 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
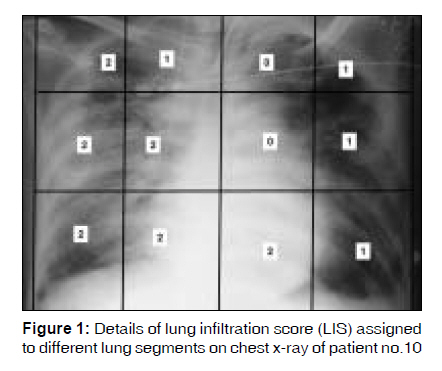
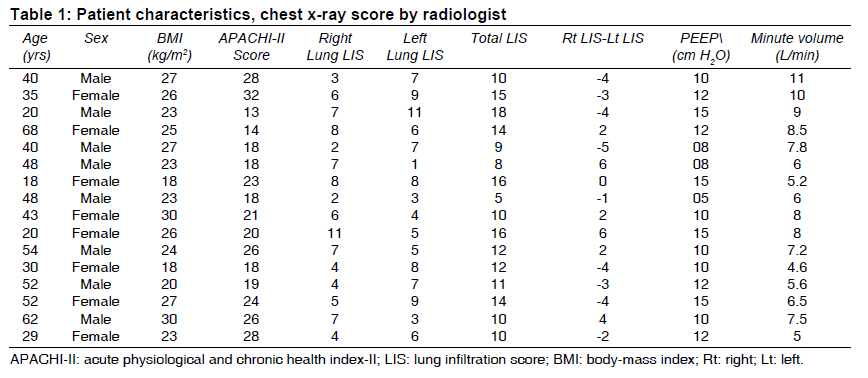
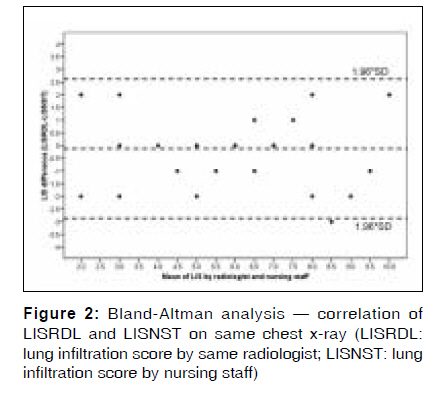
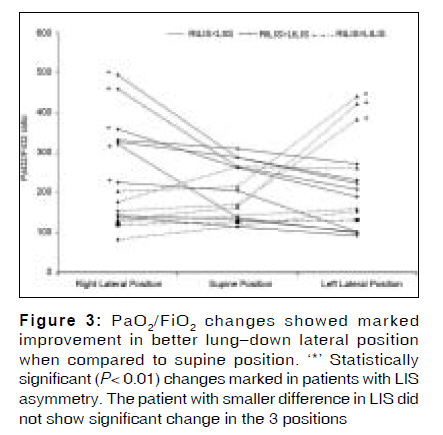
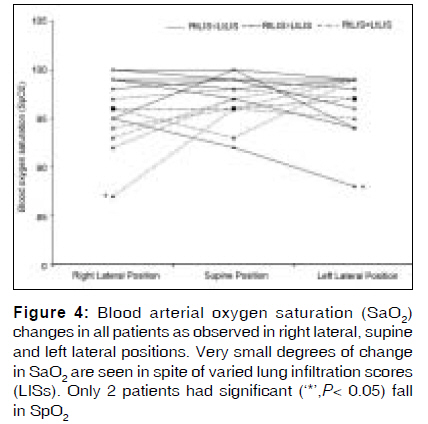
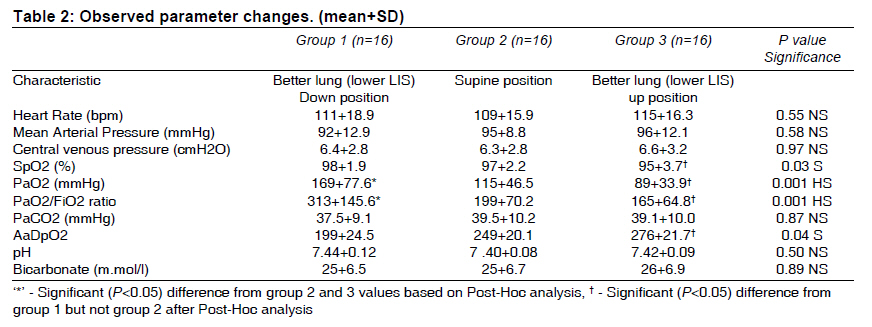
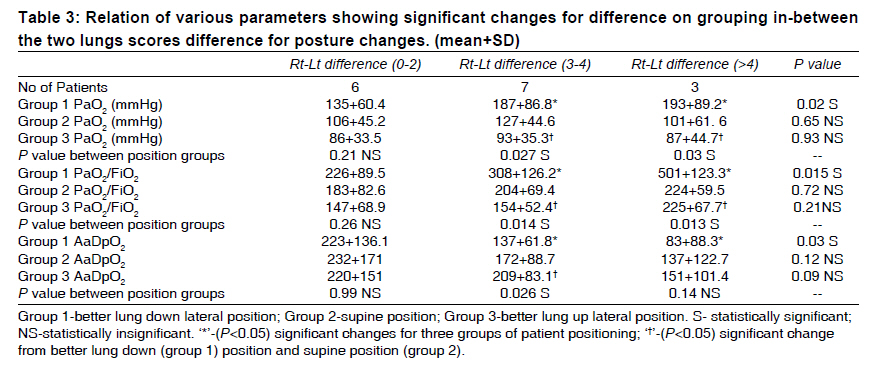
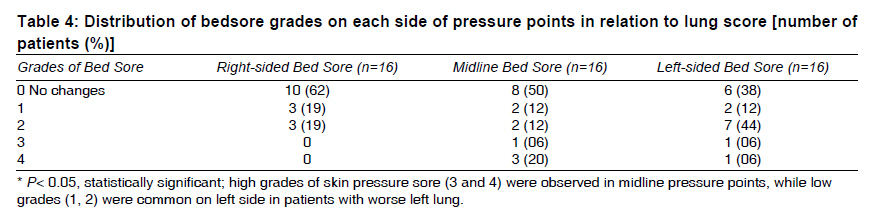
Indian Journal of Medical Sciences, Vol. 63, No. 9, September, 2009, pp. 392-401 Original Article Evaluation of lung infiltration score to predict postural hypoxemia in ventilated acute respiratory distress syndrome patients and the lateralization of skin pressure sore Mukesh Tripathi, Mamta Pandey, Bharat Nepal, Hari Rai, Balkrishna Bhattarai Department of Anaesthesiology and Critical Care, BPKIHS, Dharan, Nepal Correspondence Address: Prof. Mukesh Tripathi, C- 7.1.1, BPKIHS Campus, Dharan, Nepal Code Number: ms09072 PMID: 19805918 Abstract Context: Mechanical ventilation with positive end expiratory pressure (PEEP) is associated with unequal aeration of lungs in acute respiratory distress syndrome (ARDS) patients. Therefore, patients may develop asymmetric atelectasis and postural hypoxemia during lateral positioning. Keywords: Ayurvedic medication, d-Penicillamine, lead poisoning, peripheral neuropathy Introduction The cyclic positioning in mechanically ventilated patients is practiced to prevent pressure sores, improve oxygenation, mobilize secretions and decrease the incidence of ventilator-associated pneumonia. [1],[2],[3] Hypoxemia (decreased arterial blood oxygen level) is reported during lateral positioning of patients with unilateral lung disease. [4],[5],[6],[7] Acute respiratory distress syndrome (ARDS) is the most common pathology of respiratory failure in intensive care unit (ICU) requiring mechanical ventilation. The syndrome is characterized by refractory hypoxemia with bilateral diffuse infiltrates in lungs on chest x-ray. [8] Although radiographically and by definition, ARDS is a bilateral lung disease, blood oxygenation (PaO 2 ) in 5 of the 6 studied patients differed during lateral positioning, suggesting asymmetric lung involvement. [9] Since variable effects on oxygenation during lateral positioning of patients have been reported, [4],[10],[11],[12],[13] the effects of lateral positioning of ARDS patients are unclear. After extensive literature search, we did not find a method to quantify or predict the asymmetry of the lung disease. Therefore, we proposed a lung infiltration score (LIS) for the chest x-ray and evaluated it in predicting the risk of postural hypoxemia in ARDS patients. The problem of skin pressure sore has been widely discussed in the care of chronic patients but has become a point of concern in ICU, due to its far-reaching impact on cost of therapy and duration of hospital stay. [14],[15] Factors like older age, activity, immobilization, diminished pain sensation, moist skin, poor nutrition, friction and shear have been reported to predispose 68.4% of ICU patients for skin pressure sores (grade-2) within a week of ICU stay. [16] Thus a secondary area of the study was to look for lateralization of skin pressure sores, as tissue hypoxia might predispose towards bed sore formation. Materials and Methods We took approval from the institute's ethical committee and obtained informed written consent from the kin of every patient after explaining the nature of study. Patients who satisfied the following inclusion criteria for diagnosis of ARDS were admitted to the study: respiratory rate ≥30/min, chest x-ray with bilateral infiltrates, PaO 2 /FiO 2 < 150, [9] PaO 2 /FiO 2 < 200 with PEEP [17] and hypocarbia (PaCO 2 < 32 mm Hg). Since PaO 2 /FiO 2 ratio of < 200 is one of the ARDS criteria, for sample size calculation a 50% change in it was taken as a clinically significant difference. Assuming a standard deviation of 50, a-error of 0.05 and power (1-b) of 95%, 15 patients were desired to be studied on applying priori t test for two independent means. Thus prospective clinical study was performed on consecutive 16 adult (18-68 years of age) patients of both genders (8 male, 8 female) admitted to ICU in a 2-month period. They presented with ARDS of varied etiologies (abdominal sepsis- patient nos.1-3, 12-16; aspiration infiltrates- 6, 10; pneumonitis- 4, 5, 7; scorpion sting- 8, 9, 11). Patients were on mechanical ventilation with PEEP (5-12 cm H 2 O) for ≥24 hours to < 48 hours and had improvement in oxygenation (PaO 2 /Fi0 2≥ 200). Patients having hemodynamic instability and/ or on inotropes were excluded. Bedside chest x-ray (AP view) was taken on the day of study in expiratory phase after detaching ventilator. It was graded as follows: each lung field in the chest x-ray was divided into 3 zones on the basis of anterior shadow of ribs: upper zone- above the 2 nd rib; middle zone- from 2 nd to 4 th ribs; lower zone- from 4 th rib to dome of diaphragm. All 3 zones were further divided into medial and lateral halves, by the imaginary vertical line in between the midline (vertebral spines) and the tangential vertical line along the outer margin of the rib cage on both hemithoraces. Thus each lung was divided into 6 segments [Figure - 1]. On the basis of the radiolucency of the lung infiltrates in the chest x-ray, LIS points were assigned to each segment. LIS points scaled from 0 to 2 as follows: 0- normal alveolar picture; 1- patchy white infiltrates; 2- totally white infiltrates (radiolucency matching the heart shadow) [Figure - 1]. Only in the left medial lower zone, the scoring criteria were modified as LIS 0- normal heart shadow; 1- when bronchial web on heart shadow; and 2- radiolucency of infiltrate more than adjacent heart shadow with blurring of the heart border. Thus the maximum LIS that could be given was 12 for each lung and 24 for each patient. The LIS grading was done by the nursing staff (6 nurses scored 2 chest x-rays and 1 nurse scored 4 x-rays) attending to the patients. For validation, the same radiologist independently gave LIS points to all chest x-rays [Figure - 1]. Patients were monitored for changes in ECG lead II, arterial blood pressure, central venous pressure (CVP), arterial oxygen saturation by pulse oximetry (SpO 2 ), inhaled oxygen level (FiO 2 ), and arterial blood gas (ABG) parameters (pH, PaO 2 , PaCO 2 , HCO3 - , base deficit) during supine, left lateral by 45° tilt and right lateral by 45° tilt positions. The 3 positions were sequenced in random fashion by using sealed-envelope technique. The observer was kept blinded for the LISs of the chest x-rays. All the observations were noted after 20 minutes in each position. All patients were sedated and muscle relaxant was given to maintain identical ventilation settings during the study period. As a rescue measure, only FiO 2 was increased at any point of study in case SpO 2 dropped to a level < 90%. Data were sorted into 3 groups: group 1 (n= 16)- lateral position with better lung (lower LIS) down; group 2 (n= 16)- supine position and group 3 (n= 16)- lateral position with better lung up. We compared hemodynamic parameters, ABG and the calculated values of PaO 2 /FiO 2 , alveolar-arterial O 2 pressure difference (AaDpO 2 ) [(PB−47)ΧFi0 2−(paCO 2 /0.8)−PaO 2 ] in these 3 groups. Lung infiltrates asymmetry (right LIS−left LIS) was also calculated for each patient. Its positive value indicated that the right lung was more diseased than the left lung, and the negative value indicated that the left lung was more diseased than the right lung. We regrouped patients on the basis of LIS differences between the two lungs, i.e., LIS≤ 2 (n= 6); for 3 or 4 (n= 7); and ≥ 5 (n= 3) and compared oxygenation parameters to find out the significant lung infiltrates asymmetry related with the postural hypoxemia. The skin pressure sores were graded on 1 to 4 scale: stage 1- surface reddening of the skin like a bruise with intact skin; stage 2- blister, either broken or unbroken; stage 3- all the skin layers involved in wound; stage 4- wound involves the muscle, tendons and bones. [16] As per our ICU protocol, the cyclic change (4 hourly) of patient position from supine to right or left lateral was carried out in the subsequent days. The site and worst grades of pressure sores (sacrum, iliac crest and greater trochanter on both sides) were noted from the bedsore nursing chart in ICU in the next 1 week of the study period. Statistics All data were entered in statistical package SPSS-10.0 for windows (SPSS Inc., Chicago, IL). One-way analysis of variance (ANOVA) for descriptive data, nonparametric two-tailed Pearson's correlations coefficient, regression analysis of lung infiltrates asymmetry, Spearman's Rho and x 2 test were used. Calculated value of P < .05 at 95% confidence interval was considered statistically significant. The agreement between data pairs for the total LIS for each lung on chest x-ray given by the radiologist and nursing staff was analyzed by Bland and Altman analysis. Upper and lower limits of agreement, calculated as mean bias±1.96 SD of the difference between the LISs, were scored for each chest x-ray. Results The studied patients were 18 to 68 years of age, weighed 40 to 85 kg and had an APACHI-II score of 14 to 28 with a total LIS of 5 to 18. Patient no. 7 had bilaterally equal LIS with a total of 16, i.e., 8 for each side. Right LIS ≥ left LIS was found in 6 patients; and left LIS ≥ right LIS, in 9 patients. The difference in LIS for the two lungs ranged from −5 (left lung LIS ≥ right lung LIS) to +6 (right lung LIS ≥ left lung LIS) [Table - 1]. The scores given to bedside chest x-ray by the nursing staff and also independently assessed by a single radiologist showed a highly significant (P< 0.001) correlation (R= 0.86) for the total LIS of the two lungs. A Bland-Altman analysis of total LIS for the right and left lungs by radiologist and the nursing staff revealed a mean bias of −0.16. Limits of agreement were −2.93 and 2.61 to include 95% points within the range of LIS point differences between the radiologist and nursing staff [Figure - 2]. During the 3 position changes in the studied patients, PaO 2 /FiO 2 significantly (P< 0.01) improved in patients lying on their better lung than supine or lying on their bad lung. SpO 2 did not change significantly but for 2 patients, who developed desaturation lying on their bad lung, and the FiO 2 was increased [Figure - 3] and [Figure - 4]. Regrouping of the data on the basis of better lung-up or -down position, the oxygenation parameters (PaO 2 , 169± 77.6 mm Hg; PaO 2 /FiO 2 , 313± 145.6) in group 1 (better lung down) were significantly (P< 0.001) higher than those in group 2 (supine) or group 3 (better lung up) positions. The parameters (SpO 2 , PaO 2 , PaO 2 /FiO 2 and AaDpO 2 ) in supine position were found to be in between the two lateral positions. Other clinical parameters like heart rate, mean arterial pressure, CVP, PaCO 2 did not change significantly [Table - 2]. The arterial blood oxygenation parameters (PaO 2 , PaO 2 /FiO 2 and AaDpO 2 ) significantly (P< 0.05) changed during the 3 positions in patients with LIS difference ≥ 3. At LIS difference ≥4, PaO 2 /FiO 2 (501±123) was the highest and AaDpO 2 (83±88.3) was the lowest in better lung-down position. In patients with lesser difference between the two lungs (LIS≤ 2), the 3 parameters did not change significantly [Table - 3]. Out of the 16 studied patients, majority (9, 56%) of the patients had left lung worse than the right. Skin pressure sore grade 2 (skin redness, blisters) was more commonly (7, 44%) seen on left greater trochanter compared to the right side (3, 19%). Hence the incidence of left-sided skin pressure sore was also more, especially the higher skin pressure sore grades, viz., 3 or 4. The worst skin pressure sore (grade 4) developed on sacrum in midline in 3 (20%) patients; and in 1 (6%), on the left greater trochanter [Table - 4]. Discussion We observed that ARDS patients developed asymmetric lung infiltration after 24 hours of mechanical ventilation with PEEP (5-15 mm Hg). The proposed simple LISs of bedside chest x-rays determined by the attending nurses significantly correlated with those determined by the radiologists. Patients with asymmetric lung score (≥3) developed significant hypoxemia lying on the worse lung (higher LIS score) than when lying in the supine position or when lying on the better lung with an associated lateralization of the skin sores on the bony pressure points of the same side. Arterial blood-gas composition is determined by alveolar ventilation, pulmonary blood flow and on the basis of how ventilation is matched to blood flow in the lungs. [18] The lateral positioning with better lung down has long been recognized to give better arterial blood oxygenation than the better lung-up or the supine position in unilateral lung disease. [19] In ventilated, sedated and paralyzed patients, the alveolar ventilation of dependent worse lung remains poor due to its low compliance but there is preferential perfusion under gravity. [18],[20],[21] Thus the ventilation-perfusion mismatch adds to right-to-left shunt and reduced oxygenation in patients with unilateral lung disease. [22],[23] In ARDS patients, diffuse and bilateral infiltrates in chest x-ray still represent a patchy lung atelectasis due to varied grades of the lung's disease. [17] The mechanical ventilation with PEEP is frequently used to correct hypoxemia and improve lung function. [8] However, the aeration of alveoli by PEEP may not be uniform in different lung segments, being subject to severity of lung damage during insult. This process of patchy lung aeration in due course of therapy will predispose ARDS patients to postural hypoxemia. While studies [10],[11],[12] investigating the effects of lateral position in patients with bilateral lung infiltrates reported insignificant changes in oxygenation, PaO 2 values in supine position were not always between those in the two lateral positions. [4] Although asymmetry of the two-lung disease is not clear in these studies, we too did not find significant changes in oxygenation in patients of bilateral lung infiltrates till the LIS difference in the two lungs reached ≥3. It was noteworthy that the pulse oximetry did not change significantly, probably due to upper ceiling of 100% saturation, but PaO 2 improved significantly during better lung-down position. Since in this proposed LIS we took note of all the lung segments to map the differential lung changes, we could find PaO 2 , PaO 2 /FiO 2 and AaDpO 2 values for supine position to be in between those for the two lateral positions of the patients. Thus we could precisely map the differential lung involvement in bilateral lung disease and measure postural hypoxemia. Gillespie et al.[7] reported that in unilateral interstitial pulmonary disease, quantization of the ventilation-perfusion distribution did not show consistent differences between the patients in gas exchange. So besides improved ventilation-perfusion matching and decrease in right-to-left shunt, [7] other factors like PEEP diverting pulmonary blood away from 'normal lung' to affected lung zones, [24] hypoxemic vasoconstriction, [22] vessel obliteration and extrinsic vessel compression [25] contributed to affect oxygenation. Thus we presume that all these factors together contributed to the postural hypoxemia observed in our patients. Peripheral oxygen delivery and peripheral tissue oxygenation are difficult to measure, and inadequate oxygen delivery to tissues results in the accumulation of glycolytic end products of metabolism with lactic acidosis, [26] predisposing to pressure sores of skin. We too found significant postural hypoxemia (lowered PaO 2 and PaO 2 /FiO 2 ) with the patient lying on the worse-lung side. Although the small number of patients in this study imposes limits on the results, we feel that the postural hypoxemia probably predisposed patients to higher incidence of skin pressure sores on the weight-bearing bony points on the worse-lung (higher LIS) side. Another limitation of this scoring system could be in allocating LIS in the presence of pleural effusion, which will match to the proposed LIS value of 2. Pleural effusion was not found in any of our patients; however, the differentiation between effusion and infiltration is possible by looking at mediastinal shift. Since pleural effusion too is reported to cast similar effect on oxygenation in lateral position, [27] the LIS may still hold true to predict postural hypoxemia; however, this needs confirmation. The nurses need to be aware of how different patient positions can affect arterial blood oxygenation within the critical care environment. [28] Thus a basic acumen in nurses to adjudge the hazardous position of the ventilated patient shall help them to take care of, and protect, the patients in view of this fact. This simple LIS system of bedside chest x-ray was useful in predicting asymmetry of lung ventilation in ARDS patients during mechanical ventilation. A large study based on LIS points given by the nurses to predict early-onset pressure sore needs to be undertaken in future. Conclusion Bilateral lung involvement of ARDS becomes patchy with the use of PEEP during mechanical ventilation. The proposed simple lung infiltration score predicted hypoxemia while lying on the worse lung in patients with LIS difference ≥3 in chest x-ray. The more frequent incidence of skin pressure sores on the worse-lung (higher LIS) side compared to the better-lung (lower LIS) side also correlated with hypoxemia noted in the same lateral position. Pulse oximetry may fail to give alarming signals. Thus postural hypoxemia can remain an unnoticed yet significant factor to induce early-onset skin pressure sore in critically ill patients.- Acknowledgment The authors wish to thank Prof. C. M. Pandey for his valuable guidance in statistical analysis and interpretation. We also wish to thank Dr. Sue Smith for her help in editing in terms of language and giving a facelift to the manuscript. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09072f1.jpg] [ms09072t3.jpg] [ms09072t2.jpg] [ms09072f4.jpg] [ms09072f2.jpg] [ms09072t1.jpg] [ms09072t4.jpg] [ms09072f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}