 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
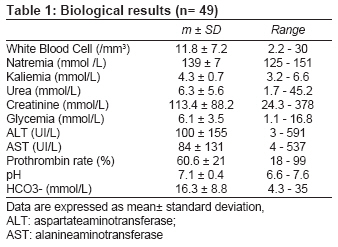
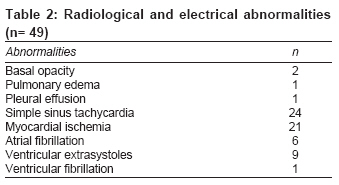
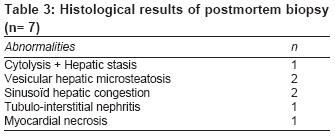
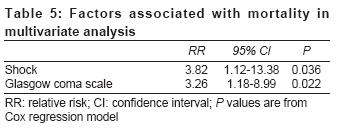
Indian Journal of Medical Sciences, Vol. 63, No. 6, June, 2009, pp. 227-234 Original Article Prognostic factors of acute aluminum phosphide poisoning Louriz M, Dendane T, Abidi K, Madani N, Abouqal R, Zeggwagh AA Medical ICU, Ibn Sina Hospital, Rabat Code Number: ms09042 PMID: 19602756 Abstract Background : In Morocco, acute aluminum phosphide poisoning (AAlPP) is a serious health care problem. It results in high mortality rate despite the progress of critical care.Aims : The present paper aims at determining the characteristics of AAlPP and evaluating its severity factors. Setting and design: We studied consecutive patients of AAlPP admitted to the medical intensive care unit (ICU) (Ibn Sina Hospital, Rabat, Morocco) between January 1992 and December 2007. Materials and Methods : Around 50 parameters were collected, and a comparison was made between survivor and nonsurvivor groups. Statistical Analysis : Data were analyzed using Fisher exact test, Mann-Whitney U test and Cox regression model. Results : Forty-nine patients were enrolled: 31 females and 18 males; their average age was 26± 11 years. The ingested dose of aluminum phosphide was 1.2± 0.7 g. Self-poisoning was observed in 47 cases, and the median of delay before admission to the hospital was 5.3 hours (range, 2.9-10 hours). Glasgow coma scale was 14± 2. Shock was reported in 42.6% of the patients. pH was 7.1± 0.4, and bicarbonate concentration was 16.3± 8.8 mmol/L. Electrocardiogram abnormalities were noted in 28 (57%) cases. The mortality rate was 49% (24 cases). The prognostic factors were APACHE II (P= 0.01), low Glasgow coma scale (P= 0.022), shock (P= 0.0003), electrocardiogram abnormalities (P= 0.015), acute renal failure (P= 0.026), low prothrombin rate (P= 0.020), hyperleukocytosis (P= 0.004), use of vasoactive drugs (P< 0.001), use of mechanical ventilation (P= 0.003). Multivariate analysis by logistic regression revealed that mortality in AAlPP correlated with shock (RR = 3.82; 95% CI= 1.12-13.38; P= 0.036) and altered consciousness (RR= 3.26; 95% CI= 1.18-8.99; P= 0.022). Conclusion : AAlPP is responsible for a high mortality, which is primarily due to hemodynamic failure. Keywords: Acute poisoning, aluminum phosphide, prognosis Introduction Aluminum phosphide is used in Morocco as a fumigant to control rodents and pests in grain-storage facilities. [1] The trade name of the fumigant is Phostoxin ® , and it comes in the form of dark gray tablets of 3 g each, consisting of aluminum phosphide (56%) and aluminum carbamate (44%). Aluminum phosphide is highly toxic, low cost and easily accessible. This explains why it is the main cause of poisoning in developing countries. Patients who intend to commit suicide take tablets. Once mixed with aqueous solutions in the stomach, phosphine gas (PH 3 ) is immediately released and absorbed rapidly via the lungs causing systemic poisoning and cell hypoxia as an outcome of the oxidative phosphorylation inhibition. [2],[3],[4] Acute aluminum phosphide poisoning (AAlPP) is responsible for oxidative stress due to induction of free radicals and catalase inhibition by PH 3 . [5] This gas, which is a very toxic systemic poison, makes AAlPP extremely dangerous, especially because antidote is not available. Symptoms of AAlPP appear within the first few hours following exposure. AAlPP is a real medical emergency demanding early and adequate management. In spite of the progress achieved in the fields of toxicology and associated therapy, AAlPP is still responsible for a high rate of mortality. [1],[2] The objectives of this study were to evaluate the characteristics and the prognostic factors of AAlPP in our context.Materials and Methods We conducted a retrospective study in the medical ICU (Universitary Hospital Ibn Sina, Rabat, Morocco) between January 1992 and December 2007. Rabat University Hospital is a referral for the inhabitants in northwestern Morocco. The 12-bed medical ICU admits approximately 550 patients annually. The staff within the unit consists of 6 seniors (physicians that have a working experience of more than 2 years in ICUs) and 6 juniors (physicians that have a working experience of less than 2 years in ICUs). We performed this study by referring to the medical ICU admission register entries between 1992 and 2007. We included all patients whose diagnosis upon admission and/ or discharge was AAlPP. We studied all medical files, collected data on working card, performed data capture on SPSS software and, finally, did statistical analysis, which was performed by 1 senior physician. All other stages were performed by 2 junior physicians. We considered patients that presented with anamnesis of AAlPP and fulfilled clinical and toxicological criteria of AAlPP. We conducted silver nitrate test to identify aluminum phosphide: silver nitrate-impregnated strips immersed in a sample of gastric fluid for 20 minutes darken in the presence of PH 3 . We excluded cases of chronic poisoning by aluminum phosphide and those of poisoning related to other pesticides and rodenticides from our study (total, 487 cases). For each patient, the following characteristics were recorded: age, gender, deliberate or accidental poisoning, previous suicide attempts, time between poisoning and admission to the ICU, APACHE II score, clinical characteristics (abdominal pain, vomiting, Glasgow coma scale, systolic blood pressure, central venous pressure), biological characteristics (silver nitrate test, cells blood count, crasis, serum electrolytes, glycemia, renal function, liver enzymes, arterial blood gas), abnormalities of chest x-ray and electrocardiogram, treatment characteristics. APACHE II score and all biologic variables were checked several times during the first 24 hours on admission to the ICU, and we kept pejorative results. In our unit, the management of AAlPP is supportive only because there is no specific antidote. Gastric lavage was performed for all patients, approximately 2 hours after admission to the emergency room before ICU admission. Activated charcoal was not available in our unit. Magnesium sulfate, a membrane stabilizer that can reverse arrhythmia, was used only if available. When monitoring of vital signs showed hypotension or shock, we administered intravenous fluids according to the central venous pressure, which can be combined with dopamine or dobutamine infusion to maintain systolic blood pressure above 80 mm Hg. Oxygen was given immediately with the monitoring of clinical respiratory effects of AAlPP, pulse oximetry and arterial blood gas; if respiratory distress was present, we used mechanical ventilation. Alkalinization was used if severe metabolic acidosis was present. We also recorded length of stay in the ICU, mortality rate and results of the postmortem biopsy. Postmortem examination was carried out for the first few cases of AAIPP (occurring in the early 1990s) for forensic and scientific reasons - in order to understand the toxicity mechanism of the aluminum phosphide especially with scarce literature on the subject. Percutaneous biopsy was performed for collecting samples from the liver, the heart and kidneys. We inserted a hollow needle into the organs to remove 3 small pieces of tissue of each organ. The samples were sent to a pathology laboratory of our hospital, where the tissue was stained to identify signs of diseases. The quantitative variables were presented in terms of mean± standard deviation, and qualitative variables were presented in terms of total number and percentage. Statistical analysis was performed using "statistical package for the social sciences" (SPSS) software. Comparisons between ′good outcome′ and ′poor outcome′ groups were made by Mann-Whitney U test for quantitative data and Fisher exact test for categorical data. P values of less than 0.05 were considered to indicate statistical significance. A multivariate logistic regression analysis was performed to identify factors independently associated with mortality. Only variables with a strong association with poor outcome in univariate analysis (P< 0.05) were included in the Cox regression model.Results Forty-nine patients (31 females, 18 males) were registered from the 1145 patients of poisoning admitted to the ICU during the same period. Their age was 26± 11 years. Forty-seven cases were of voluntary poisoning, and 2 were of accidental poisoning. The ingested dose was 1.2± 0.7 g [range, 1.5-12 g]. Previous suicide attempts using other products were found in 2 patients. APACHE II score was 5.6± 5.9. The time between ingestion and admission to the medical ICU was 9.1± 10.7 hours. Abdominal pain was found in 50% of the cases; and vomiting, in 71.4%. Glasgow coma scale (GCS) was 14± 2 [range, 8-15]. Systolic blood pressure was 85.5± 40 mm Hg, and central venous pressure was 18± 5.5 cm H 2 O. The main biological results are presented in [Table - 1]. The electrocardiogram was abnormal in 28 (58.7%) patients. The radiological and electrical anomalies are reported in [Table - 2]. The results of silver nitrate test using gastric fluid were positive in all patients. Volemic expansion used isotonic saline serum in 45% of patients (n= 32) and colloid in 14.2% of the patients. Alkalinization was used in 1 patient with pH at 6.6, and 9 (18.4%) patients received magnesium sulfate. Twenty-six (53.1%) patients required vasoactive drugs, and 20 (40%) patients needed mechanical ventilation. The mortality rate was 49% (24 patients). Death occurred after 64± 47 hours from the time of admission, corresponding to 72± 58 hours from the time of ingestion. The postmortem biopsy was realized in 7 patients [Table - 3]. Length of stay was 60± 70 hours [range, 1-120 hours]. The risk factors predicting mortality in AAlPP in univariate analysis are reported in [Table - 4]. Multivariate analysis revealed that mortality in AAlPP correlated with shock (RR = 3.82; 95% CI= 1.12-13.38; P= 0.036) and altered consciousness (RR= 3.26; 95% CI= 1.18-8.99; P= .022) [Table - 5]. Discussion Forty-nine patients were enrolled in this study. The ingested dose of aluminum phosphide was 1.2± 0.7 g. Self-poisoning was observed in 47 cases, and the median of delay before admission to the hospital was 5.3 hours. The prognostic factors were APACHE II score, low Glasgow coma scale, shock, electrocardiogram abnormalities, acute renal failure, low prothrombin rate, hyperleukocytosis, use of vasoactive drugs, use of mechanical ventilation. Multivariate analysis revealed that mortality in AAlPP correlated with shock and altered consciousness. In Morocco, AAlPP cases were first reported at the end of 1980. [5] AAlPP is a serious public health problem and a real challenge for medical professionals in developing countries, mainly in the northern parts of India, where this intoxication increased from 35% in 1977 to 77% in 1997 with a decrease in the number of cases of accidental origin from 63% to 17% in the same period. [6],[7],[8],[9],[10],[11],[12],[13],[14],[15] Indeed, AAlPP is mainly voluntary, as revealed in our study (96% of patients). Survival is unlikely if more than 1.5 g is ingested. [14] The age of patients varies between 10 and 55 years, with high rate between 20 and 30 years, as described in our study. [11],[16] The main complications observed in the course of fatal AAlPP are cardiac dysrhythmias, severe metabolic acidosis, shock, respiratory distress syndrome and hypomagnesemia. [12],[17],[18],[19],[20],[21],[22] Several severity factors are described in the literature, such as age, lack of vomiting, severe acidosis, hypotension, hyperglycemia and ingestion of high dose of aluminum phosphide. [2],[3],[14],[21],[23] In our study, these factors were not found to influence significantly the mortality rate, especially hyperglycemia. The correlation of hyperglycemia with mortality described by some authors suggests that its management may have a useful role in treatment of AAlPP by allowing increased entrance of glucose into cells and reducing oxygen consumption. [23] Other factors such as shock, electrical abnormalities and respiratory failure have been reported in different studies and in our study as well. [2],[12],[21],[24] In addition, we found that altered consciousness, acute renal failure, impaired hemostasis and hyperleukocytosis were other risk factors for mortality. All these effects of AAlPP could be explained by the pathologic action of phosphine, which involves inhibition of cytochrome oxydase and free radical damage of tissues. The organs with the greatest oxygen requirement appear to be especially sensitive to damage; these include the brain, heart, kidneys and liver. Dysmagnesemia following AAlPP has been described, though its pathogenesis is not clear. [17],[19] In our cases, the serum concentration of magnesium was not checked. In our study, the multivariate analysis revealed that mortality in AAlPP correlated with shock and altered consciousness. A number of researchers reported that the frequency of hypotension and shock varied from 76% to 100%. [20,[24] The mechanism of shock is not clear. Clinical, biological and electrical observations suggest that myocardial lesion is responsible for hemodynamic failure. [13],[25] In our study, shock associated with high central venous pressure suggests a cardiac mechanism, although the volemic expansion did not cause pulmonary edema. Echocardiography exploration in AAlPP revealed reversible diffuse myocardial injury with left ventricle hypokinesia. [26],[27] This was confirmed in our study by autopsy, which revealed a myocardial necrosis. On the other hand, the hypovolemia induced by vomiting could contribute to hypotension. Several studies noted electric abnormalities in 36% to 91% of cases. [8],[24] These are conduction disorders such as right and left bundle branch block (25%), atrioventricular block (8%) and, rarely, sinoatrial block. [8] On the other hand, cardiac dysrhythmias were described as atrial fibrillation (4% to 61%), junctional rhythm (4% to 100%), ventricular and atrial extrasystoles and ventricular tachycardia. [2] Finally, re-polarization disorders were also reported, such as ST segment depression (12% to 65%), ST segment elevation (4% to 65%) and T wave inversion (36%). [13] These 4 types of electric abnormalities were observed in our study with variable frequency. The administration of magnesium sulfate might prevent these disorders. [18],[19],[21] Several studies reported neurological toxicity of aluminum phosphide resulting in clinical effects like headache, stupor, restlessness, agitation, anxiety, ataxia, paresthesia and central nervous system depression leading to coma and seizures. [28],[29],[30] In our study, we investigated microscopic changes in vital organs of the body, liver, heart and kidneys [Table - 3]. These changes were found to be suggestive of cellular hypoxia. Other recent studies with more patients were performed and showed congestion, edema and leukocytis infiltration in the liver, kidneys, heart, stomach, lung, brain and adrenals. [31],[32] AAlPP is characterized by high mortality, which exceeds 60% and can reach 100%. [1],[2],[12],[14],[16],[24],[25] In our study, mortality rate was less (49%). We explain this result by 2 hypotheses. First, the ingested dose was less (1.2± 0.7 g) - survival is unlikely if more than 1.5 g is ingested; [14] and the second hypothesis is related to vomiting, which was found in 71.4% of our patients - lack of vomiting is a severity factor described in several studies. [2],[3],[14],[21] Most deaths occurred after 60 hours or more, and we can attribute that, perhaps, to early administration of vasoactive drugs and supportive treatment for AAlPP and to less severity of our cases. Conclusion AAlPP is responsible for a high mortality, which is primarily due to hemodynamic failure. In our study, mortality in AAlPP correlated with shock and altered consciousness. Because of unavailability of a specific antidote, early and adequate management of heart failure could improve prognosis. Therefore, it is recommended that efforts be made to prevent AAlPP and to set strict rules for its use ans sales.References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09042t1.jpg] [ms09042t4.jpg] [ms09042t3.jpg] [ms09042t2.jpg] [ms09042t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}