 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
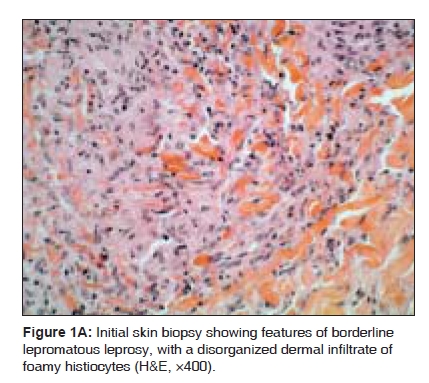
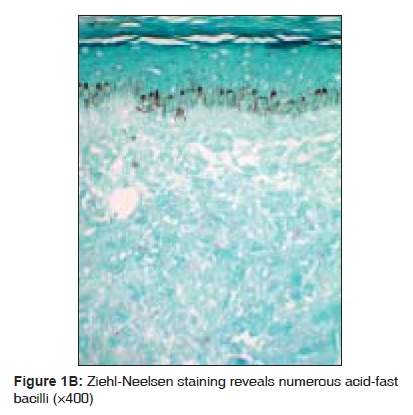
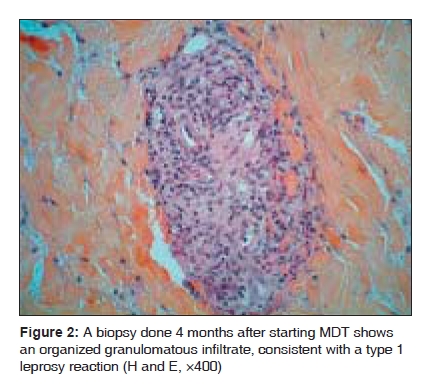
Indian Journal of Medical Sciences, Vol. 63, No. 8, August, 2009, pp. 359-362 Case Report Type 1 leprosy reversal reaction treated with topical tacrolimus along with systemic corticosteroids Safa Gilles, Darrieux Laure, Coic Alain, Tisseau Laurent Department of Dermatology, Centre Hospitalier de Saint-Brieuc, 22000 Saint-Brieuc Correspondence Address:Department of Dermatology, Centre Hospitalier de Saint-Brieuc, 22000 Saint-Brieuc gilles.safa@ch-stbrieuc.fr Code Number: ms09064 PMID: 19770527 DOI: 10.4103/0019-5359.55888 Abstract An 11-year-old black Haitian boy presented with borderline lepromatous leprosy and was treated with rifampicin, dapsone, and clofazimine. After 4 months he developed a severe type 1 reversal reaction without nerve involvement. He was started on prednisolone (1 mg/kg daily). After 4 weeks of treatment with corticosteroids, his condition did not improve and the lesions remained painful. The patient was given a therapeutic trial with twice daily application of topical tacrolimus 0.1% ointment. The result was a dramatic improvement in the skin lesions. The patient's condition was maintained by topical tacrolimus therapy, with healing of all skin lesions. The prednisolone dose was then tapered to zero over a period of 12 weeks. To the best of our knowledge, this is the first report of the efficacy of topical tacrolimus in the treatment of type 1 leprosy reaction.Keywords: Leprosy, tacrolimus, type 1 reaction Introduction Leprosy, which is caused by Mycobacterium leprae, is a chronic granulomatous infectious disease, primarily involving the skin and peripheral nerves. The clinical features can vary significantly, depending upon the patient's cell-mediated immune response to the organism. An increase in immunity, manifesting as a type 1 or reversal reaction, is common after treatment in patients with borderline lepromatous leprosy, and the disease then moves toward the tuberculoid pole. [1] Corticosteroids are the drugs of choice for treatment of type 1 leprosy reversal reactions. The failure of this treatment in one patient led us to try topical application of tacrolimus ointment. Case Report An 11-year-old black Haitian boy presented with bilateral, multiple non-anaesthetic hypopigmented macules on the arms, buttocks, and thighs, along with papules on the face. The peripheral nerves were not thickened and clinical examination showed a normal sensory and motor system. Histopathological examination of a thigh lesion showed an infiltrate below a subepidermal clear zone of foamy histiocytic cells admixed with few lymphocytes and occasional plasma cells. The infiltrate showed perineural accentuation. Ziehl-Neelsen stain showed numerous acid-fast bacilli within the histiocytes [Figure - 1A and B]. The bacterial index was 4+. A diagnosis of borderline lepromatous leprosy was made and the World Health Organization (WHO)-recommended multibacillary multidrug therapy (MDT) with rifampicin, dapsone, and clofazimine was started. Four months later, the patient presented with increases in size, erythema, and induration of the lesions; he also had new lesions on the face and limbs. Neither enlarged peripheral nerves nor sensory or motor neuropathies were detected. Biopsy from a new skin lesion revealed tuberculoid granulomatous inflammation involving the superficial and deep dermis, with only occasional acid-fast bacilli on Ziehl-Neelsen staining [Figure - 2]. He was diagnosed with type 1 leprosy reversal reaction and started on prednisolone (1 mg/kg daily). After 4 weeks of treatment with corticosteroids, his condition did not improve and the lesions remained painful [Figure - 3]. The patient was then given a therapeutic trial with twice daily application of topical tacrolimus 0.1% ointment. There was marked improvement of the lesions after 7 days of treatment and almost complete clearance of lesions after 2 weeks [Figure - 4A and B]. The reaction was thus controlled with topical tacrolimus and the dose of prednisolone was tapered to zero over a period of 12 weeks. Discussion Type 1 leprosy reversal reaction, which occurs in a third of patients With borderline leprosy, is an expression of delayed hypersensitivity.[2] The reactions usually occur early on during treatment with MDT but can continue to occur for 12 months and, occasionally, may even occur after MDT has been halted. [3] It is triggered by the interaction of CD4-positive T-helper lymphocytes with antigens released by M leprae. It is postulated that lysis of mycobacteria as a result of anti-leprosy therapy causes the release of antigens that promote an immune response. [4] Reversal reactions are associated with the infiltration of skin lesions and nerves by interferon-g and tumour necrosis factor-a-secreting CD4-positive lymphocytes, resulting in edema and painful inflammation. [5] Cytokine production by peripheral blood lymphocytes and serum cytokine concentrations are also increased during reversal reactions. The levels decrease with corticosteroid treatment, but patients with high cytokine responses have a poor clinical response to treatment and are more likely to relapse after withdrawal of corticosteroid therapy. [6],[7] Clinically, during these reactions there is increased erythema and induration of existing lesions as well as the development of new lesions. Severe neuritis, acral edema, and malaise may be seen. [8] Reversal reactions in leprosy must be considered a medical emergency that requires immediate treatment if permanent neurologic damage is to be prevented. Usually, type 1 leprosy reversal reactions are treated with corticosteroids. The failure of this regimen in our patient may have been due to high cytokine production in the skin lesions. Hence, the inhibition of the transcription and release of cytokines might explain, at least in part, the beneficial effect of tacrolimus ointment and the observed dramatic improvement in the skin lesions. Indeed, tacrolimus ointment has been used to treat a variety of inflammatory dermatoses. Tacrolimus is an immunomodulatory and immunosuppressant agent that inhibits T-cell activation by blocking the action of calcineurin; this results in inhibition of the transcription of several cytokine genes, with consequent decrease in the production of interleukin (IL)-2, IL-3, IL-4, IL-5, granulocyte-monocyte colony-stimulating factor, interferon-g, and tumour necrosis factor-a. [9] Interestingly, cyclosporin, another calcineurin inhibitor, has also been reported to be successful in the management of type 1 leprosy reactions when administered orally. [2],[10] Type 1 leprosy reactions are a major clinical management problem in leprosy. To the best of our knowledge, this is the first report of the use of topical tacrolimus in the treatment of a type 1 leprosy reaction. We think that it may be a new and promising adjunctive therapy for lesions that do not respond to corticosteroids. However, resource constraints limit the use of such expensive therapy in developing countries where leprosy remains a major public health issue. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09064f1b.jpg] [ms09064f4b.jpg] [ms09064f3.jpg] [ms09064f1a.jpg] [ms09064f4a.jpg] [ms09064f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}