 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
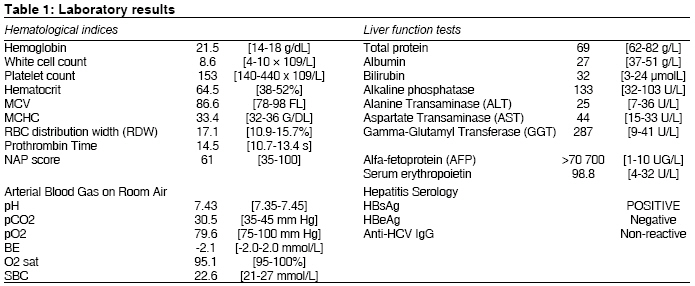
Indian Journal of Medical Sciences, Vol. 63, No. 5, May, 2009, pp. 202-203 Letter To Editor Paraneoplastic erythrocytosis as a primary presentation of hepatocellular carcinoma Chang Pik-Eu, Tan Chee-Kiat Department of Gastroenterology and Hepatology, Singapore General Hospital Code Number: ms09039 PMID: 19584492 Sir, A 55-year-old man with hypertension, diabetes mellitus and gout presented with generalized lethargy and weight loss. He was diagnosed as a hepatitis B carrier 5 years ago but was not on regular follow-up and did not undergo regular liver function tests or ultrasound examinations. He smoked 20 cigarettes per day for the past 30 years. Clinical examination revealed facial plethora, mild scleral icterus and conjunctival suffusion. He had hepatomegaly with a hard, irregular liver. The patient was fully orientated with no asterixis. He had minimal ascites, numerous spider nevi (>6) and palmar erythema. His hemoglobin count was elevated (21.5 g/dL) with a hematocrit concentration of 64.5%, indicative of polycythemia (erythrocytosis) [Table - 1]. Serum erythropoietin level was elevated, indicating a secondary polycythemia. Liver function tests revealed a cholestatic picture with markedly elevated alfa-fetoprotein (AFP) level. Triphasic CT abdomen revealed an enhancing heterogenous mass in the liver, measuring 9.0 x 6.6 cm, in segments 5 and 6, with evidence of invasion and thrombosis of the right portal vein; and a metastatic deposit in the left adrenal gland. The patient was diagnosed with advanced hepatocellular carcinoma (HCC) with portal vein thrombosis and adrenal metastasis, with paraneoplastic erythrocytosis due to increased tumor-related erythropoietin production. He underwent daily venesection for 4 days, which improved his hemoglobin to 17.9 g/dL. He was discharged well after 6 days but died suddenly 3 weeks later from an acute pulmonary embolism on a background of metastatic HCC. Paraneoplastic syndromes occur when a cancer produces substances (hormones, cytokines or tumor-related proteins) which circulate in the bloodstream, affecting the function of other tissues at a site distant from the tumor origin. The prevalence of HCC-related paraneoplastic erythrocytosis ranges from 1% to 3%. [1],[2] The underlying pathophysiology of HCC-related paraneoplastic erythrocytosis is multi-factorial. Firstly, local hypoxia from focal hepatic tumor necrosis leads to compensatory production of erythropoietin by the kidneys. Secondly, tumor cells themselves can directly produce erythropoietin in response to hypoxia. Thirdly, certain HCC cells are capable of producing "ectopic erythropoietin" even in the absence of tissue hypoxia. [3] Direct evidence of erythropoietin production by HCC cells was demonstrated by electron microscopy and immunohistochemistry of HCC tissue from patients with paraneoplastic erythrocytosis. [4] HCC-related paraneoplastic erythrocytosis is significantly associated with large tumor volume, markedly elevated AFP levels, advanced disease and reduced survival. [5] The high erythropoietin levels in such patients are a reflection of the advanced disease and large tumor burden. This case illustrates the importance of regular surveillance of hepatitis B carriers as they are 100 times more likely to develop liver cancer compared to uninfected individuals. Furthermore, the development of HCC in these patients may occur in the absence of symptoms or signs. As the incidence of HCC continues to rise, such paraneoplastic syndromes are likely to be encountered with increasing frequency. It is therefore important to recognize that erythrocytosis may be secondary to underlying HCC. This will aid in a more timely diagnosis of HCC, thus expediting appropriate treatment. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09039t1.jpg] |
| |||||||||

{kind=link}