 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
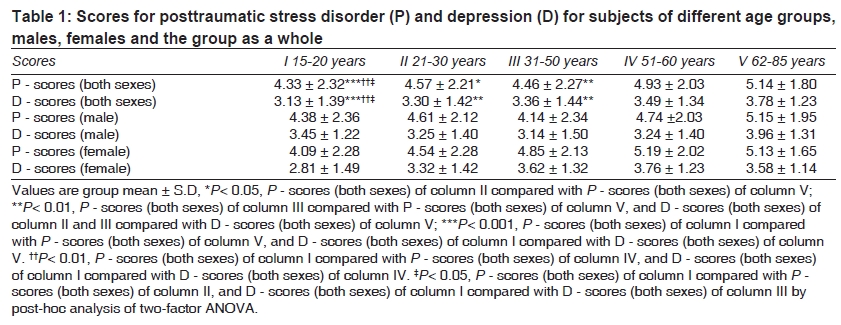
Indian Journal of Medical Sciences, Vol. 63, No. 8, August, 2009, pp. 330-334 Original Article Risk of posttraumatic stress disorder and depression in survivors of the floods in Bihar, India Telles Shirley, Singh Nilkamal, Joshi Meesha Department of Yoga Research and Development, Patanjali Yogpeeth, Haridwar Correspondence Address:Patanjali Yogpeeth, Maharishi Dayanand Gram, Near Bahadarabad, Haridwar - 249 402, Uttarakhand shirleytelles@gmail.com Code Number: ms09060 PMID: 19770523 DOI: 10.4103/0019-5359.55883 Abstract Background: Following a natural disaster, survivors are vulnerable to develop posttraumatic stress disorder (PTSD) and/ or depression. Objectives: (i) To screen survivors of the Bihar floods a month after the event to determine their scores in a screening questionnaire for PTSD and/ or depression and (ii) to correlate these scores with age and gender. Materials and Methods: One thousand two hundred eighty-nine persons (645 females) who had been directly exposed to the floods in Bihar, India, in August 2008 were assessed. The Screening Questionnaire for Disaster Mental Health (SQD) was used to screen for PTSD and depression. Statistical Analysis: Separate two-factor ANOVAs were used to compare persons of both sexes and 5 different age groups for PTSD and depression scores. This was followed by post-hoc analysis for multiple comparisons. Results: People over the age of 60 years had significantly higher scores for PTSD and depression compared to all groups (P< 0.05 for all comparisons). Conclusion: Following a natural disaster, older people appear more vulnerable to develop PTSD and depression. This should be taken into account in devising strategies for disaster relief. Keywords: Disasters, India, posttraumatic stress disorders Introduction In August 2008, heavy rains in the previous month led to a breach in the embankments of the Kosi River near the Indo-Nepal border. [1] The breach resulted in colossal loss of life and property in the north Indian state of Bihar, with over 2.5 million lives being affected. In India, following natural disasters like floods, there is unacceptably high morbidity and mortality amongst the affected population. [2] While there is a National Disaster Management Authority, each state is required to set up disaster management authorities and district disaster management committees, as well. This is important, as in the past, poor coordination at the local level has contributed to a poor response following disasters. [2] This can have psychological consequences, as occurrence of posttraumatic stress disorder (PTSD) among flood victims is significantly associated with social support. Social support is important, as it has been shown that after a natural disaster in India, groups like single women, children and men with negative coping behavior are the most vulnerable. [3] After the immediate needs are met and before survivors can return to their homes, there is often a period ranging from a few days to several months when large numbers of people are housed in temporary facilities. In such a situation, survivors require not only material relief but also psychological support to reduce the psychological trauma resulting from the event. [4],[5] There have been few attempts to screen Indian populations during this interim and stressful period. Children and adolescents were screened a year after a super-cyclone in the Indian state of Orissa, to find out the prevalence at one year and compare the effects in high- and low-exposure areas. [6] Quite obviously it was seen that significantly more children in high-exposure areas had PTSD compared to those in low-exposure areas. Also depression was significantly associated with PTSD. It was also seen that high exposure, lower educational levels and average socioeconomic status predicted the outcome of PTSD. The assessments were based on a semi-structured questionnaire for disaster-related experience, while diagnoses were based on the International Classification of Mental and Behavioral Disorders and the Diagnosis Criteria for Research. A more specific questionnaire has been developed, viz., the Screening Questionnaire for Disaster Mental Health, which screens for PTSD and depression. [7] This was used in Japan after the 1995 Great Hanshin earthquake and was shown to have good screening validity, especially for PTSD. The advantage of this questionnaire is that it reflects the characteristics of the aftermath of a large-scale disaster. This is particularly useful to understand mental health-related problems in those with scarce economical resources and whose lives are disrupted by the calamity. Hence the Screening Questionnaire for Disaster Mental Health (SQD) was administered to 1289 persons one month after the floods in Bihar, to screen the population to find those with high scores for PTSD and depression and to make comparisons across age groups and genders to determine which group had the highest scores. Materials and Methods Participants A total of 1289 persons, out of which 645 were females, who had been directly exposed to the floods in Bihar, India, on August 18, 2008, were assessed. The population consisted of lower-middle class persons (categorized based on their annual income), with less than 7 years of education. Most of them had completed their primary education and had started learning job-related skills due to economic constraints. Approximately 90% of the male participants were self employed (e.g., farmers and shopkeepers), and approximately 90% of the female participants were housewives. Their employment had been terminated and their income drastically reduced by the floods, as were their prospects of employment in the immediate future. The age range of the persons screened was wide, between 15 and 85 years (group mean age± S.D. was 34.1± 12.9 years), as the study aimed at determining the PTSD and depression scores of different age groups, using the screening tool. The SQD was translated into Hindi by a person with postgraduate degrees in both English and Hindi. The translation was also checked by a native speaker from Bihar. The persons administering the questionnaire attempted to cover as many individuals as possible by starting from one part of the camp and administering the questionnaire to all people over the age of 15 years. Most of the camp participants were in the camp as there was nowhere else for them to go. In case a particular family member was not present, the person was assessed later on. They were all staying in a temporarily erected flood relief camp in Bihar. The study was explained to the participants, and informed consent signed by them or their guardians was obtained. The study was approved by the institution's ethical committee. Design This was a cross-sectional study. The participants were categorized as 5 groups according to age, i.e., between (i) 15 and 20 years (n= 159), (ii) 21 and 30 years (n= 504), (iii) 31 and 50 years (n= 488), (iv) 51 and 60 years (n= 88) and (v) 61 and 85 years (n= 50). Assessment The Screening Questionnaire for Disaster Mental Health (SQD) was used to screen for symptoms of PTSD and depression in persons affected by the floods. The SQD consists of 12 close-ended questions which had two options as answers, viz., 'yes' and 'no.' The questions included 9 items for PTSD (SQD-P) and 6 items for depression (SQD-D). Questions numbered 3, 6 and 10 were common to both SQD-P and SQD-D. In this study, scores for PTSD (SQD-P) and for depression (SQD-D) were assessed. Data extraction Scoring of SQD was carried out according to the guidelines mentioned by the authors who developed the screening tool. [7] The scoring was done by a person who was not the same as the one who administered the SQD. The subscales on PTSD (9 items) were summed up to evaluate the possibility of being affected by PTSD; participants who scored between 6 and 9 were categorized as severely affected; between 4 and 5, as moderately affected; and between 0 and 3, as slightly affected. The subscales on depression (6 items) were also summed up to evaluate the possibility of having depression; participants who scored between 5 and 6 were categorized as more likely to be depressed; and those who scored between 0 and 4, as less likely to be depressed. Data analysis Data were analyzed using SPSS version 10.0. Two separate two-factor analyses of variance (ANOVAs) were performed for PTSD and depression scores. One factor was gender (with 3 levels, i.e., male, female and both male and female), and the other factor was age (with 5 levels). Post-hoc analyses for multiple comparisons were performed between people of different age groups and different genders, using the least significant difference test. Results The two-factor ANOVA showed a significant difference between different age groups for P (PTSD) scores (P< 0.001, df 4, 2563) and D (depression) scores (P= 0.001, df 4, 2563). In the post-hoc analyses, people over the age of 60 years had higher scores for PTSD than those with ages between (i) 15 and 20 years (P< 0.001; post-hoc analysis least significant difference LSD, 19% higher), (ii) 21 and 30 years (P= 0.014; post-hoc analysis LSD, 12% higher) and (iii) 31 and 50 years (P= 0.004; post-hoc analysis LSD, 15% higher). Those with ages between 51 and 60 years had higher PTSD scores than those with ages between (i) 15 and 20 years (P= 0.001; post-hoc analysis LSD, 14% higher), (ii) 21 and 30 years (P= 0.045; post-hoc analysis LSD, 8% higher) and (iii) 31 and 50 years (P= 0.010; post-hoc analysis LSD, 11% higher). Participants aged between 21 and 30 years also had higher PTSD scores than those between 15 and 20 years of age (P= 0.018; post-hoc analysis LSD, 6% higher). Also, persons over the age of 60 years had higher depression scores than those with ages between (i) 15 and 20 years (P< 0.001; post-hoc analysis LSD, 21% higher), (ii) 21 and 30 years (P= 0.001; post-hoc analysis LSD, 15% higher) and (iii) 31 and 50 years (P= 0.004; post-hoc analysis LSD, 13% higher). Those with ages between 31 and 50 years also had higher depression scores than those with ages between 15 and 20 years (P= 0.013; post-hoc analysis LSD, 7% higher). The PTSD and depression scores are given in [Table 1]. Discussion The present study assessed 1289 survivors of the floods in the north Indian state of Bihar for posttraumatic stress disorder (PTSD) and depression, one month after the event, while they were still located in temporary housing. Persons of both sexes aged over 60 years had higher scores for PTSD and depression compared to persons in other age groups. The Screening Questionnaire for Disaster Mental Health (SQD) has the following advantages: It can be administered by people with no specific experience in mental health; and the questions are designed so that self-reporting is easy, especially when dealing with older persons. [7] However, the reliability and validity for use in an Indian population have not been established. This did not seem to be especially important as none of the questions are culture-specific. However, the fact that the validity has not been established for an Indian population is a limiting factor of the study. The present study demonstrated the vulnerability of older persons. This group has already been shown to be vulnerable to developing mental health problems and difficulty in rebuilding their lives. [8] Also, the older population is recognized to be reluctant to seek local public health services, and hence particular effort is needed to reach out to this population. The floods in Bihar have occurred before in the same region and are, in a sense, a recurring cause for trauma. Hence the disaster response should involve (i) attempts to prevent the floods, where possible (as in this case, wherein there was a breach in the embankment of an adjoining river); and (ii) better preparedness in terms of basic necessities and medical and psychological assistance, particularly emphasizing the needs of older persons. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09060t1.jpg] |
| |||||||||

{kind=link}