 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
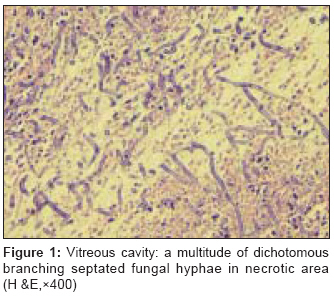
Indian Journal of Medical Sciences, Vol. 63, No. 6, June, 2009, pp. 253-256 Case Report Aspergillus endophthalmitis in orthotopic liver transplantation Hosseini Hamid, Saki Soraya, Saki Nasrin, Eghtedari Masoomeh Research Center of Shiraz University of Medical Sciences, Shiraz Code Number: ms09045 PMID: 19602759 Abstract In this report, we describe a patient with drug-induced liver failure who developed endogenous endophthalmitis after liver transplantation. Our patient's clinical course was so fulminant that the eye was lost in less than 1 month, without any response to therapy. Recognition of this infection is important because many patients die of disseminated Aspergillus infection, which may be detected early with bedside funduscopic examination by an ophthalmologist. Probably if the patient had referred to us earlier, it may have been possible to save the eye.Keywords: Aspergillus endophthalmitis, orthotopic liver transplant Introduction Aspergillus endophthalmitis (AE) is a rare invasive form of aspergillosis and can occur as exogenous and endogenous infection. The former is a complication of ocular penetrating injury or surgery, whereas the latter has been generally reported as associated with intravenous drug abuse, solid organ transplants and cancer. [1],[2],[3] Our report presents a fulminant course of this infection in an adult after orthotopic liver transplant. Despite treatment, which generally includes pars plana vitrectomy (PPV), intravitreal amphotericin B, systemic amphotericin B and oral antifungal agents, the visual prognosis remains grave, and the risk of mortality is high. [4],[5] Case Report A 22-year-old man with allogenic orthotopic liver transplantation due to drug-induced liver failure (sodium valporate) referred to the ophthalmology emergency clinic. The patient complained of decreased visual acuity in his left eye of 3 days′ duration about 3 weeks after liver transplantation. He was on immunosuppressive medications (azathioprine and mycophenolate mofetil [MMF]). He did not have any ocular problem before the operation. Best-corrected visual acuity was 20/20 in right eye; and in the left eye, there was detection of hand-motion only. Intraocular pressure was 12 mm Hg in both eyes. Slit-lamp examination of the left eye revealed mild conjunctival hyperemia, 2+ to 3+ cells in anterior chamber, clear lens and vitreous inflammation (intense cellularity and whitish debris). Ophthalmoscopy through the dilated pupil showed moderate vitreous haze with diffuse retinal edema and multifocal large (several disc diameter area) subretinal mass-like lesions. Due to hazy vitreous, the lesions could not be evaluated well, so ocular sonography was requested. In ocular sonography, posterior segment wall thickening, partial retinal detachment and choroidal detachment were detected The right eye revealed no abnormalities. These findings were suggestive of a unilateral endogenous endophthalmitis, especially fungal endophthalmitis; therefore, systemic workup for infection was done. Intravenous therapy with amphotericin B (conventional) 0.7 mg/kg/day, Imipenem and vancomycin was started according to clinical diagnosis. Pars plana core vitrectomy was performed. Undiluted samples from vitreous and aqueous were used for pathogen identification. An intravitreal injection of amphotericin (50µg/mL), vancomycin (10 mg/mL) and ceftazidime (20 mg/mL) were administered. Topical amphotericin and atropine were started. KOH smear showed fungal hyphae. Samples from anterior chamber and vitreous were sent for aerobic and anaerobic bacterial and fungal cultures. While aqueous humor yielded no growth, vitreous specimen was positive for Aspergillus. Blood and urine samples were culture negative. Chest x-ray was normal. No systemic findings, such as fever, skin lesions, neurological abnormalities, in favor of invasive aspergillosis were detected. Erythrocyte sedimentation rate was normal. Complete blood count was normal except for thrombocytopenia. In the first postoperative week, no improvement was observed. So intravenous amphotericin was changed to IV voriconazole (6 mg/kg 2 doses 12 hours apart, followed by maintenance dose of 4 mg/kg every 12 hours), and intravitreal voriconazole (1000 µg/mL) was injected. In the following week, visual acuity of his left eye did not improve but declined to light perception. Another intravitreal injection of voriconazole was administered 6 days after the first one. Conjunctival congestion and anterior chamber reaction decreased, but the vitreous demonstrated increased opacity. Two weeks later, the left eye became painful and vision decreased to no light perception. A cataract developed in the lens, anterior chamber became shallow, and yellowish dense vitreous opacity was seen behind the lens. Also corneal edema was seen. Ultrasonography showed total retinal detachment. To remove this possible source of continuous infection, the eye was eviscerated and subjected to histopathologic examination. Macroscopically, prominent yellowish exudates occupied vitreous cavity. During operation, no sclera involvement was detected. Histopathologic findings demonstrated granulomatous reaction with severe necrosis in vitreous cavity and multinucleated giant cell. A multitude of dichotomous branching septated fungal hyphae in necrotic area were also detected [Figure - 1]. Sphere ball was implanted, and the patient was followed up with full examination of the other eye. No involvement of the other eye was detected after 1 year follow-up. Discussion In this report, we describe a patient with drug-induced liver failure who developed endogenous endophthalmitis after liver transplantation. In the literature, Aspergillus endophthalmitis is described as a fulminant and devastating process. [1],[2],[3] Aspergillus endophthalmitis has been reported following antibiotic administration, surgical procedures; in parenteral drug abusers and in patients with malignancy (lymphoma and leukemia). [1],[2],[3],[4],[7],[8],[9] However, the main risk group comprises of individuals that have received immunosuppressive agents and transplant recipients. [6],[7] Our patient received immunosuppressive medications (MMF and azathioprine), and that was an important risk factor for aspergillosis. [6],[7] Clinically the infection often begins in the posterior part of the eye as the hyphae invade the retina and the choroids, leading to choroidoretinitis. The invasion of small blood vessels can cause hemorrhages and necrosis of the retina, followed by a breakthrough into the vitreous, leading to blurred and impaired vision. The anterior segment of the eye is often deceptively quiet, although pain, photophobia and iridocyclitis can occur. [8] Diagnostic and therapeutic pars plana vitrectomy is indicated in these patients. Despite the approval of new antifungal agents, a vast majority of patients with endogenous Aspergillus endophthalmitis are still treated with intravenous or intravitreous amphotericin B. Because of the side effects and the poor penetration into aqueous humor and vitreous, therapy with intraocular injections with or without vitrectomy is more preferable in cases of endophthalmitis. [9] Voriconazole demonstrates potent activity against a broad spectrum of yeasts and molds. Studies have shown that voriconazole is more active than amphotericin B against filamentous fungi such as Aspergillus species and is currently the treatment of choice for invasive aspergillosis. It is available for IV administration or as an oral preparation, both of which demonstrate high bioavailability, with good penetration into the cerebrospinal fluid and eye. [10],[11],[12] Treatment of endogenous Aspergillus endophthalmitis with voriconazole has only been reported by Kramer et al. - in a case of Aspergillus terreus in a lung transplant patient, with some improved outcome. [10] Few publications have reported encouraging results of the treatment of other ocular fungal diseases with this new triazole. [13] In the present case of Aspergillus endophthalmitis, amphotericin was used, at first, intravenously and then intravitreal; and when no clinical improvement was observed, IV amphotericin was changed to voriconazole. Voriconazole was also injected into the vitreous, but no improvement was detected; his eye became blind, and evisceration was done, finally. To conclude, our patient′s clinical course was so fulminant that the eye was lost in less than 1 month, without any response to therapy. Aspergillus endophthalmitis is almost always disseminated from elsewhere in the body, often the lung. One limitation of our case is the lack of a high-resolution CT or MRI, as a normal chest x-ray may not exclude invasive pulmonary aspergillosis. Recognition of this infection is important because many patients die of disseminated Aspergillus infection, which may be detected early with bedside funduscopic examination by an ophthalmologist. Probably if the patient had referred to us earlier, it may have been possible to save the eye. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09045f1.jpg] |
| |||||||||

{kind=link}