
|
Indian Journal of Medical Sciences
Medknow Publications on behalf of Indian Journal of Medical Sciences Trust
ISSN: 0019-5359 EISSN: 1998-3654
Vol. 63, Num. 5, 2009, pp. 207-221
|
Indian Journal of Medical Sciences, Vol. 63, No. 5, May, 2009, pp. 207-221
Practitioners section
Adult - onset Still's disease : A review
Owlia MohammadBagher, Mehrpoor Golbarg
Department of Internal Medicine, Shahid Sadoughi University of Medical Sciences, Yazd
Correspondence Address:Division of Rheumatology, Shahid Sadoughi Hospital, Department of Internal Medicine, Safaeieh, Yazd 0098
golbargmehrpoor@yahoo.com
Code Number: ms09041
PMID: 19584494
DOI: 10.4103/0019-5359.53169
Abstract Objective: This article is an attempt to review recent literature regarding pathogenesis and clinical and laboratory findings in adult-onset Still's disease (AOSD).
Materials and methods: A search was conducted in PubMed and Ovid for English language publications, using individual or linked search terms "adult-onset Still's disease," "adult Still's disease," "Still's disease," "AOSD," and other related terms, from 1996 to 2009, and the clinically relevant articles were subsequently selected.
Results: More than 1000 titles were reviewed by the authors, and the most important concepts were selected from 143 full-text articles.
Conclusion: Adult-onset Still's disease (AOSD) is a rare systemic inflammatory disorder of unknown etiology and pathogenesis, usually presenting with high spiking fever accompanied by systemic manifestations. The disease is an entity with heterogeneous pathology; and diverse suggested etiologies, clinical manifestations and prognoses. There is no single diagnostic test for AOSD; rather, the diagnosis is based on a set of criteria, the most important of which are indeed clinical, but they also include paraclinical ones. Treatment aims at both minimizing inflammation and halting disease progression. For the former, nonsteroidal anti-inflammatory drugs have limited efficacy; so glucocorticoids in conjunction with disease-modifying antirheumatic drugs are also used. Novel therapeutic approaches such as anti-tumor necrosis factor blockade and monoclonal antibodies are promising.
Keywords: Adult-onset Still′s disease, adult Still′s disease, Still′s disease
Introduction
Adult-onset Still′s disease (AOSD) is a rare inflammatory disorder of unknown etiology. Its main features are high spiking fever; evanescent rash; polyarthralgia; lymphadenopathy; hepatosplenomegaly; leukocytosis; and elevated liver enzymes, erythrocyte sedimentation rate (ESR) and ferritin. [1] The first description of an adult patient with signs and symptoms of AOSD (erroneously labeled rheumatoid arthritis) was published in 1896. [2] In 1971, Eric Bywaters described 14 adults with presentation similar to that of pediatric Still′s disease; hence he used the term AOSD. [3],[4]
Materials and Methods We searched in the PubMed and Ovid from 1996 to 2009, using keywords "adult-onset Still′s disease," "adult Still′s disease," "Still′s disease" and "AOSD" in combination with "fever of unknown origin." We found more than 1000 titles. From among these titles, 143 published full-text English-language articles were identified for inclusion in this review. These articles, which included important case reports, original articles and review articles, were extensively reviewed by the authors. No randomized controlled trial was found, which may be due to the rarity of this disease. Major textbooks on rheumatology were also reviewed for background information.
Epidemiology Prevalence of AOSD is estimated to be 1.5 cases per 100,000-1000,000 people. It occurs worldwide and has been reported from France, [5],[6] Norway, [7] Japan, [8],[9] Greece, [10] USA, [11] Taiwan, [12],[13] Spain, [14] Korea, [15],[16] China, [17],[18] Turkey, [19],[20] India [21],[22] and Iran. [23] The disease affects young people and has a bimodal age distribution with two peaks - at 15-25 and 36-46 years of age. [24] It is generally considered a disorder of youth, [25] but there are several reports of new cases of AOSD in older people. [24],[26] The disease affects a slightly larger number of women as compared to men. [19],[23] On the other hand, in some case series, male-to-female ratio was seen to be high. [4],[6],[21]
Pathogenesis
The etiology of the disease is not fully understood. Observations supporting the role of genetic, infectious and environmental factors have been published. In a review of 62 patients, HLAB17, B18, B35 and DR2 were associated with AOSD. [6] The existence of relationship of DRB1FNx0112, DRB1FNx0115 and HLA-DRB1FNx0104 with AOSD was reported in Korean patients. [27] In another study on Japanese patients, DRB1FNx011501 (DR2) and DRB1FNx011201 (DR5) alleles were more frequent in chronic articular than in polycyclic systemic AOSD; whereas DQB1FNx010602 (DQ1) was observed in all types of AOSD. [28] Polymorphism in IL-1 and IL-18 genes was proposed by a few authors as a possible mechanism in pathogenesis of AOSD, but the former was not found to be associated with AOSD. Also, possession of the diplotype configuration of S01/S01 was found to be a major genetic risk factor for susceptibility to AOSD. [29],[30],[31]
Several reports have indicated the role of infectious factors but have not proved anything decisively. Viruses like rubella, [32] Epstein-Barr virus, [33] human herpes virus (HHV6), [34] hepatitis B and C, [35],[36] parvovirus B19, [37] cytomegalovirus, [38] human immunodeficiency virus (HIV); [39],[40] and bacteria like Mycoplasma pneumonia, Chlamydia pneumonia, Chlamydia trachomatis are considered to be risk factors. [41],[42],[43]
Several cytokines have been described in the pathogenesis of AOSD, including interleukin (IL)-1, IL-6, tumor necrosis factor-alpha (TNF-a) and IL-18. Serum levels of these cytokines are highly elevated in active AOSD. [44] Higher levels of IL-18, IFN-γ, sIL-2R and IL-8 were shown in patients with AOSD as compared to healthy controls. There is a positive correlation between serum IL-18, sIL-2R and the level of serum ferritin In active AOSD. [45] Chen demonstrated that the mean percentage of Th1 cells was significantly higher in active AOSD , correlating with clinical activity score and serum IL-18, which plays a critical role in AOSD. [46] In several studies, it has been shown that high levels of IL-18 correlate with disease activity, and this is a predictor of liver dysfunction. [47],[48] It has been also demonstrated for the first time that in biopsy specimens from skin lesions and synovium of patients with AOSD, Th1/Th2 cytokine mRNA expression is significantly higher than that in the specimens from healthy controls. [46]
Intercellular adhesion molecule 1 (ICAM-1) has been shown to be significantly higher in AOSD patients as compared with rheumatoid arthritis (RA) patients or healthy controls. Serum ICAM-1 levels correlate well with the clinical activity score, serum levels of ferritin, and aminotransferase in patients with AOSD. [49]
Clinical Manifestations
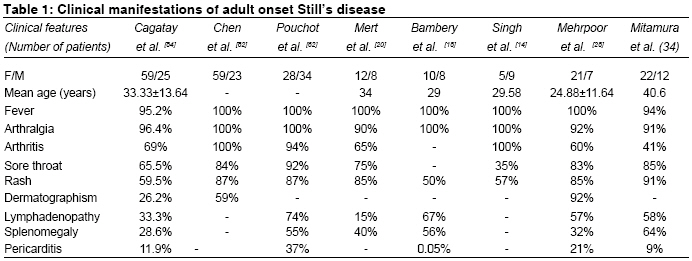
Fever, rash, sore throat and arthralgia are the most typical clinical features of AOSD. [4] Over 99% of patients manifest a fever ≥39°C. Fever is the most commonly quotidian or double quotidian manifestation. The highest temperatures are seen in late afternoon or early evening. [50] In the differential diagnosis of a patient with FUO (fever of unknown origin), AOSD should be considered; and maculopapular rashes, arthralgia and sore throat should raise the suspicion of AOSD. [51],[52],[53],[54] Low-grade and atypical pattern of fever is sometimes seen in older patients. [19] Febrile spikes are often accompanied by exacerbation of the other symptoms like rash, fatigue and arthralgia. [55]
The classic rash is an evanescent, salmon-pink, maculopapular eruption, which frequently appears during febrile attacks and is predominantly found on the proximal limbs and trunk with rare involvement of the face and distal limbs. [4],[56],[57] The rash can be mildly pruritic or may be associated with burning. In general, the Still rash lasts for hours and changes daily; although in some patients, the duration of the rash correlates well with the degree of systemic activity, and the rash may last for days without change. [50] It can be induced by a minor trauma (Kobner phenomenon). [58] Urticaria, [59],[60] dermal plaque, [61],[62],[63] vesicles and pustules [64] are also described. Several atypical rashes have been reported. [65],[66] Skin biopsy shows nonspecific inflammation and mild perivascular inflammation. Immunofluorescence of the skin biopsy may show some slight deposition of C3 at blood vessel wall. [67] Dermatographism is a frequently encountered phenomenon in patients with AOSD. [23]
The onset of the disease is usually heralded by a sore throat and constitutional manifestations. Sore throat is known as a cardinal sign of AOSD and may be associated with odynophagia. [68] Despite the presence of marked sore throat in most cases, physical examinations fail to show any significant findings. Throat cultures are negative, and viral serological tests are nondiagnostic in all AOSD patients. Antibiotic therapy is ineffective. Magnetic resonance imaging (MRI) of the larynx in 6 active AOSD patients has demonstrated cricothyroid perichondritis. [68],[69]
Arthralgia and arthritis occur in about 64% to 100% of the patients, and flare-up of joint symptoms occurs during the febrile spikes. [6],[70],[71] Presence of arthritis before constitutional and extra-articular manifestations is rare. [19] The most common joints involved are the knees, wrists, ankles and elbows. Sacroiliac involvement is uncommon but has been reported. [21],[72] Narrowing of the carpometacarpal and intercarpal joint spaces is said to be specific for AOSD (as compared to more frequent radiocarpal joint involvement in RA). [73],[74] Destructive arthritis is found in 25% of patients, and carpal joints are the most affected joints. [4],[74] Destructive arthritis of the hips occurs in 5% to 33% of patients. [6],[25] Joint fluid aspirate often discloses marked leukocytosis, with a neutrophilic predominance. [50] Generalized myalgia is seen in many patients and can be severe and coincide with fever spikes. [6],[9]
Lymphadenopathy develops in approximately 44% to 90% of patients with AOSD [25],[55],[75] and may raise suspicion of lymphoma initially. [76],[77],[78],[79] AOSD lymphadenopathy represents a wide spectrum of histopathological features: normal or nondiagnostic reactive hyperplasia, atypical paracortical hyperplasia, burnt-out histiocytic reaction, immunoblastic reaction and follicular hyperplasia. Occasionally, lymph node histology in AOSD may mimic malignant lymphoma. [16] Hepatosplenomegaly is common in early disease and reflects tissue infiltration by inflammatory cells. [19],[23],[80] Macrophage activation syndrome (MAS) is a life-threatening condition, which is characterized by uncontrolled activation and proliferation of T lymphocytes and macrophages in bone marrow, reticuloendothelial system and central nervous system. [81] MAS is a dreaded complication of rheumatic diseases, especially systemic-onset juvenile rheumatoid arthritis (JRA). [82] It has also been reported in AOSD and should be considered in patients with AOSD when it presents with acute febrile illness; hepatosplenomegaly; lymphadenopathy; pancytopenia; increased serum liver enzymes; coagulopathy; central nervous system, pulmonary or renal involvement. [11],[81] Hemophagocytosis which is seen in bone marrow aspiration and biopsy establishes the diagnosis, even though hemophagocytosis could be seen more frequently in biopsies from liver, lymph node and spleen. [82]
The reactive hemophagocytic syndrome (RHS) is a term describing a condition similar to MAS from the clinical and also the laboratory standpoint in patients with AOSD. It is characterized by fever, hepatosplenomegaly, lymphadenopathy, pancytopenia and increased serum liver enzymes, ferritin and triglycerides, which have been also described in MAS. [83] Despite similar immunologic abnormalities in MAS and RHS, there are significant heterogenic mechanisms leading to abnormal cytotoxicity in RHS and MAS; [84] although in recent studies, it is seen that authors believe that MAS is the primary type of hemophagocytic syndrome. [82] RHS is not so rare in AOSD, even though it could be underdiagnosed in clinical practice. [83]
Disseminated intravascular coagulopathy (DIC) is a critical condition secondary to pathological activation of coagulation system that occurs in the setting of several conditions, notably AOSD. This entity has been reported by some authors in AOSD. [85],[86],[87],[88]
There are several case reports about AOSD emerging first in pregnancy. [89],[90],[91] AOSD could be seen clinically in 3 forms: a self-limited or monocyclic pattern, an intermittent or polycyclic systemic pattern, and a chronic articular pattern. [19]
In [Table - 1], clinical manifestations of AOSD that have been reported in various case series are shown.
Laboratory Investigations
An elevated ESR and leukocytosis more than 15000/µL are present in most of the patients. The findings of liver function tests may be elevated in up to three fourths of patients. [25],[92] Anemia of chronic disease is common. Pancytopenia has been described in AOSD associated with hemophagocytic syndrome (HS). [93] Rheumatoid factor and antinuclear antibody tests are generally negative and, if positive, these are of low titers. [6] Synovial and serosal fluids are inflammatory type with a predominance of neutrophils. [50]
High levels of ferritin seem to be characteristic of AOSD. [3],[19],[68] Nearly 70% of patients have hyper-ferritinemia. [68] Cagatay reported very high levels of ferritin (>2000) in 38% of patients. High levels of ferritin can be seen in other diseases such as liver disease, infections and malignancies and especially in the hemophagocytic syndrome. Ferritin levels in AOSD are usually higher than those found in other autoimmune or inflammatory diseases. [3],[68] Hyper-ferritinemia in AOSD is not related to iron metabolism and is likely to be a consequence of cytokine secretion induced by the reticuloendothelial system or hepatic damage; [3],[19],[94] but in most cases, ferritin levels are increased in the absence of overt liver damage. [3] Several cytokines - mainly, IL1b, IL-18, TNF-α and IL6 - seem to have some role in increasing the production of ferritin. A more specific diagnostic marker may be drop in glycosylated ferritin. In AOSD, decreased glycosylated ferritin, an isoform of ferritin, was noted in comparison with other inflammatory diseases. In 50% to 80% of healthy individuals, ferritin is glycosylated; while in inflammatory diseases, it drops to 20%-50%; and in AOSD, less than 20%. [3],[95] Recently, in some studies, it was shown that hyper-ferritinemia, which is correlated to histiocyte hyperactivity, can lead to an association of AOSD with MAS. [19] Hyper-ferritinemia with a value between 4000 and 30000 mg/dL has been reported in association with onset and disease activity. [96]
The validity of the diagnostic test for hyper-ferritinemia has been evaluated in a retrospective study, where a fivefold increase in serum ferritin has 41% specificity and 80% sensitivity. [97] Furthermore, serum ferritin levels correlate with disease activity; and after remission, they get normalized. Glycosylated ferritin cannot be used to monitor disease activity or response to treatment, because it remains low for many months after the disease goes into remission. [98],[99] Normal levels of total serum ferritin are not a criterion for exclusion of a diagnosis of AOSD. [100] Liver dysfunction in AOSD is frequent, and hepatic involvement can range from mildly elevated transaminases to severe hepatic failure unresponsive to treatment. [25],[101],[102],[103]
The results of radiography are normal in the early phase of disease and may be helpful in the late stages and chronic phase, with emerging erosions, joint space narrowing or frank ankylosis. [73],[104]
Differential Diagnosis
Before considering AOSD, many other diagnoses should be ruled out. Acute or chronic infections such as brucellosis, tuberculosis and bacterial endocarditic infections; malignant diseases, especially lymphoma; and autoimmune disorders like systemic lupus erythematosus and systemic vasculitides are among the most important differential diagnoses.
Diagnostic Criteria
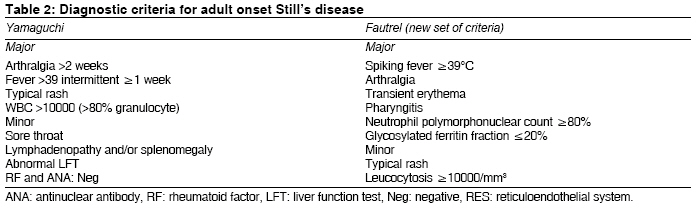
Despite the constellation of characteristic clinical manifestations, the diagnosis of AOSD is difficult in some instances, due to absence of specific serological and pathological findings. The Yamaguchi′s criteria are the most widely cited criteria and were shown to be the most sensitive ones (93.5%). [105],[106] In 2002, a new set of criteria were proposed by Fautrel et al., which contained 2 new markers: serum ferritin and its glycosylated fraction. It does not have any exclusion criterion. [71] The sensitivity and specificity of Fautrel criteria were 80.6% and 98.5%, respectively. In [Table - 2], the two diagnostic criteria are shown.
Treatment
Aspirin or NSAIDs are recommended as the initial treatment in AOSD, but the response rate is reported to be as low as 20% to 25%. [107] Liver enzymes should be closely monitored in patients in whom NSAIDs are used. [75],[108] Since response to NSAID monotherapy is not enough, most patients are treated with corticosteroids in the course of their disease, with an efficacy of up to 95%. Prednisolone should be used for the patient who does not respond to NSAIDs and also for patients suffering from persistent anemia, pericarditis, serositis and marked elevation of liver enzymes. [50],[109]
In a small number of case reports where the disease persisted despite administration of prednisolone, dexamethasone was used successfully. [110] Similarly, another case report demonstrated the efficacy of high-dose intravenous pulse methylprednisolone in treating disease refractory to prednisolone. [111] Intra-articular steroid injection is an important option in the treatment of AOSD patients with severe and chronic joint disease. [112]
Disease-modifying antirheumatic drugs (DMARDs) such as methotraxate (MTX), azathioprine, cyclosporine, cyclophophamide have been used for maintenance therapy and control of disease. [113] Sulfasalazine appears to have severe adverse reactions in AOSD, as in systemic-onset JRA, and should be avoided in AOSD. [21],[114] MTX is used in the treatment of AOSD due to its steroid-sparing effect. In many cases, arthritis and joint destruction are particularly found to respond to MTX administration. [24],[115] Cyclosporine is a valuable option in the treatment of AOSD and MAS. [81] In one case report, cyclosporine was used for treatment of AOSD with disseminated intravascular coagulation and multiple organ dysfunctions. [85]
Given the role of proinflammatory cytokines such as IL1a, IL6 and TNF-α in the pathogenesis of AOSD, biologic agents have been used by some clinicians. Biological therapies can be administered to patients that do not respond to conventional medications such as corticosteroids and DMARDs. [116],[117],[118],[119]
In various trials, use of infliximab, the monoclonal chimeric anti-TNF-α antibody, has also been reported to be effective in AOSD. In a study of 3 patients with chronic AOSD unresponsive to conventional treatment with prednisone and MTX, addition of infliximab (3 mg/kg in weeks 0, 2, 6, and every 8 weeks thereafter) led to improvements in both clinical and laboratory parameters. [119] In a Greek case series, 4 patients refractory to high doses of corticosteroids and MTX responded favorably to treatment with infliximab 3 mg/kg. [120] Infliximab at a dose of 5 mg/kg was found to be effective in a patient with early AOSD who was steroid resistant and ineligible for MTX treatment. [121] In another study, after administering infliximab to a patient of AOSD with persistent proteinuria and arthritis, proteinuria was decreased and arthritis was improved. [122] Adalimumab, which is an injectable protein that blocks the inflammatory effects of tumor necrosis factor-alpha (TNF-alpha), was also used in an AOSD patient. [123]
TNF-blocking agents (etanercept) have been employed in some studies. [124],[125] Etanercept in conjunction with MTX and corticosteroids was used successfully by Asherson and Pascoe in a single patient when multiple immunosuppressive drugs and plasmapheresis had failed. [126] Furthermore, etanercept was used in a patient with Still′s disease and nephrotic syndrome due to renal AA amyloidosis, resulting in amelioration of proteinuria. [127] Deng-Ho Yang described a patient with flared-up AOSD and congestive heart failure due to left ventricular dysfunction. The patient showed no improvement with glucocorticoid therapy, but dramatic response was seen in the imaging and laboratory studies after therapy with etanercept. [128]
Administration of tacrolimus may be effective for patients with AOSD, even when TNF inhibitors and cyclosporine are not effective. [129]
Most recently, IL1 blockade (anakinra) has been used as a possible new therapeutic option. It was first used in a patient with refractory AOSD in the year 2005. After administration of anakinra, the patient achieved a prolonged remission. [130],[131] Another study also showed the efficacy of anakinra in the treatment of 4 patients with AOSD that were refractory to treatment with corticosteroids and MTX. In all the 4 cases, the patients responded quickly to anakinra; symptoms resolved within days and laboratory values (WBC count, ferritin, C- Reactive Protein) were normalized. [132]
Due to the central role of IL-1Ra in fulminant hepatic failure, anakinra was administered to a patient with AOSD complicated with acute hepatitis; the patient dramatically improved. [133] Plasma exchange [134],[135] and intravenous immunoglobulin [136],[137],[138] are the other treatments which were used in AOSD. These options were used in the treatment of patients with refractory AOSD with high serum levels of interleukin-10 and -18 (hypercytokinemia). Plasmapheresis [40 units of fresh frozen plasma six times totally (twice a week x 3 weeks)] resulted in rapid reduction in the elevated cytokine levels in the peripheral blood. The use of Intra VenousImmuno Globolin (IVIG) in AOSD has also been described in the treatment of flares at doses ranging from 0.4 to 2 g/kg/day for 2 to 5 days. Also in AOSD associated with pregnancy, IVIG 1 g/kg/day resulted in complete remission in one study.
Rituximab (monoclonal antibody, antiCD20) is a new option in treatment; there are some case reports about its usefulness in AOSD. [23],[139]
Leflunomide, an immunomodulating agent, is used as a disease-modifying drug in rheumatoid arthritis. Inhibition of dihydro-orotate reductase by the A771726, the active metabolite of leflunomide, results in decreased lymphocyte proliferation. In addition, it seems that production of tumor necrosis factor-alfa, interleukin-1, nitric oxide and matrix metalloproteinase-3 by human synovial cells is inhibited by the A771726. In a few case reports, the efficacy of leflunomide was shown in the treatment of AOSD. [140],[141],[142]
As noted above, one of the cytokines that play an important role in AOSD is IL-6. It is suggested that systemic manifestations of AOSD, such as fever, leukocytosis and elevated ESR, are mediated by overproduction of IL-6. Tocilizumab, a humanized anti-IL-6 receptor (IL-6R) monoclonal antibody of the IgG1 subclass, has been addressed in 2 case reports as being effective for AOSD. [143]
Acknowledgment
We thank Professor F. Davatchi, Mr. A. Eslamizadeh and S. Owlia for their contribution and useful comments.
References
| 1. | Bywaters EG. Still's disease in the adult. Ann Rheum Dis 1971;30:121-33. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Efthimiou P, Paik PK, Bielory L. Diagnosis and management of adult onset Still's disease. Ann Rheum Dis 2006;65:564-72. Back to cited text no. 2 [PUBMED] [FULLTEXT] |
| 3. | Meijvis SC, Endeman H, Geers AB, ter Borg EJ. Extremely high serum ferritin levels as diagnostic tool in adult-onset Still's disease. Neth J Med 2007;65:212-4. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Larson EB. Adult Still's disease--recognition of a clinical syndrome and recent experience. West J Med 1985;142:665-71. Back to cited text no. 4 [PUBMED] [FULLTEXT] |
| 5. | Magadur-Joly G, Billaud E, Barrier JH, Pennec YL, Masson C, Renou P, et al. Epidemiology of adult Still's disease: Estimate of the incidence by a retrospective study in west France. Ann Rheum Dis 1995;54:587-90. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Pouchot J, Sampalis JS, Beaudet F, Carette S, Decary F, Salusinsky-Sternbach M, et al. Adult Still's disease: Manifestations, disease course, and outcome in 62 patients. Medicine (Baltimore) 1991;70:118-36. Back to cited text no. 6 |
| 7. | Evensen KJ, Nossent HC. Epidemiology and outcome of adult-onset Still's disease in Northern Norway. Scand J Rheumatol 2006;35:48-51. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Wakai K, Ohta A, Tamakoshi A, Ohno Y, Kawamura T, Aoki R, et al. Estimated prevalence and incidence of adult Still's disease: Findings by a nationwide epidemiological survey in Japan. J Epidemiol 1997;7:221-5. Back to cited text no. 8 [PUBMED] |
| 9. | Ohta A, Yamaguchi M, Tsunematsu T, Kasukawa R, Mizushima H, Kashiwagi H, et al. Adult Still's disease: A multicenter survey of Japanese patients. J Rheumatol 1990;17:1058-63. Back to cited text no. 9 [PUBMED] |
| 10. | Akritidis N, Papadopoulos A, Pappas G. Long-term follow-up of patients with adult-onset Still's disease. Scand J Rheumatol 2006;35:395-7. Back to cited text no. 10 [PUBMED] [FULLTEXT] |
| 11. | Stern A, Riley R, Buckley L. Worsening of macrophage activation syndrome in a patient with adult onset Still's disease after initiation of etanercept therapy. J Clin Rheumatol 2001;7:252-6. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Chen DY, Lan JL, Hsieh TY, Chen YH. Clinical manifestations, disease course, and complications of adult-onset Still's disease in Taiwan. J Formos Med Assoc 2004;103:844-52. Back to cited text no. 12 [PUBMED] |
| 13. | Lee JY, Yang CC, Hsu MM. Histopathology of persistent papules and plaques in adult-onset Still's disease. J Am Acad Dermatol 2005;52:1003-8. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
| 14. | Garcia-Porrua C, Gonzalez-Gay MA, Crespo F, Gonzalez-Juanatey C. Adult onset Still's disease in Catalonia, Spain. J Rheumatol 2000;27: 280-1. Back to cited text no. 14 |
| 15. | Oh YB, Ahn JY, Lee HS, Kim TH, Jun JB, Jung SS, et al. Association Between FcgammaR IIa and IIIa polymorphism and clinical manifestations in Korean patients with adult-onset Still's disease. J Korean Med Sci 2002;17:75-80. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Jeon YK, Paik JH, Park SS, Park SO, Kim YA, Kim JE, et al. Spectrum of lymph node pathology in adult onset Still's disease: Analysis of 12 patients with one follow up biopsy. J Clin Pathol 2004;57:1052-6. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
| 17. | Mok CC, Lau CS, Wong RW. Clinical characteristics, treatment, and outcome of adult onset Still's disease in southern Chinese. J Rheumatol 1998;25:2345-51. Back to cited text no. 17 [PUBMED] |
| 18. | Lin SJ, Chao HC, Yan DC. Different articular outcomes of Still's disease in Chinese children and adults. Clin Rheumatol 2000;19:127-30. Back to cited text no. 18 [PUBMED] [FULLTEXT] |
| 19. | Cagatay Y, Gul A, Cagatay A, Kamali S, Karadeniz A, Inanc M, et al. Adult-onset still's disease. Int J Clin Pract 2007 18. Back to cited text no. 19 |
| 20. | Pay S, Turkcapar N, Kalyoncu M, Simsek I, Beyan E, Ertenli I, et al. A multicenter study of patients with adult-onset Still's disease compared with systemic juvenile idiopathic arthritis. Clin Rheumatol 2006;25:639-44. Back to cited text no. 20 |
| 21. | Singh S, Samant R, Joshi VR. Adult onset Still's disease: A study of 14 cases. Clin Rheumatol 2008;27:35-9. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
| 22. | Uppal SS, Pande IR, Kumar A, Kailash S, Sekharan NG, Adya CM, et al. Adult onset Still's disease in northern India: Comparison with juvenile onset Still's disease. Br J Rheumatol 1995;34:429-34. Back to cited text no. 22 [PUBMED] [FULLTEXT] |
| 23. | Mehrpoor G, Owlia MB, Soleimani H, Ayatollahi J. Adult-onset Still's disease: A report of 28 cases and review of the literature. Mod Rheumatol 2008;28. Back to cited text no. 23 |
| 24. | Kurasawa M, Kotani K, Kurasawa G, Shida K, Yamada S, Tago T. Adult-onset Still's disease in a patient over 80 years old successfully treated with low-dose methotrexate therapy. Age Ageing 2007;36:104-6. Back to cited text no. 24 [PUBMED] [FULLTEXT] |
| 25. | Ohta A, Yamaguchi M, Kaneoka H, Nagayoshi T, Hiida M. Adult Still's disease: Review of 228 cases from the literature. J Rheumatol 1987;14:1139-46. Back to cited text no. 25 [PUBMED] |
| 26. | Ichiki H, Shishido M, Nishiyama S. Two cases of adult onset of Still's disease in the elderly. Nippon Ronen Igakkai Zasshi 1992;29:960-4. Back to cited text no. 26 [PUBMED] |
| 27. | Joung CI, Lee HS, Lee SW, Kim CG, Song YH, Jun JB, et al. Association between HLA-DR B1 and clinical features of adult onset Still's disease in Korea. Clin Exp Rheumatol 2003;21:489-92. Back to cited text no. 27 [PUBMED] |
| 28. | Fujii T, Nojima T, Yasuoka H, Satoh S, Nakamura K, Kuwana M, et al. Cytokine and immunogenetic profiles in Japanese patients with adult Still's disease. Association with chronic articular disease. Rheumatology (Oxford) 2001;40:1398-404. Back to cited text no. 28 |
| 29. | Youm JY, Woo JH, Kim TH, Bae SC, Yoo DH. Interleukin-1beta and interleukin-1 receptor antagonist gene polymorphisms in Korean patients with adult-onset Still's disease. Scand J Rheumatol 2007;36:390-3. Back to cited text no. 29 [PUBMED] [FULLTEXT] |
| 30. | Sugiura T, Kawaguchi Y, Harigai M, Terajima-Ichida H, Kitamura Y, Furuya T, et al. Association between adult-onset Still's disease and interleukin-18 gene polymorphisms. Genes Immun 2002;3:394-9. Back to cited text no. 30 [PUBMED] [FULLTEXT] |
| 31. | Sugiura T, Maeno N, Kawaguchi Y, Takei S, Imanaka H, Kawano Y, et al. A promoter haplotype of the interleukin-18 gene is associated with juvenile idiopathic arthritis in the Japanese population. Arthritis Res Ther 2006;8:R60. Back to cited text no. 31 [PUBMED] [FULLTEXT] |
| 32. | Escudero FJ, Len O, Falco V, de Sevilla TF, Sellas A. Rubella infection in adult onset Still's disease. Ann Rheum Dis 2000;59:493. Back to cited text no. 32 |
| 33. | Schifter T, Lewinski UH. Adult onset Still's disease associated with Epstein-Barr virus infection in a 66-year-old woman. Scand J Rheumatol 1998;27:458-60. Back to cited text no. 33 [PUBMED] |
| 34. | Daibata M, Taguchi H. Human herpesvirus 6 and adult-onset Still's disease. Am J Med 2002;113:532. Back to cited text no. 34 [PUBMED] [FULLTEXT] |
| 35. | Gambichler T, Paech V, Rotterdam S, Stucker M, Boms S, Altmeyer P. Hepatitis B-assocciated adult-onset Still's disease presenting with neutrophilic urticaria. Eur J Med Res 2003;9:527-30. Back to cited text no. 35 |
| 36. | Castanet J, Lacour JP, Fuzibet JG, Perrin C, Rodot S, Ortonne JP. Adult Still's disease associated with hepatitis C virus infection. J Am Acad Dermatol 1994;31:807-8. Back to cited text no. 36 [PUBMED] |
| 37. | Blidi M, Gatfosse M, Barjonet G. Adult-onset Still disease associated with acute parvovirus B19 infection in pregnancy. Ann Med Interne (Paris) 1996;147:518-9. Back to cited text no. 37 [PUBMED] |
| 38. | Amenomori M, Migita K, Miyashita T, Yoshida S, Ito M, Eguchi K, et al. Cytomegalovirus-associated hemophagocytic syndrome in a patient with adult onset Still's disease. Clin Exp Rheumatol 2005;23:100-2. Back to cited text no. 38 [PUBMED] |
| 39. | Antinori S, Rusconi S, Ridolfo AL, Orlando G. Still's disease in a patient infected with human immunodeficiency virus type I. Clin Exp Rheumatol 1995;13:759-61. Back to cited text no. 39 [PUBMED] |
| 40. | DelVecchio S, Skidmore P. Adult-onset Still's disease presenting as fever of unknown origin in a patient with HIV infection. Clin Infect Dis 2008;46:e41-3. Back to cited text no. 40 [PUBMED] [FULLTEXT] |
| 41. | Perez C, Artola V. Adult Still's disease associated with Mycoplasma pneumoniae infection. Clin Infect Dis 2001;32:E105-6. Back to cited text no. 41 |
| 42. | Takeda H, Ling M, Ochi M, Watanabe K. A patient with adult Still's disease with an increased Chlamydia pneumoniae antibody titer. J Infect Chemother 2002;8:262-5. Back to cited text no. 42 [PUBMED] [FULLTEXT] |
| 43. | Andres E, Imler M. A patient with adult Still's disease and high Chlamydia trachomatis titers. J Infect Chemother 2003;9:194. Back to cited text no. 43 |
| 44. | Chen DY, Lan JL, Lin FJ, Hsieh TY. Proinflammatory cytokine profiles in sera and pathological tissues of patients with active untreated adult onset Still's disease. J Rheumatol 2004;31:2189-98. Back to cited text no. 44 [PUBMED] [FULLTEXT] |
| 45. | Choi JH, Suh CH, Lee YM, Suh YJ, Lee SK, Kim SS, et al. Serum cytokine profiles in patients with adult onset Still's disease. J Rheumatol 2003;30:2422-7. Back to cited text no. 45 [PUBMED] [FULLTEXT] |
| 46. | Chen DY, Lan JL, Lin FJ, Hsieh TY, Wen MC. Predominance of Th1 cytokine in peripheral blood and pathological tissues of patients with active untreated adult onset Still's disease. Ann Rheum Dis 2004;63:1300-6. Back to cited text no. 46 [PUBMED] [FULLTEXT] |
| 47. | Arlet JB, Le Thi Huong DB, Pouchot J, Piette JC. Current concepts on the physiopathology of adult-onset Still's disease. Rev Med Interne 2005;26:549-56. Back to cited text no. 47 [PUBMED] [FULLTEXT] |
| 48. | Esdaile JM, Tannenbaum H, Lough J, Hawkins D. Hepatic abnormalities in adult onset Still's disease. J Rheumatol 1979;6:673-9. Back to cited text no. 48 [PUBMED] |
| 49. | Chen DY, Lan JL, Lin FJ, Hsieh TY. Association of intercellular adhesion molecule-1 with clinical manifestations and interleukin-18 in patients with active, untreated adult-onset Still's disease. Arthritis Rheum 2005;53:320-7. Back to cited text no. 49 [PUBMED] [FULLTEXT] |
| 50. | Cush JJ. Adult-onset Still's disease. Bull Rheum Dis 2000;49:1-4. Back to cited text no. 50 |
| 51. | Bambery P, Thomas RJ, Malhotra HS, Kaur U, Bhusnurmath SR, Deodhar SD. Adult onset Still's disease: clinical experience with 18 patients over 15 years in northern India. Ann Rheum Dis 1992;51:529-32. Back to cited text no. 51 [PUBMED] [FULLTEXT] |
| 52. | Mert A, Ozaras R, Tabak F, Bilir M, Ozturk R, Ozdogan H, et al. Fever of unknown origin: a review of 20 patients with adult-onset Still's disease. Clin Rheumatol 2003;22:89-93. Back to cited text no. 52 |
| 53. | Crispin JC, Martinez-Banos D, Alcocer-Varela J. Adult-onset Still disease as the cause of fever of unknown origin. Medicine (Baltimore) 2005;84:331-7. Back to cited text no. 53 |
| 54. | Owlia MB. clinical spectrum of connective tissue disorders. J Indian Acad Community Med 2006;7:217-24. Back to cited text no. 54 |
| 55. | Cush JJ, Medsger TA, Jr., Christy WC, Herbert DC, Cooperstein LA. Adult-onset Still's disease: Clinical course and outcome. Arthritis Rheum 1987;30:186-94. Back to cited text no. 55 |
| 56. | Phillips WG, Weller R, Handfield-Jones SE, Kobza-Black A. Adult Still's disease. Br J Dermatol 1994;130:511-3. Back to cited text no. 56 |
| 57. | Ridgway HA. Adult-onset Still's disease. J R Soc Med 1982;75:474-6. Back to cited text no. 57 |
| 58. | Sunderkotter C, Frieling U, Nashan D, Metze D. Adult-onset Still's disease and its characteristic rash. Hautarzt 1998;49:920-4. Back to cited text no. 58 |
| 59. | Criado RF, Criado PR, Vasconcellos C, Szajubok JC, Michalany NS, Kadunc BV, et al. Urticaria as a cutaneous sign of adult-onset Still's disease. J Cutan Med Surg 2006;10:99-103. Back to cited text no. 59 |
| 60. | Salaffi F, Filosa G, Bugatti L, Maestrini MD. Urticaria as a presenting manifestation of adult-onset Still's disease. Clin Rheumatol 2000;19:389-91. Back to cited text no. 60 |
| 61. | Kaur S, Bambery P, Dhar S. Persistent dermal plaque lesions in adult onset Still's disease. Dermatology 1994;188:241-2. Back to cited text no. 61 |
| 62. | Thien Huong NT, Pitche P, Minh Hoa T, Laurent R. Persistent pigmented plaques in adult-onset Still's disease. Ann Dermatol Venereol 2005;132:693-6. Back to cited text no. 62 |
| 63. | Fernandez-Guarino M, Gonzalez C, Bardal Ruiz A, Calvo Pulido M, Harto Castano A, Jaen Olasolo P. Adult Still's disease with atypical skin manifestations. Actas Dermosifiliogr 2006;97:591-3. Back to cited text no. 63 |
| 64. | Lee JB, Kim JW, Lee SS, Kim SJ, Won YH, Lee SC. Adult-onset Still's disease with vesiculopustules on the hands and feet. J Korean Med Sci 2002;17:852-5. Back to cited text no. 64 |
| 65. | Affleck AG, Littlewood SM. Adult-onset Still's disease with atypical cutaneous features. J Eur Acad Dermatol Venereol 2005;19:360-3. Back to cited text no. 65 |
| 66. | Saito A, Sato Y, Miyata M, Nishimaki T, Kasukawa R. Two cases of adult Still's disease with atypical rash. Ryumachi 1998;38:516-22. Back to cited text no. 66 |
| 67. | Elkon KB, Hughes GR, Bywaters EG, Ryan PF, Inman RD, Bowley NB, et al. Adult-onset Still's disease: Twenty-year followup and further studies of patients with active disease. Arthritis Rheum 1982;25:647-54. Back to cited text no. 67 |
| 68. | Kelly J, Chowienczyk P, Gibson T. Sore throat and hyperferritinaemia. J R Soc Med 2001;94:400-1. Back to cited text no. 68 |
| 69. | Chen DY, Lan HH, Hsieh TY, Chen HH, Lan JL. Crico-thyroid perichondritis leading to sore throat in patients with active adult-onset Still's disease. Ann Rheum Dis 2007;66:1264-6. Back to cited text no. 69 |
| 70. | Wouters JM, van de Putte LB. Adult-onset Still's disease: Clinical and laboratory features, treatment and progress of 45 cases. Q J Med 1986;61:1055-65. Back to cited text no. 70 |
| 71. | Fautrel B, Zing E, Golmard JL, Le Moel G, Bissery A, Rioux C, et al. Proposal for a new set of classification criteria for adult-onset still disease. Medicine (Baltimore) 2002;81:194-200. Back to cited text no. 71 |
| 72. | Goldman JA, Beard MR, Casey HL. Acute febrile juvenile rheumatoid arthritis in adults: cause of polyarthritis and fever. South Med J 1980;73:555-63. Back to cited text no. 72 |
| 73. | Bjorkengren AG, Pathria MN, Sartoris DJ, Terkeltaub R, Esdaile JM, Weisman M, et al. Carpal alterations in adult-onset Still disease, juvenile chronic arthritis, and adult-onset rheumatoid arthritis: Comparative study. Radiology 1987;165:545-8. Back to cited text no. 73 |
| 74. | Appenzeller S, Castro GR, Costallat LT, Samara AM, Bertolo MB. Adult-onset Still disease in southeast Brazil. J Clin Rheumatol 2005;11:76-80. Back to cited text no. 74 |
| 75. | Reginato AJ, Schumacher HR Jr, Baker DG, O'Connor CR, Ferreiros J. Adult onset Still's disease: Experience in 23 patients and literature review with emphasis on organ failure. Semin Arthritis Rheum 1987;17:39-57. Back to cited text no. 75 |
| 76. | Valente RM, Banks PM, Conn DL. Characterization of lymph node histology in adult onset Still's disease. J Rheumatol 1989;16: 349-54. Back to cited text no. 76 |
| 77. | Quaini F, Manganelli P, Pileri S, Magnani G, Ferrari C, Delsignore R, et al. Immunohistological characterization of lymph nodes in two cases of adult onset Still's disease. J Rheumatol 1991;18:1418-23. Back to cited text no. 77 |
| 78. | Kojima M, Nakamura S, Miyawaki S, Yashiro K, Oyama T, Itoh H, et al. Lymph node lesion in adult-onset Still's disease resembling peripheral T-cell lymphoma: A report of three cases. Int J Surg Pathol 2002;10:197-202. Back to cited text no. 78 |
| 79. | Reichert LJ, Keuning JJ, van Beek M, van Rijthoven AW. Lymph node histology simulating T-cell lymphoma in adult-onset Still's disease. Ann Hematol 1992;65:53-4. Back to cited text no. 79 |
| 80. | Uppal SS, Al-Mutairi M, Hayat S, Abraham M, Malaviya A. Ten years of clinical experience with adult onset Still's disease: Is the outcome improving? Clin Rheumatol 2007;26:1055-60. Back to cited text no. 80 |
| 81. | Owlia MB, Soleimani H, Mortazavizadeh M. Macrophage activation syndrome (MAS) and Thrombotic Thrombocytopenia Purpura (TTP): Are they from a single spectrum? J Indian Acad Community Med 2005;6:337-40. Back to cited text no. 81 |
| 82. | Tristano AG. Macrophage activation syndrome: A frequent but under-diagnosed complication associated with rheumatic diseases. Med Sci Monit 2008;14:RA27-36. Back to cited text no. 82 |
| 83. | Arlet JB, Le TH, Marinho A, Amoura Z, Wechsler B, Papo T, et al. Reactive haemophagocytic syndrome in adult-onset Still's disease: A report of six patients and a review of the literature. Ann Rheum Dis 2006;65:1596-601. Back to cited text no. 83 |
| 84. | Grom AA. Macrophage activation syndrome and reactive hemophagocytic lymphohistiocytosis: The same entities? Curr Opin Rheumatol 2003;15:587-90. Back to cited text no. 84 |
| 85. | Park JH, Bae JH, Choi YS, Lee HS, Jun JB, Jung S, et al. Adult-onset Still's disease with disseminated intravascular coagulation and multiple organ dysfunctions dramatically treated with cyclosporine A. J Korean Med Sci 2004;19:137-41. Back to cited text no. 85 |
| 86. | Sanada I, Kawano F, Tsukamoto A, Kiyokawa T, Shido T, Koga S. Disseminated intravascular coagulation in a case of adult onset Still's disease. Rinsho Ketsueki 1997;38:1194-8. Back to cited text no. 86 |
| 87. | Yokoyama M, Suwa A, Shinozawa T, Fujii T, Mimori T, Akizuki M, et al. A case of adult onset Still's disease complicated with adult respiratory distress syndrome and disseminated intravascular coagulation. Nihon Rinsho Meneki Gakkai Kaishi 1995;18:207-14. Back to cited text no. 87 |
| 88. | Arai Y, Handa T, Mitani K. Adult-onset Still disease presenting with disseminated intravascular coagulation. Rinsho Ketsueki 2004;45:316-8. Back to cited text no. 88 |
| 89. | Owlia MB, Soleimani H, HajiGhasemian S. Adult-onset Still's Disease presenting first in pregnancy (case report). J Shahid Sadoughi Univ Med Sci 2003;11:67-70. Back to cited text no. 89 |
| 90. | Mok MY, Lo Y, Leung PY, Lau CS. Pregnancy outcome in patients with adult onset Still's disease. J Rheumatol 2004;31:2307-9. Back to cited text no. 90 |
| 91. | Le Loet X, Daragon A, Duval C, Thomine E, Lauret P, Humbert G. Adult onset Still's disease and pregnancy. J Rheumatol 1993;20:1158-61. Back to cited text no. 91 |
| 92. | Motoo Y, Ohta H, Okai T, Sawabu N. Adult-onset Still's disease: hepatic involvement and various serum markers relating to the disease activity. Jpn J Med 1991;30:247-50. Back to cited text no. 92 |
| 93. | Pamuk ON, Pamuk GE, Usta U, Cakir N. Hemophagocytic syndrome in one patient with adult-onset Still's disease: Presentation with febrile neutropenia. Clin Rheumatol 2007;26:797-800. Back to cited text no. 93 |
| 94. | ten Kate J, Drenth JP, Kahn MF, van Deursen C. Iron saturation of serum ferritin in patients with adult onset Still's disease. J Rheumatol 2001;28:2213-5. Back to cited text no. 94 |
| 95. | Fardet L, Coppo P, Kettaneh A, Dehoux M, Cabane J, Lambotte O. Low glycosylated ferritin: A good marker for the diagnosis of hemophagocytic syndrome. Arthritis Rheum 2008;58:1521-7. Back to cited text no. 95 |
| 96. | Van Reeth C, Le Moel G, Lasne Y, Revenant MC, Agneray J, Kahn MF, et al. Serum ferritin and isoferritins are tools for diagnosis of active adult Still's disease. J Rheumatol 1994;21:890-5. Back to cited text no. 96 |
| 97. | Fautrel B, Le Moel G, Saint-Marcoux B, Taupin P, Vignes S, Rozenberg S, et al. Diagnostic value of ferritin and glycosylated ferritin in adult onset Still's disease. J Rheumatol 2001;28:322-9. Back to cited text no. 97 |
| 98. | Vignes S, Le Moel G, Fautrel B, Wechsler B, Godeau P, Piette JC. Percentage of glycosylated serum ferritin remains low throughout the course of adult onset Still's disease. Ann Rheum Dis 2000;59:347-50. Back to cited text no. 98 |
| 99. | Hamidou MA, Denis M, Barbarot S, Boutoille D, Belizna C, Le Moel G. Usefulness of glycosylated ferritin in atypical presentations of adult onset Still's disease. Ann Rheum Dis 2004;63:605. Back to cited text no. 99 |
| 100. | Schwarz-Eywill M, Heilig B, Bauer H, Breitbart A, Pezzutto A. Evaluation of serum ferritin as a marker for adult Still's disease activity. Ann Rheum Dis 1992;51:683-5. Back to cited text no. 100 |
| 101. | Andres E, Kurtz JE, Perrin AE, Pflumio F, Ruellan A, Goichot B, et al. Retrospective monocentric study of 17 patients with adult Still's disease, with special focus on liver abnormalities. Hepatogastroenterology 2003;50:192-5. Back to cited text no. 101 |
| 102. | Dino O, Provenzano G, Giannuoli G, Sciarrino E, Pouyet M, Pagliaro L. Fulminant hepatic failure in adult onset Still's disease. J Rheumatol 1996;23:784-5. Back to cited text no. 102 |
| 103. | Ogata A, Kitano M, Yamanaka J, Yamasaki T, Hashimoto N, Iwasaki T, et al. Interleukin 18 and hepatocyte growth factor in fulminant hepatic failure of adult onset Still's disease. J Rheumatol 2003;30:1093-6. Back to cited text no. 103 |
| 104. | Medsger TA, Jr., Christy WC. Carpal arthritis with ankylosis in late onset Still's disease. Arthritis Rheum 1976;19:232-42. Back to cited text no. 104 |
| 105. | Masson C, Le Loet X, Liote F, Dubost JJ, Boissier MC, Perroux-Goumy L, et al. Comparative study of 6 types of criteria in adult Still's disease. J Rheumatol 1996;23:495-7. Back to cited text no. 105 |
| 106. | Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still's disease. J Rheumatol 1992;19:424-30. Back to cited text no. 106 |
| 107. | Kadar J, Petrovicz E. Adult-onset Still's disease. Best Pract Res Clin Rheumatol 2004;18:663-76. Back to cited text no. 107 |
| 108. | Chandran V, Aggarwal A. Adult-Onset Still's Disease. J Indian Rheumatol Assoc 2002;10:19-21. Back to cited text no. 108 |
| 109. | van de Putte LB, Wouters JM. Adult-onset Still's disease. Baillieres Clin Rheumatol 1991;5:263-75. Back to cited text no. 109 |
| 110. | Koizumi R, Tsukada Y, Ideura H, Ueki K, Maezawa A, Nojima Y. Treatment of adult Still's disease with dexamethasone, an alternative to prednisolone. Scand J Rheumatol 2000;29:396-8. Back to cited text no. 110 |
| 111. | Khraishi M, Fam AG. Treatment of fulminant adult Still's disease with intravenous pulse methylprednisolone therapy. J Rheumatol 1991;18:1088-90. Back to cited text no. 111 |
| 112. | Fautrel B. Adult-onset Still disease. Best Pract Res Clin Rheumatol 2008;22:773-92. Back to cited text no. 112 |
| 113. | Kraetsch HG, Antoni C, Kalden JR, Manger B. Successful treatment of a small cohort of patients with adult onset of Still's disease with infliximab: first experiences. Ann Rheum Dis 2001;60:iii55-7. Back to cited text no. 113 |
| 114. | Jung JH, Jun JB, Yoo DH, Kim TH, Jung SS, Lee IH, et al. High toxicity of sulfasalazine in adult-onset Still's disease. Clin Exp Rheumatol 2000;18:245-8. Back to cited text no. 114 |
| 115. | Okamoto O, Oishi M, Fujiwara S. Steroid-resistant adult-onset Still's disease which showed a quick response to methotrexate. J Dermatol 2008;35:106-10. Back to cited text no. 115 |
| 116. | Espinosa G, Cervera R. Role of biologic therapy in systemic autoimmune diseases.. Med Clin (Barc) 2007;128:456-7. Back to cited text no. 116 |
| 117. | Efthimiou P, Kontzias A, Ward CM, Ogden NS. Adult-onset Still's disease: can recent advances in our understanding of its pathogenesis lead to targeted therapy? Nat Clin Pract Rheumatol 2007;3:328-35. Back to cited text no. 117 |
| 118. | Furst DE, Breedveld FC, Kalden JR, Smolen JS, Burmester GR, Sieper J, et al. Updated consensus statement on biological agents for the treatment of rheumatic diseases, 2007. Ann Rheum Dis 2007;66:iii2-22. Back to cited text no. 118 |
| 119. | Cavagna L, Caporali R, Epis O, Bobbio-Pallavicini F, Montecucco C. Infliximab in the treatment of adult Still's disease refractory to conventional therapy. Clin Exp Rheumatol 2001;19:329-32. Back to cited text no. 119 |
| 120. | Kokkinos A, Iliopoulos A, Greka P, Efthymiou A, Katsilambros N, Sfikakis PP. Successful treatment of refractory adult-onset Still's disease with infliximab. A prospective, non-comparative series of four patients. Clin Rheumatol 2004;23:45-9. Back to cited text no. 120 |
| 121. | Olivieri I, de Stefano G, Padula A, La Gala A, de Stefano C. Infliximab in a case of early adult-onset Still's disease. Clin Rheumatol 2003;22:369-70. Back to cited text no. 121 |
| 122. | Thonhofer R, Soleiman A, Kriessmayr M, Thonhofer U, Wipfler E, Gaugg M, et al. Decrease of proteinuria in a patient with adult-onset Still's disease and glomerulonephritis after anti-TNFalpha therapy. Scand J Rheumatol 2006;35:485-8. Back to cited text no. 122 |
| 123. | Benucci M, Li GF, Del Rosso A, Manfredi M. Adalimumab (anti-TNF-alpha) therapy to improve the clinical course of adult-onset Still's disease: the first case report. Clin Exp Rheumatol 2005;23:733. Back to cited text no. 123 |
| 124. | Husni ME, Maier AL, Mease PJ, Overman SS, Fraser P, Gravallese EM, et al. Etanercept in the treatment of adult patients with Still's disease. Arthritis Rheum 2002;46:1171-6. Back to cited text no. 124 |
| 125. | Kuek A, Weerakoon A, Ahmed K, Ostor AJ. Adult-onset Still's disease and myocarditis: Successful treatment with intravenous immunoglobulin and maintenance of remission with etanercept. Rheumatology (Oxford) 2007;46:1043-4. Back to cited text no. 125 |
| 126. | Asherson RA, Pascoe L. Adult onset Still's disease: response to Enbrel. Ann Rheum Dis 2002;61:859-60;author reply 60. Back to cited text no. 126 |
| 127. | Serratrice J, Granel B, Disdier P, Weiller PJ, Dussol B. Resolution with etanercept of nephrotic syndrome due to renal AA amyloidosis in adult Still's disease. Am J Med 2003;115:589-90. Back to cited text no. 127 |
| 128. | Yang DH, Chang DM, Lai JH, Kuo SY, Ho TY, Lin KM, et al. Etanercept as a rescue agent in patient with adult onset Still's disease complicated with congestive heart failure. Rheumatol Int 2008. Back to cited text no. 128 |
| 129. | Murakami K, Fujii T, Yukawa N, Yoshifuji H, Kawabata D, Tanaka M, et al. Successful treatment of a patient with refractory adult Still's disease by tacrolimus. Mod Rheumatol 2007;17:167-70. Back to cited text no. 129 |
| 130. | Fitzgerald AA, Leclercq SA, Yan A, Homik JE, Dinarello CA. Rapid responses to anakinra in patients with refractory adult-onset Still's disease. Arthritis Rheum 2005;52:1794-803. Back to cited text no. 130 |
| 131. | Vasques Godinho FM, Parreira Santos MJ, Canas da Silva J. Refractory adult onset Still's disease successfully treated with anakinra. Ann Rheum Dis 2005;64:647-8. Back to cited text no. 131 |
| 132. | Kotter I, Wacker A, Koch S, Henes J, Richter C, Engel A, et al. Anakinra in patients with treatment-resistant adult-onset Still's disease: four case reports with serial cytokine measurements and a review of the literature. Semin Arthritis Rheum 2007;37:189-97. Back to cited text no. 132 |
| 133. | Mylona E, Golfinopoulou S, Samarkos M, Fanourgiakis P, Papadakos V, Skoutelis A. Acute hepatitis in adult Still's disease during corticosteroid treatment successfully treated with anakinra. Clin Rheumatol 2008;27:659-61. Back to cited text no. 133 |
| 134. | Ito T, Ozaki Y, Shimamoto K, Amuro H, Tanijiri T, Yokoi T, et al. Successful treatment with plasma exchange in adult-onset Still's disease with hyper-IL-18-naemia and hyperallergic state. Mod Rheumatol 2008;18:407-10. Back to cited text no. 134 |
| 135. | Kato T, Kobayashi T, Nishino H, Hidaka Y. Double-filtration plasmapheresis for resolution of corticosteroid resistant adult onset Still's disease. Clin Rheumatol 2006;25:579-82. Back to cited text no. 135 |
| 136. | Vignes S, Wechsler B. Still's disease in adults: treatment with intravenous immunoglobulins. Rev Med Interne 1999;20:419s-22s. Back to cited text no. 136 |
| 137. | Mahmud T, Hughes GR. Intravenous immunoglobulin in the treatment of refractory adult Still's disease. J Rheumatol 1999;26: 2067-8. Back to cited text no. 137 |
| 138. | Liozon E, Ly K, Aubard Y, Vidal E. Intravenous immunoglobulins for adult Still's disease and pregnancy. Rheumatology (Oxford) 1999;38:1024-5. Back to cited text no. 138 |
| 139. | Ahmadi-Simab K, Lamprecht P, Jankowiak C, Gross WL. Successful treatment of refractory adult onset Still's disease with rituximab. Ann Rheum Dis 2006;65:1117-8. Back to cited text no. 139 |
| 140. | Pirildar T. Treatment of adult-onset Still's disease with leflunomide and chloroquine combination in two patients. Clin Rheumatol 2003;22:157. Back to cited text no. 140 |
| 141. | Cefle A. Leflunomide and azathioprine combination in refractory adult-onset Still's disease. Ann Pharmacother 2005;39:764-7. Back to cited text no. 141 |
| 142. | Sayarlioglu M, Ucmak H, Ozkaya M, Ucar MA, Sayarlioglu H. Leflunomide and methotrexate combination in refractory adult-onset Still's disease. Ann Pharmacother 2007;41:1319-20. Back to cited text no. 142 |
| 143. | Nakahara H, Mima T, Yoshio-Hoshino N, Matsushita M, Hashimoto J, Nishimoto N. A case report of a patient with refractory adult-onset Still's disease who was successfully treated with tocilizumab over 6 years. Mod Rheumatol 2008 2. Back to cited text no. 143 |
Copyright 2009 - Indian Journal of Medical Sciences
The following images related to this document are available:
Photo images
[ms09041t1.jpg]
[ms09041t2.jpg]
|

{kind=link}
{kind=link}