 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
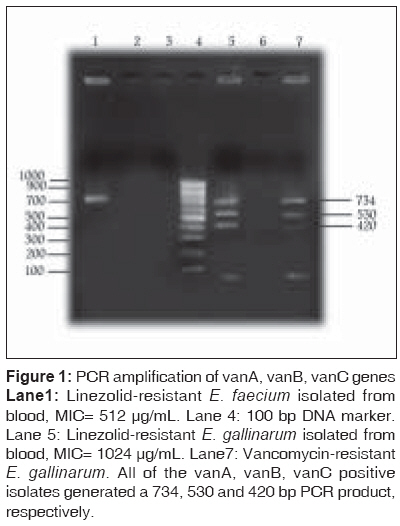
Indian Journal of Medical Sciences, Vol. 63, No. 7, July, 2009, pp. 297-302 Original Article Linezolid vancomycin resistant Enterococcus isolated from clinical samples in Tehran hospitals Yasliani S, Mobarez AMohabati, Doust RHosseini, Satari M, Teymornejad O Department of Bacteriology, Faculty of Medical Sciences, Tarbiat Modares University, Tehran Code Number: ms09053 PMID: 19700910 Abstract Background: Vancomycin-resistant enterococci pose an emerging health risk. The limitation in therapeutic options has resulted in the development of new drugs such as quinupristin/ dalfopristin and linezolid.Aim, Setting and Design: This study investigated the species prevalence and antibacterial resistance among enterococci isolated in selected Tehran hospitals. Materials and Methods: Between March 2006 and August 2007, 200 enterococcal isolates from urine, blood, stool and wound were recovered in 2 teaching hospitals of Tehran province. Susceptibility of all isolates was tested against vancomycin, teicoplanin and linezolid antibiotics by disk diffusion and agar dilution method. Results and Conclusion: Seventeen (8.5%), 6 (3%) and 4 (2%) of the isolates were resistant to vancomycin, teicoplanin and linezolid, respectively. Within the vancomycin-resistant isolates, 6 (35.2%), 4 (25%) and 1 (5.88%) showed vanA, vanB and vanC genotype patterns, respectively. Four (23.5%) of VRE isolates were resistant to linezolid with minimum inhibitory concentrations between 16 and 32 µg/mL. Two linezolid vancomycin resistant enterococci were E. faecium. Keywords: Linezolid vancomycin resistant Enterococcus, vanA, B, C gene, vancomycin resistant Enterococcus Introduction Vancomycin resistant enterococci (VRE) are the main sources of infections in humans and carry the transferable vancomycin resistance markers. [1] This organism has been reported as the second leading cause of urinary tract infections and the third leading cause of nosocomial bacteremia in hospitalized patients. Bacteremia due to VRE is a significant complication in surgical patients and is associated with mortality rates ranging from 33% to 68%. [2] Linezolid has been used successfully alone and in combination with gentamicin in treating VRE bacteremia. [3],[4] Linezolid belongs to the class of oxazolidinones, a new antimicrobials with a unique mechanism of action. They are active against gram-positive organisms, including VRE and methicillin resistant Staphylococcus aureus (MRSA), with a primarily bacteriostatic mode of action. [3],[5] In vitro resistance to linezolid is mediated via mutations in the central region of domain V of 23SrRNA and/ or by as yet unknown mechanisms. [6],[7] However, resistance in wild-type isolates of Enterococcus and Staphylococcus is conferred by a single nucleotide transvertion at position 2576 in 23SrRNA. Linezolid has been used in clinical practice for a relatively short period of time; there are already several reports of linezolid-resistant enterococci. [8],[9],[10] In this study we compared the in vitro activity of linezolid with that of vancomycin and teicoplanin against 200 enterococci isolates. To our knowledge, this is the first report of linezolid vancomycin resistant Enterococcus strains isolated in selected Tehran hospitals. Materials and Methods A total of 200 isolates were obtained from different clinical samples between 2006 and 2007 in 2 teaching hospitals in Tehran, Iran. The isolates were cultured from blood, urine, wound and stool. The isolates were identified to the genus and species level by culture characteristic, Gram′s stain, catalase test, bile esculin, sorbitol, raffinose, arabinose, motility, pigmentation and SH2 tests. Antimicrobial susceptibility testing Disk diffusion method on Muller-Hinton agar [11] was used to detect resistance to vancomycin (30 µg) and teicoplanin (30 µg). Break point zone diameter for vancomycin was ≤10 mm (≥16 µg/mL); and for linezolid ≤17 mm (≥16 µg/mL), for resistance. Results were read after incubation at 35°C for 24 hours. MICs for vancomycin and linezolid were determined by the agar dilution method. Enterococcus faecalis strain ATCC 29212 was used as a control for susceptibility testing. Detection of vancomycin - resistance determinants by PCR The presence of the vanA, B and C resistance genes was assessed by PCR using specific primers described by Khan et al.[11] The primers were vanA Forward- 5′-AAT ACT GTT TGG GGG TTG CTC-3′ and vanA Reverse- 5′-CTT TTT CCG GCT CGA CTT CCT-3′; vanB forward- 5-GGG GGG A GG ATG GTG GGA TAGAG-3 and vanB Reverse- 5-GGA AGATACCGT GGC TCA AAC-3; vanC Forward- 5-TTG ACC CGC TGA AAT ATG AAGTAA-3 and vanC Reverse- 5-TAG AAC CGT AAG CAA AAG CAG TGG-3. The amplification mixture consisted of 5 µL of 10 x PCR buffer (100 mM Tris / HCl, pH 8.4 500 mM KCl; 20 mM MgCl 2 ), 220 µM each dNTP, 22 U mL -1 recombinant Taq DNA polymerase, 5 µL bacterial DNA and 5 µL primer, 6 µL H2O. An Ependroff thermocycler was programmed for 30 cycles with the following parameters: denaturation at 97°C for 1 minute, annealing at 52°C for 55 seconds, extension at 72°C for 1.5 minutes and final extension at 72°C for 10 minutes. Amplified products were detected by agarose gel electrophoresis using 1.5% agarose (w/v) in TAE buffer for 2 hours at 70 V. E. faecium ATCC 51559, E. faecalis ATCC 51299 and E. gallinarum ATCC 49573 (kindly provided by Dr M. Feyzabady) were used for standardizing the PCR amplification of vanA, vanB, vanC. Vancomycin-sensitive strain, E. faecalis ATCC 29212, was used as the negative control in the PCR experiments. Results Susceptibility to antimicrobial agents A total of 200 enterococcal isolates were obtained from different clinical samples in 2 teaching hospitals in Tehran. The majority of them were obtained from urine [95 (47.5%)], followed by blood [63 (31.5%)] and wound swabs [42 (21%)]. The isolates were identified as E. faecalis (80%), E. faecium (11%), E. casseliflavous (6.5%), E. gallinarum (2%) and E. avium (0.5%). High level of resistance to vancomycin (MIC> 64 µg/mL) was detected in 17 (8.5%) of the isolates. In addition, 6 (3%) and 4 (2%) of the isolates were resistant to teicoplanin and linezolid, respectively [Table - 1]. The linezolid minimum inhibitory concentrations for linezolid vancomycin resistant enterococci isolates were between 16 and 32 µg/mL [Table - 2]. Two (50%), 1 (25%) and 1 (25%) of the VLRE isolates were E. faecium, E. gallinarum and E. casseliflavous, respectively. All of linezolid vancomycin resistant enterococci were isolated from blood samples. Detection of van genotype in vancomycin resistant (VRE) and linezolid vancomycin resistant Enterococcus. The 17 vancomycin resistant enterococci (VRE) and 4 linezolid vancomycin resistant enterococci were investigated for their van genotypes by PCR. VanA, B and C were detected in 6 (35.2%), 4 (23.5%) and 1 (5.88%) VRE isolates, respectively. All of the linezolid vancomycin resistant enterococci (VLRE) gave positive results for the presence of the vanA or vanB genotype [Figure - 1]. Discussion In the present study, we determined the species prevalence, vancomycin and linezolid susceptibility of clinical enterococcal isolates from 2 teaching hospitals in Tehran. The majority of the isolates were either E. faecalis (80%) or E. faecium (11%), while E. casseliflavus, E. gallinarum and E. avium accounted for only 9% of the isolates, which was comparable to the distribution of enterococcal species in other studies. [13],[14] Although we found 8.5%, 3% and 2% of isolates were resistant to vancomycin, teicoplanin and linezolid, respectively, diverse patterns of enterococci resistance have been reported from many countries. [13],[14],[15] In vitro resistance to linezolid is mediated via mutations in the central region of domain V of 23SrRNA and/ or by as yet unknown mechanisms. [6],[7] However, resistance in wild-type isolates of Enterococcus and Staphylococcus is conferred by a single nucleotide transvertion at position 2576 in 23SrRNA. Isolates for which the MICs are more than 8 mg/L are defined as resistant. [18] In this study, 4 out of 17 VRE isolates were also resistant to linezolid that was recovered from blood samples. This is the first report of a linezolid-resistant enterococci (VLRE) strain in Tehran hospitals. Two of the isolates were E. faecium and 1 was E. gallinarum. The MIC of linezolid for the resistant isolates was between 16 and 32 µg /mL in each case, where the susceptibility break point for linezolid was less than 4 µg/mL. It is useful to identify the VRE isolates and also the vanA and vanB distributions by means of genotype. This linezolid vancomycin resistance has been classified as vanA, vanB, vanC cross resistance to teicoplanin. All linezolid resistant isolates were positive for vanA genes, and 2 of them were found to have vanB genotype by PCR. VLRE isolates were found to have MICs between 16 and 32 mg/L. The emergence of linezolid vancomycin resistant enterococci (VLRE) in blood samples is a dangerous fact. Additional concern is the risk of nosocomial spread of linezolid resistant organisms. Aukland et al.[19] recommended susceptibility testing of clinically significant gram-positive pathogens before starting linezolid therapy so as to shorten the course of linezolid treatment. Worldwide surveillance programs should closely monitor all linezolid resistance reports in order to trace any trend in the development of resistance. Acknowledgment We would like to thank the medical personnel at the laboratories of Baghyatollah and Sharyaty hospitals. We would also like to thank Tarbiat Modares University for providing grant for this research. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09053t2.jpg] [ms09053t1.jpg] [ms09053f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}