019-5359.53164
Abstract
Background : The vitamin D receptor (VDR) gene is a candidate gene for susceptibility to several diseases. Studies on association between VDR polymorphisms and risk of type 2 diabetes (T2DM) in different ethnic populations are yet inconclusive.
Aims : This study was conducted to evaluate association between VDR polymorphisms and genetic susceptibility to T2DM in the north Indian population.
Settings and Design : One hundred clinically diagnosed T2DM patients and 160 healthy controls from the north Indian population were recruited for genetic association study.
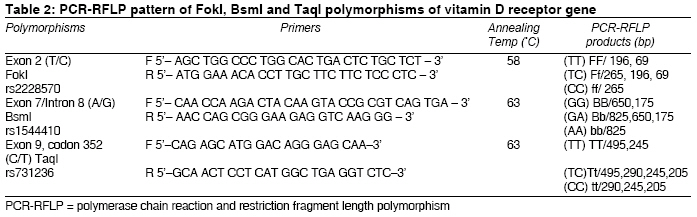
Materials and Methods : Genomic DNA was extracted from blood and genotyped for the single nucleotide polymorphism SNPs of FokI (T/C) [rs2228570], BsmI (A/G) [rs1544410] and TaqI (C/T) [rs731236] by polymerase chain reaction and restriction fragment length polymorphism (PCR-RFLP) analysis.
Statistical Analysis Used : Genotype distribution and allelic frequencies were compared between patients and controls. Mean values and odds ratios (ORs) with 95% confidence interval (CI) were calculated using SPSS software (version 15.0).
Results : The genotype distribution, allele and haplotype frequencies of VDR polymorphism did not differ significantly between patients and controls. Mean age and waist-hip ratio of patients were found to be associated with VDR polymorphism. Combination studies showed FFBbtt increased the risk of T2DM in north Indians.
Conclusions : Our data suggest that VDR gene polymorphism in combination of genotypes is associated with the risk of T2DM and thus requires further studies as a probable genetic risk marker for T2DM.
Keywords: Diabetes, genetic polymorphisms, restriction fragment length polymorphisms, vitamin D receptor
Introduction
Environmental and genetic factors play important roles in the mechanisms involved in the development of T2DM. Studies on genes inducing susceptibility to T2DM have been carried out by various groups in different populations. [1],[2],[3],[4],[5],[6],[7],[8],[9] An association study of candidate genes, viz., fatty acid binding protein 2 (FABP2), uncoupling protein type 1 gene (UCP1), protein phosphatase type 1 (PP1G), b3 adrenergic receptor (b3AR), VDR, was carried out on T2DM patients in a migrant Indian population as well by Boullus-Sanchis et al.[10]
Genome-wide association studies have led to the identification of several single nucleotide polymorphisms in genes such as CDKAL1, CDKN2B, HHEX/IDE, IGF2BP2, KCNJ11, SLC30A8, TCF2, TCF7L2 and WFS1.[11] Several genes were studied but only a handful showed confirmed association, such as resistin, alpha-endosulfine, calpain10, peroxisome proliferators-activated receptor-gamma 2 (PPARg-2), abundant transcript 1 gene (apM1), TCF7L2, insulin-like growth factor-binding protein 5 (IGFBP5), to name a few. [9],[12],[13],[14],[15],[16],[17],[18],[19]
Earlier studies on genetic polymorphisms in T2DM candidate genes were carried out among south Indians, in addition to those in the VDR gene. [20],[21],[22] VDR is a member of the steroid/thyroid hormone receptor family. [23] It is known that vitamin D and especially its activated metabolite 1,25-dihydroxyvitamin D3 (1,25D3) are involved in controlling the normal functions of the endocrine pancreas, particularly insulin secretion; and the action of vitamin D is mediated through binding to its nuclear receptor (VDR). [24] Vitamin D and its receptor complex play the role of a transcription factor in regulating the b-cell insulin secretion. Vitamin-D deficiency has been shown to impair insulin synthesis and secretion in humans and in animal models of diabetes, which suggests it has a role in the development of type 2 diabetes. [25] There is evidence to suggest that altered vitamin D and calcium homeostasis also play a role in the development of T2DM; and recently, Knekt et al. reported that high vitamin D status provides protection against type 2 diabetes. [26],[27]
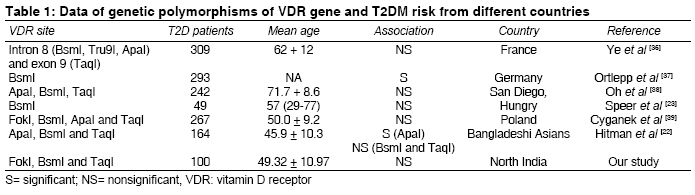
In recent years, several polymorphisms, such as BsmI and FokI, have been described in the VDR genes that are able to alter the activity of VDR protein. [28] Some of the other polymorphisms in the VDR gene identified by allelic variation in restriction enzyme sites are Tru9I, TaqI, EcoRV and ApaI. [29] All these are located between exons 8 and 9 except that FokI is in exon 2. FokI polymorphism has been shown to have functional role in trascriptional activation of VDR gene. [30] However, the genetic background of the disease still remains unclear. Although these findings suggest that the VDR gene is a novel candidate gene contributing to susceptibility to T2DM [Table - 1], there are no data on association of VDR gene polymorphism with T2DM in the north Indian population. In our present work, we studied the FokI, BsmI and TaqI restriction enzyme polymorphisms of the VDR gene in patients with T2DM in a north Indian population.
Materials and Methods
Subject selection
The current study was carried out after obtaining prior approval from the institutional ethical committee of Chhatrapati Sahuji Maharaj Medical University (CSMMU), Lucknow, India. Patients (n= 100) with type 2 diabetes attending the Diabetes Clinic in the outpatient department of CSMMU, Lucknow, were enrolled for the present study. Screening and management of patients were done as per American Diabetes Association guidelines. [31] A questionnaire was used to record clinical history of patients, family history of diabetes and associated complications such as hypertension, etc.
A total of 160 age- and sex-matched normal healthy controls were enrolled for the study from among the healthy staff members of the institute and the university. They were screened with standard oral glucose tolerance test. Subjects having a history of coronary artery disease and other complications were not included in the control group.
DNA extraction and genotyping
After obtaining an informed consent, 5 mL of blood sample was collected in anticoagulant and plain vials from patients of both the groups. DNA was extracted from the blood samples by using QIAamp DNA mini kit (QIAGEN, Germany). Amplification was performed in a 20-µL reaction mixture containing genomic DNA (100-150 ng), 200 nM dNTPs (MBI-Fermentas, USA), 2-8 pmol of each primer and 0·5U of Taq DNA polymerase (MBI-Fermentas, USA) per tube in a gradient thermal Master cycler (Eppendorf, USA). Amplification reactions were set up separately for FokI, BsmI and TaqI polymorphic sites of VDR gene using primers given by Harris et al. and Morrison et al. [Table - 2]. [32],[33] PCR-RFLP was used to identify the genotypic pattern of VDR family.
In order to improve the genotyping quality and validation, 20% of samples were re-genotyped by other laboratory personnel, and results were found to be reproducible with no discrepancy in genotyping. Genotyping of 10% randomly selected samples was confirmed by DNA sequencing.
Statistical analysis
Allele frequencies, genotype frequencies and carriage rates of the alleles in all the groups were compared by using Fisher′s exact test. The Hardy-Weinberg equilibrium at individual loci was assessed by c2 statistics using SPSS software (version 15.0), and clinical association was calculated by paired t test. All P values were two sided, and differences were considered statistically significant for P< 0.05. Odds ratio (OR) at 95% confidence interval (CI) was determined to describe the strength of association by logistic regression model. Allele frequency was calculated as the number of occurrences of the test allele in the population divided by the total number of alleles. Carriage rate was calculated as the number of individuals carrying at least one copy of test allele divided by the total number of individuals.
Results
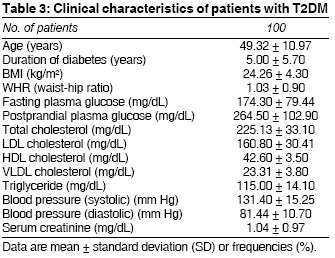
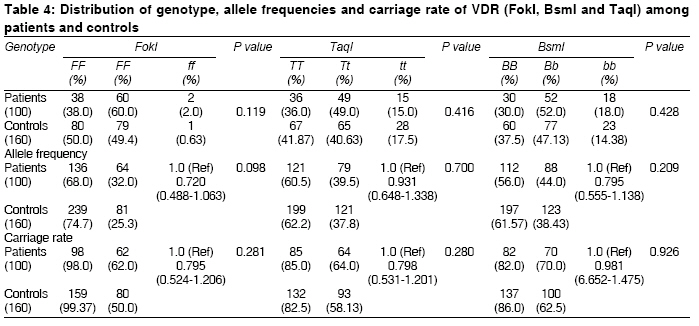
Clinical characteristics of the patients are summarized in [Table - 3]. The average age of the patient population was 49.32± 10.97 years, with mean BMI of 24.26± 4.30 kg/m 2 . The allele and genotype frequency distribution and carriage rate of VDR (FokI, BsmI and TaqI) genes among patients and controls were as shown in [Table - 4]. We did not observe any significant difference in VDR (FokI, BsmI and TaqI) genotypes between patient and control groups (P= 0.119, 0.428 and 0.416, respectively). Genotypes of each VDR marker were in Hardy-Weinberg equilibrium in each group separately and in the total of 100 T2DM patients.
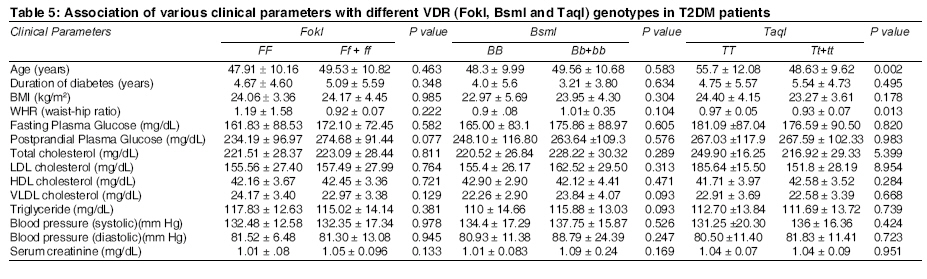
In addition, we also compared the VDR (FokI, BsmI and TaqI) genotypes with different clinical parameters of T2DM but could not obtain association of any of the parameters except age (P= 0.002) and waist-hip ratio (P= 0.013) with VDR TaqI genotypes [Table - 5].
Combining FokI, BsmI and TaqI genotypes resulted in 23 possible combinations. When each combination genotype was tested using χ2 against all other combination genotypes, there was a trend of increased risk of diabetes in the genotypes FfBbTt {P= 0.136, OR= 4.00 (0.64-24.69)} and FFBbtt {P= 0.334, OR= 2.50 (0.38-16.04)}.
Discussion
Allelic differences in the VDR gene may contribute to the genetic predisposition to certain diseases. As vitamin D modulates insulin secretion, it is feasible that genetic variants of the VDR gene may contribute to the development of T2DM. Since patients with T2DM exhibit subtle alterations in glucose metabolism long before onset of the disease, genetic factors contributing to its pathogenesis or development could be detected early in the disease process. [34]
Our study revealed significant association of age (P= 0.002) and waist-hip ratio (P= 0.013) with TaqI genotypes of VDR gene polymorphism. This may indicate the association of VDR polymorphism with both modifiable and nonmodifiable risk factors of diabetes.
Our investigation showed the nonsignificant association between VDR (FokI, BsmI and TaqI) genotypes and diabetes risk in the north Indian population. Previous investigations of VDR polymorphisms and diabetes risk by other groups have produced inconsistent results [Table - 1].
Two studies have reported link between VDR polymorphism and diabetes risk - one in Caucasian subjects, for BsmI site; and the other in Bangladeshi Asians, for ApaI site.[23] However, our study, like the one in Polish population, showed no association between VDR FokI, ApaI, BsmI and TaqI polymorphism and diabetes risk. [35]
Further studies involving genetic linkage assessment are needed to evaluate the direct effect of these polymorphisms on T2DM; also, the studies should be carried out on a large cohort of population. The major limitation of the current study is its moderately low sample size. While polymorphisms of the VDR gene might play a role in the pathogenesis of T2DM, the non-association of FokI, BsmI and TaqI need to be interpreted considering this limitation. Finally, our data affirms the association of VDR polymorphism in combination of genotypes with risk of T2DM in the north Indian population.
Acknowledgments The authors would like to thank the Department of Biotechnology, Govt. of India, for funding the work.[39]
References
| 1. | Gragnoli C, Milord E, Habener JF. Linkage study of the glucagon receptor gene with type 2 diabetes mellitus in Italians. Metabolism 2005;54:786-7. Back to cited text no. 1 |
| 2. | Almawi WY, Wakim-Ghorayeb SF, Arekat MR, Najm P, Keleshian SH, Al-Sayed N, et al. Association of selective HLA class II susceptibility-conferring and protective haplotypes with type 2 diabetes in patients from Bahrain and Lebanon. Clin Vaccine Immunol 2006;13:1296-8. Back to cited text no. 2 |
| 3. | Grarup N, Rose CS, Andersson EA, Andersen G, Nielsen AL, Albrechtsen A, et al. Studies of association of variants near the HHEX, CDKN2A/B, and IGF2BP2 genes with type 2 diabetes and impaired insulin release in 10,705 Danish subjects: Validation and extension of genome-wide association studies. Diabetes 2007;56:3105-11. Back to cited text no. 3 |
| 4. | Leak TS, Mychaleckyj JC, Smith SG, Keene KL, Gordon CJ, Hicks PJ, et al. Evaluation of a SNP map of 6q24-27 confirms diabetic nephropathy loci and identifies novel associations in type 2 diabetes patients with nephropathy from an African-American population. Hum Genet 2008;124:63-71. Back to cited text no. 4 |
| 5. | Herder C, Rathmann W, Strassburger K, Finner H, Grallert H, Huth C, et al. Variants of the PPARG, IGF2BP2, CDKAL1, HHEX, and TCF7L2 genes confer risk of type 2 diabetes independently of BMI in the German KORA studies. Horm Metab Res 2008;40:722-6. Back to cited text no. 5 |
| 6. | Wu Y, Li H, Loos RJ, Yu Z, Ye X, Chen L, et al. Common variants in CDKAL1, CDKN2A/B, IGF2BP2, SLC30A8, and HHEX/IDE genes are associated with type 2 diabetes and impaired fasting glucose in a Chinese Han population. Diabetes 2008;57:2834-42. Back to cited text no. 6 |
| 7. | Lee YH, Kang ES, Kim SH, Han SJ, Kim CH, Kim HJ, et al. Association between polymorphisms in SLC30A8, HHEX, CDKN2A/B, IGF2BP2, FTO, WFS1, CDKAL1, KCNQ1 and type 2 diabetes in the Korean population. J Hum Genet 2008;53:991-8. Back to cited text no. 7 |
| 8. | Ng MC, Park KS, Oh B, Tam CH, Cho YM, Shin HD, et al. Implication of genetic variants near TCF7L2, SLC30A8, HHEX, CDKAL1, CDKN2A/B, IGF2BP2, and FTO in type 2 diabetes and obesity in 6,719 Asians. Diabetes 2008;57:2226-33. Back to cited text no. 8 |
| 9. | Tong Y, Lin Y, Zhang Y, Yang J, Zhang Y, Liu H, et al. Association between TCF7L2 gene polymorphisms and susceptibility to type 2 diabetes mellitus: A large Human Genome Epidemiology (HuGE) review and meta-analysis. BMC Med Genet 2009;10:15. Back to cited text no. 9 |
| 10. | Boullu-Sanchis S, Lepretre F, Hedelin G, Donnet JP, Schaffer P, Froguel P, et al. Type 2 diabetes mellitus: Association study of five candidate genes in an Indian populaton of Guadeloupe, genetic contribution of FABP2 polymorphism. Diabetes Metab (Paris) 1999;25:150-6. Back to cited text no. 10 |
| 11. | Ruchat SM, Elks CE, Loos RJ, Vohl MC, Weisnagel SJ, Rankinen T, et al. Association between insulin secretion, insulin sensitivity and type 2 diabetes susceptibility variants identified in genome-wide association studies. Acta Diabetol 2008;Dec 10 [Epub ahead of print]. Back to cited text no. 11 |
| 12. | Groop L, Lyssenko V. Genes and type 2 diabetes mellitus. Curr Diab Rep 2008;8:192-7. Back to cited text no. 12 |
| 13. | Osawa H, Yamada K, Onuma H, Murakami A, Ochi M, Kawata H, et al. The G/G genotype of a resistin single-nucleotide polymorphism at -420 increases type 2 diabetes mellitus susceptibility by inducing promoter activity through specific binding of Sp1/3. Am J Hum Genet 2004;75:678-86. Back to cited text no. 13 |
| 14. | Wang H, Craig RL, Schay J, Chu W, Das SK, Zhang Z, et al. Alpha-endosulfine, a positional and functional candidate gene for type 2 diabetes: molecular screening, association studies, and role in reduced insulin secretion. Mol Genet Metab 2004;81:9-15. Back to cited text no. 14 |
| 15. | Elbein SC, Chu W, Ren Q, Hemphill C, Schay J, Cox NJ, et al. Role of calpain-10 gene variants in familial type 2 diabetes in Caucasians. J Clin Endocrinol Metab 2002;87:650-4. Back to cited text no. 15 |
| 16. | Kang ES, Kim HJ, Nam M, Nam CM, Ahn CW, Cha BS, et al. A novel 111/121 diplotype in the Calpain-10 gene is associated with type 2 diabetes. J Hum Genet 2006;51:629-33. Back to cited text no. 16 |
| 17. | Mohamed MB, Mtiraoui N, Ezzidi I, Chaieb M, Mahjoub T, Almawi WY. Association of the peroxisome proliferator-activated receptor-gamma2 Pro12Ala but not the C1431T gene variants with lower body mass index in Type 2 diabetes. J Endocrinol Invest 2007;30:937-43. Back to cited text no. 17 |
| 18. | Li S, Li L, Li K, Qi X, Hoekema D, Liu H, et al. Association of adipose most abundant transcript 1 gene (apM1) with type 2 diabetes mellitus in a Chinese population: A meta-analysis of case-control studies. Clin Endocrinol (Oxf) 2008;68:885-9. Back to cited text no. 18 |
| 19. | Kallio P, Tolppanen AM, Kolehmainen M, Poutanen K, Lindstrφm J, Tuomilehto J, et al. Association of sequence variations in the gene encoding insulin-like growth factor binding protein 5 with adiponectin. Int J Obes (Lond) 2009;33:80-8. Back to cited text no. 19 |
| 20. | Lepretre F, Vionnet N, Budhan S, Dina C, Powell KL, Gιnin E, et al. Genetic Studies of polymorphisms in ten non-insulin dependent diabetes mellitus candidate genes in Tamil Indians from Pondichery. Diabetes Metab 1998;24:244-50. Back to cited text no. 20 |
| 21. | McDermott MF, Ramachandran A, Ogunkolade BW, Aganna E, Curtis D, Boucher BJ, et al. Allelic variation on the VDR influence susceptibility to insulin dependent diabetes mellitus in Indian Asians. Diabetolgia 1997;40:971-5. Back to cited text no. 21 |
| 22. | Hitman GA, Mannan N, McDermott MF, Aganna E, Ogunkolade BW, Hales CN, et al. VDR gene polymorphism influence insulin secretion in Bangladeshi Asian. Diabetes 1998;47:688-91. Back to cited text no. 22 |
| 23. | Speer G, Cseh K, Winkler G, Vargha P, Braun E, TakaÂcs I, et al. Vitamin D and estrogen receptor gene polymorphisms in type 2 diabetes mellitus and in android type obesity. Eur J Endocrinol 2001;144:385-9. Back to cited text no. 23 |
| 24. | Calle C, Maestro B, Garcνa-Arencibia M. Genomic actions of 1,25-dihydroxyvitamin D3 on insulin receptor gene expression, insulin receptor number and insulin activity in the kidney, liver and adipose tissue of streptozotocin-induced diabetic rats. BMC Mol Biol 2008;9:65. Back to cited text no. 24 |
| 25. | Lee S, Clark SA, Gill RK, Christakos S. 1,25-Dihydroxyvitamin D3 and pancreatic -cell function: VDRs, gene expression, and insulin secretion. Endocrinology 1994;134:1602-10. Back to cited text no. 25 |
| 26. | Pittas AG, Lau J, Hu F, Dawson-Hughes B. The Role of Vitamin D and Calcium in type 2 diabetes. A systematic Review and Meta-Analysis. J Clin Endocrinol Metab 2007;92:2017-29. Back to cited text no. 26 |
| 27. | Knekt P, Laaksonen M, Mattila C, Hδrkδnen T, Marniemi J, Heliφvaara M, et al. Serum Vitamin D and Subsequent Occurrence of Type 2 Diabetes. Epidemiol 2008;19:666-71. Back to cited text no. 27 |
| 28. | Filus A, Trzmiel A, Kuliezkowska-Plaksej J, Tworowska U, Jedrzejuk D, Milewiez A, et al. Relationship between VDR BsmI and FokI polymorphism and anthropometric and biochemical parameters describing metabolic syndrome. Aging Male 2008;11:134-9. Back to cited text no. 28 |
| 29. | Naito M, Miyaki K, Naito T, Zhang L, Hoshi K, Hara A, et al. Association between vitamin D receptor gene haplotypes and chronic periodontitis among Japanese men. Int. J Med Sci 2007;4:216-22. Back to cited text no. 29 |
| 30. | Whitfield GK, Remus LS, Jurutka PW, Zitzer H, Oza AK, Dang HT, et al. Functionally relevant polymorphisms in the human nuclear vitamin D receptor gene. Mol Cell Endocrinol 2001;177: 145-59. Back to cited text no. 30 |
| 31. | American Diabetes Association. Screening for Type 2 Diabetes. Diabetes Care 2004;27:S11-S14. Back to cited text no. 31 |
| 32. | Harris SS, Eccleshall TR, Gross C, Dawson-Hughes B, Feldman D. The VDR start codon polymorphism (Fok-I) and bone mineral density in premenopausal American Black and White women. J Bone Miner Res 1997;12:1043-8. Back to cited text no. 32 |
| 33. | Morrison, NA, Qi JC, Tokita A, Kelly PJ, Crofts L, Nguyen TV, et al. Prediction of bone density from Vitamin D receptor. Nature 1994;367:284-7. Back to cited text no. 33 |
| 34. | Palomer X, Gonza´lez-Clemente JM, Blanco-Vaca F, Mauricio D. Role of vitamin D in the pathogenesis of type 2 diabetes mellitus. Diabetes Obes Metab 2008;10:185-97. Back to cited text no. 34 |
| 35. | Malecki MT, Frey J, Moczulski D, Klupa T, Kozek E, Sieradzki J. VDR gene polymorphisms and association with type 2 diabetes mellitus in a polish population. Exp Clin Endocrinol Diabetes 2003;111:505-9. Back to cited text no. 35 |
| 36. | Ye W, Reis AF, Dubois-Laforgue D, Bellanne-Chantelot C, Timsit J, Velho G. VDR gene polymorphisms are associated with obesity in type 2 diabetic subjects with early age of onset. Euro J Endocrinol 2001;145:181-6. Back to cited text no. 36 |
| 37. | Ortlepp JR, Lauscher J, Hoffmann R, Hanrath P, Joost HG. The VDR gene variant is associated with the prevalence of Type 2 diabetes mellitus and coronary artery disease. Diabet Med 2001;18:842-5. Back to cited text no. 37 |
| 38. | Oh J, Barrett-Connor E. Association between VDR Polymorphism and Type 2 Diabetes or Metabolic Syndrome in Community-Dwelling Older Adults: The Rancho Bernardo Study. Metabolism 2002;5:356-9. Back to cited text no. 38 |
| 39. | Cyganek K, Mirkiewicz-Sieradzka B, Malecki MT, Wolkow P, Skupien J, Bobrek J, et al. Clinical risk factors and the role of VDR gene polymorphisms in diabetic retinopathy in Polish type 2 diabetes patients. Acta Diabetol 2006;43:114-9. Back to cited text no. 39 |
Copyright 2009 - Indian Journal of Medical Sciences
The following images related to this document are available:
Photo images
[ms09036t4.jpg]
[ms09036t3.jpg]
[ms09036t2.jpg]
[ms09036t5.jpg]
[ms09036t1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}