 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
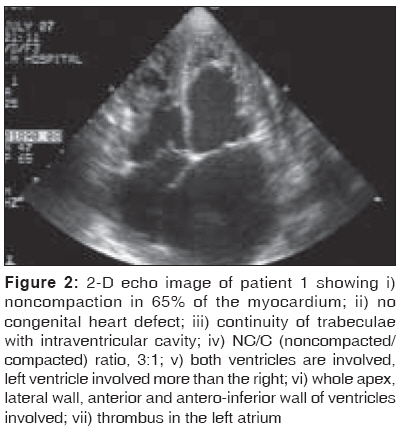
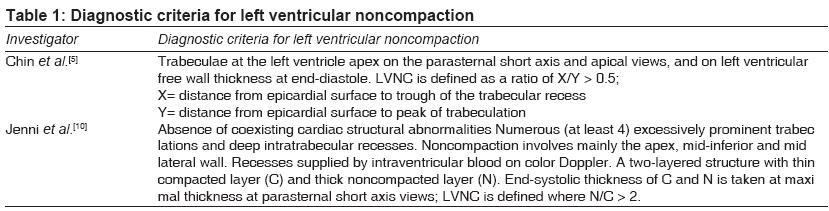
Indian Journal of Medical Sciences, Vol. 63, No. 7, July, 2009, pp. 303-307 Case Report Left ventricular noncompaction: A cardiomyopathy often mistaken Suvarna JyotiC, Deshmukh ChandrahasT, Hajela ShaliniA Department of Pediatrics, Seth GS Medical College and KEM Hospital, Mumbai Code Number: ms09054 PMID: 19700911 Abstract Left ventricular noncompaction (LVNC) is a rare genetic cardiomyopathy postulated to be a defect in endomyocardial morphogenesis due to the embryonic arrest of the compaction of myocardial fibers. It could be isolated, without other structural heart defects; or associated with congenital heart defects. It is characterized by prominent ventricular myocardial trabeculations and deep intertrabecular recesses. The clinical manifestations, i.e., heart failure, arrhythmias or thromboembolism, overlap with those of other cardiac disorders. It is often misdiagnosed as restrictive or dilated cardiomyopathy. The high mortality and morbidity associated with it and familial occurrence make diagnosis important. Only 3 pediatric cases have been reported from India. We present 2 cases, that of an 11-year-old girl (familial case) with embolism (documented but rare in children) and atrial flutter (not yet reported), with mother having asymptomatic LVNC; and that of a 4-month-old girl. Both presented with heart failure. The 11-year-old child had sudden death, known to occur in LVNC.Keywords: Arrhythmias, cardiomyopathy, embolism, heart failure, myocardium, noncompaction Introduction Left ventricular noncompaction (LVNC) is a cardiomyopathy due to a disorder in endomyocardial morphogenesis, seen either isolated (in the absence of other cardiac anomalies) or in association with congenital heart disease. It is postulated to be due to the intrauterine arrest of the compaction of myocardial fibers. [1] Initially categorized as unclassified cardiomyopathy (WHO, 1995), it is now categorized as a genetic cardiomyopathy (2006 classification of cardiomyopathies). [2] It is characterized by prominent trabeculations in the left ventricle and deep intertrabecular recesses; the later communicate with the ventricular cavity but not with the epicardial coronary artery system. [3] Right ventricular noncompaction may be associated in < 50% of the cases (seen in case 1). [4],[5] LVNC is misdiagnosed and missed in 89% of the cases. [3] Proper diagnosis requires an aware, experienced echocardiologist. To date only 3 pediatric cases of LVNC are reported from India. We describe 2 cases, that of an 11-year-old girl (familial case) with systemic embolism (rare in children) and atrial flutter (not yet reported) and that of a 4-month-old girl. Case Reports Case 1 An 11-year-old girl born of nonconsanguineous marriage, presented with dyspnea at rest, chest pain of 6 months′ duration, fever of 10 days′ duration, painful right calf swelling with blackish discoloration of 1 days′ duration. Past history and family history were uneventful. On examination, the child had irregularly irregular pulse, cold, dusky extremities, raised jugular venous pulse, no dysmorphic features and normal CNS examination. Cardiovascular examination revealed left ventricular hypertrophy, gallop rhythm and grade 4/6 pansystolic murmur in mitral area. The child had hepatosplenomegaly, basal crepitations (lungs), right calf erythema, discoloration, prolonged capillary refill, impalpable anterior, posterior tibial artery and signs of deep vein thrombosis. Chest roentgenogram showed cardiomegaly; electrocardiogram showed atrial flutter and left ventricular hypertrophy. Echocardiography demonstrated biventricular noncompaction (left ventricle>right ventricle) with sinusoids and deep recesses involving the whole ventricular apex; antero-inferior, anterolateral wall; and distal inter-ventricular septum - with biventricular systolic dysfunction, bi-atrial enlargement, moderate-to-severe mitral regurgitation, evidence of left atrial clot and ejection fraction of 30%. The sinusoids communicated with the ventricles but not the coronary system. Right limb arterial Doppler showed right common, external iliac thrombosis, monophasic flow in circumflex, superficial femoral artery, popliteal artery and no flow in anterior, posterior tibial arteries [Figure - 1],[Figure - 2]. Anti-streptolysin-O antibody throat culture: negative; ESR- 6 mm; CRP- 62 mg/L (normal, up to 5); PR interval- normal; serum cholesterol- 168 mg/dL (normal); triglyceride- 82 (normal); LDL- 138.9 mg/dL (normal, up to 130); HDL- 28 mg/dL (normal); anticardiolipin antibody IgG- 3.5 GPLU/mL (normal), IgM- 8 MPLU/mL (normal); Anti-nuclear antibody, anti-double stranded DNA antibody: negative. Cardiac MRI reported cardiomyopathy. Echocardiography of family showed LVNC in mother. The patient required inotropic support, decongestive therapy (digoxin, frusemide), anticoagulation therapy (heparin, warfarin) and captopril. Her condition improved, dyspnea improved, fever subsided and she underwent amputation but had sudden death 2 months after admission. Case 2 A 4-month-old girl born of nonconsanguineous marriage presented with complaints of feed refusal, forehead sweating of 3 weeks′ duration and breathlessness of 4 days′ duration. On examination the child had congestive cardiac failure, cardiomegaly, basal crepitations (lungs), hepatomegaly, no arrhythmias, no dysmorphic features and normal CNS examination. Chest roentgenogram showed cardiomegaly, and electrocardiogram revealed normal rhythm and left ventricular and atrial enlargement. Echocardiography confirmed noncompaction of left ventricle with severely compromised left ventricular systolic function (ejection fraction, 15%-20%). She was treated with inotropes, decongestive therapy, captopril and put on anticoagulants on follow-up due to persistent low ejection fraction. Discussion LVNC, first described by Chin et al., [5] has a male preponderance (56% to 82%). [5],[6],[7],[8] Female preponderance has been reported in Arabs/Africans. (Both our patients were female.) The 2 standard criteria for diagnosis [Table - 1] are complementary. [1] Although transthoracic echocardiography is the mainstay of diagnosis, other modalities include MRI (may identify arrhythmia substrate), contrast ventriculography and computed tomography. The clinical manifestations are heart failure, arrhythmias and embolic events. Adults have severe manifestations and higher mortality in comparison to children, who may be asymptomatic with variable presentations. [6] Both our patients presented with heart failure (seen in 67% of the cases). [8] Arrhythmia, rarer in children than in adults, [6] manifests as ventricular tachyarrhythmia (47% of adults), [5] atrial fibrillation (25% of adults), [5] left bundle branch block (44% of adults), [8] paroxysmal supra-ventricular tachycardia, [6],[7] complete heart block [6],[7] and Wolf Parkinson White syndrome (15% of children). Patient 1 had atrial flutter, which has not yet been reported in literature. Both subendocardial hypoperfusion and microcirculatory dysfunction contribute to the left ventricular dysfunction and arrhythmogenesis. [3] Subendocardial ischemia occurs due to the isometric contraction of endocardium and myocardium within the intratrabecular recesses. [3] The low ejection fraction, rhythm disturbances and the presence of blood in the deep intratrabecular recesses - all predispose to systemic embolism. [5],[7] Patient 1 had thromboembolism, which is documented but rare in children and seen in 21% to 38% of adults. [5],[6],[7],[8] Higher left ventricular end diastolic diameter, grade III-IV dyspnea, permanent/persistent atrial fibrillation, and bundle branch block increase the risk of mortality. [8] Our first patient, with grade IV dyspnea, atrial flutter, heart failure and thrombosis, was at high risk and died suddenly (seen in 50% of deaths in LVNC). [8] The treatment of LVNC consists of management of the clinical manifestations. Carvedilol (β-blocker) may have beneficial effects on left ventricular function, hypertrophy, metabolic and adrenergic abnormalities. [9] Long-term prophylactic anticoagulation is recommended for all patients, especially with severe noncompaction, embolic episodes or ejection fraction < 25%. [1],[5],[8] In high-risk patients (i.e., those with refractory heart failure, markedly reduced left ventricular function, prolonged intraventricular conduction), cardiac transplantation, implantable defibrillator or biventricular pacemakers have been tried. [7],[8] An association between LVNC and facial dysmorphism and neuromuscular disorders is reported. [6],[7] A familial occurrence in 18% to 51% of the cases, [3],[5],[6],[8] left ventricular dysfunction eventually in most [6] and death in 25% of the asymptomatic cases, make screening of family members mandatory. Our first patient′s mother had LVNC. Prognosis is better in incidental diagnosis of asymptomatic LVNC. [6] G4.5 gene mutations on Xq28 chromosome in pediatric LVNC; cardiac-specific gene CSX loss (distal chromosome 5q deletion), -dystrobrevin and Cypher/ZASP gene mutations in adults have been described. [1],[3],[4] Although capable of detecting in newborns and fetuses, antenatal fetal echocardiogram is reported to be unreliable. As many as 47% to 60% of adults die or undergo cardiac transplantation within 4 to 6 years, [7],[8] and most develop ventricular dysfunction over 10 years. [6] The high morbidity/ mortality and high chances of missing diagnosis would make the awareness of LVNC among physicians and cardiologists of prime importance.[10] References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09054f2.jpg] [ms09054f1.jpg] [ms09054t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}