 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
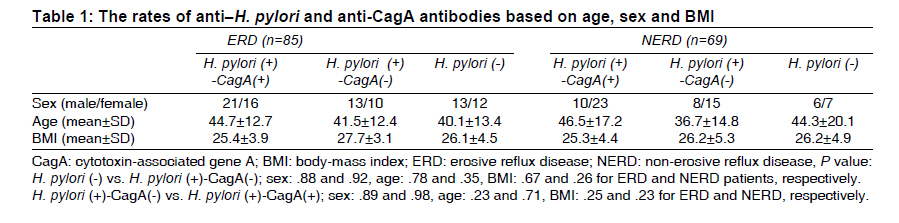
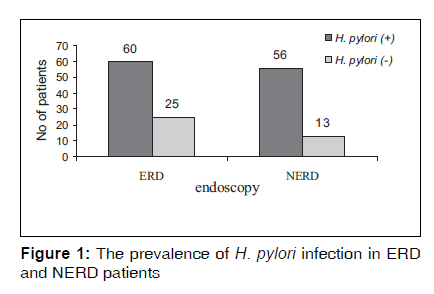
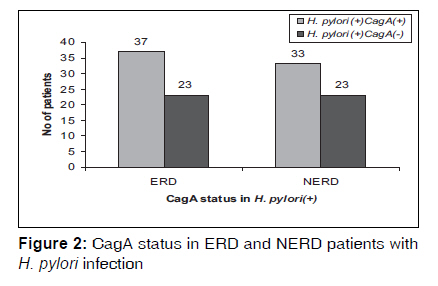
Indian Journal of Medical Sciences, Vol. 63, No. 9, September, 2009, pp. 402-407 Original Article Prevalence of Helicobacter pylori and cytotoxin-associated gene A in Iranian patients with non-erosive and erosive reflux disease Yousef Rasmi, Masoud Sadreddini 1 , Zahra Shahsavari, Sina Raeisi Department of Biochemistry and 1 Gastroenterology, Faculty of Medicine, Urmia University of Medical Sciences, Urmia, Iran Correspondence Address: Dr. Yousef Rasmi, Department of Biochemistry, Faculty of Medicine, Urmia University of Medical Sciences, Urmia, Iran Code Number: ms09073 PMID: 19805919 Abstract Background: The prevalence of Helicobacter pylori (H. pylori) infection and its virulent strain (cytotoxin-associated gene A: CagA) has not been evaluated in patients with gastroesophageal reflux disease (GERD) subgroups (erosive and non-erosive) in Iran.AIMS: This study was conducted to evaluate H. pylori infection and anti-CagA status in GERD. Setting and Design: One hundred fifty-four patients (71 male and 83 female; mean age, 42.6± 15.5 years) were evaluated for symptoms - heartburn and acid regurgitation - compatible with GERD. Materials and Methods: The esophagus was diagnosed endoscopically whether it was with erosion (erosive reflux disease, ERD) or without erosion (non-erosive reflux disease, NERD). Rates of anti-H. pylori and anti-CagA-IgG (immunoglobulin G) antibodies were determined for each subject by ELISA. H. pylori was considered by ELISA if the rapid urease test proved positive. Statistical Analysis: anti-H. pylori and anti-CagA statuses were compared in ERD and NERD patients with and without related IgG antibodies. Mean values and P values were calculated using SPSS (version 12). Results: The overall prevalence of H. pylori infection was 75.3% (116/154). Anti-CagA antibody was found in 60.3% (70/116) of infected patients. The prevalence of H. pylori infection in patients with NERD and ERD was 81.2% (56/69) and 70.6% (60/85), respectively (OR= 0.56; 95% CI [confidence interval]= 0.26-1.20; P= .14). The prevalence of anti-CagA antibody in infected NERD and ERD patients was 58.9% (33/56) and 61.7% (37/60), respectively (OR= 1.16; 95% CI= 0.49-1.70; P= 0.83). Conclusion: The results showed that more than 70% of the patients, either NERD or ERD, acquire H. pylori infection. Anti-CagA antibody is also common in patients with reflux disorders in our community. Keywords: Cytotoxin-associated gene A, Helicobacter pylori, non-erosive reflux disease Introduction Helicobacter pylori (H. pylori) is a gram-negative microaerophilic bacteria that colonize the human gastric mucosa, causing chronic infection. [1] H. pylori prevalence ranges from 25% in the developed countries to more than 80% in the developing world. [2],[3],[4] In recent decades, while the prevalence of H. pylori infection has been declining, the incidence of gastroesophageal reflux disease (GERD) has been increasing in developed countries. [3] GERD, which is induced by reflux of the gastric and duodenal contents into the esophagus, has recently come to be recognized as a serious clinical problem. [5] Regarding bacterial factors, cytotoxin-associated gene A (CagA) is thought to be the major H. pylori virulence factor involved in the pathogenesis of H. pylori diseases. [4] Patients colonized by strains containing the CagA present with more severe gastric inflammation, [6],[7] which may explain the lower levels of acid output and the lower levels of protection against GERD. [8] It is noteworthy that GERD is heterogeneous in terms of endoscopic features and etiologic factors. On the basis of whether mucosal breaks or ulcerations were noted in endoscopic examination, GERD can be classified into erosive reflux disease (ERD) and non-erosive or endoscopy-negative reflux disease (NERD). Considering the high genetic and geographic variability that characterizes H. pylori [9] and the discrepant results regarding the role of H. pylori infection in protecting against GERD, either NERD or ERD, and because the role of virulent markers of the bacteria has not been evaluated in most studies, the aim of this study was to evaluate the prevalence of antibodies to H. pylori and CagA in patients with NERD and ERD in Iran. Materials and Methods Between September 2007 and February 2008, 154 patients (71 male and 83 female; mean age, 42.6±15.5 years; range, 16-80 years) who were self- and/ or physician-referred to our university hospital were enrolled in the present study. Patients were evaluated in our endoscopy unit for symptoms compatible with GERD, namely, heartburn and acid regurgitation. A standardized questionnaire was completed for each patient during an interview. Demographic details of the GERD patients were recorded. Based on the results of upper endoscopic examination, patients were divided into 2 major groups: ERD and NERD. ERD patients were those who had heartburn and/ or regurgitation and erosions in the distal esophagus. NERD patients were those who had heartburn and/ or regurgitation but were without mucosal erosions in the distal esophagus. At first, the presence of H. pylori in gastric biopsy was determined by the rapid urease test. Peripheral heparinized blood samples were collected from each patient after endoscopy. The blood samples were centrifuged and the plasma was separated and frozen at−80°C until analysis. The presence of plasma IgG antibodies to H. pylori was determined by enzyme-linked immunosorbent assay (ELISA) kits (Globe Co. Ltd., Milan, Italy). Patients were evaluated by anti-H. pylori antibody if the rapid urease test proved positive. Infected patients were determined by the presence of IgG antibodies to CagA, also by ELISA method (DiaPro Co. Ltd., Milan, Italy). Patients with a history of gastrointestinal surgery, malignancy and antibiotics or bismuth consumption; and those who had used H 2 blockers, proton pump inhibitors or nonsteroidal anti-inflammatory drugs during the last 4 weeks were excluded from the study. This study was conducted in accordance with the Declaration of Helsinki and its revisions was approved by the ethics committee of our university. All patients were required to give written informed consent before participating in the study. Results are expressed as mean± SD. For statistical analysis, the one-way ANOVA, chi-square and Mann-Whitney U tests were carried out using SPSS software (version 12.0). P values < 0.05 were considered statistically significant. Results Of the 154 patients, ERD was found in 85 (55.0%; mean age, 40.4±14.3 years) and NERD was found in 69 (45.0%; mean age, 43.9±16.2 years) patients. There were 24 (34.8%) and 47 (55.3%) males, respectively, in the NERD and ERD groups. The mean body-mass index (BMI) was 25.6±4.7. The means of BMI of NERD and ERD patients are shown in [Table - 1]. There were no significant differences in sex, age and BMI between patients with and without H. pylori infection either in NERD group or ERD group [Table - 1]. Also, we could not find significant differences in sex, age and BMI between anti-CagA-positive and anti-CagA-negative patients in both groups [Table - 1]. The overall prevalence of H. pylori infection was 75.3% (116 out of 154 patients). H. pylori infection was found in 56 (81.2%) patients in the NERD group and 60 (70.6%) patients in the ERD group (P= 0.14) [Table - 2] and [Figure - 1]. Also, overall, anti-CagA antibody was found in 60.3% (70/116) of infected patients. We found positivity for anti-CagA antibody in 58.9% (33/56) of infected NERD patients. In contrast, anti-CagA antibody was found in 61.7% (37/60) of infected ERD patients (P= 0.83) [Table - 2] and [Figure - 2]. Discussion GERD is a common condition affecting 25% to 40% of the population. [10] Recent published epidemiologic studies, however, indicate the prevalence of GERD is increasing in Asia. [11],[12],[13] Asian GERD patients share similar risk factors and pathophysiological mechanisms with western counterparts. [14] Recently, increasing attention has been paid to the relationship between H. pylori infection and GERD, but the evidence for an association between H. pylori and GERD remains mixed and largely uncertain. Raghunath et al., in a systematic review, found a significantly lower prevalence of H. pylori infection among patients with GERD than among those without the disease. [15] This review confirmed that H. pylori infection is less prevalent in GERD patients, especially in eastern Asian countries, and there was no data about this topic from western Asian countries. The contrasting trend of GERD, H. pylori prevalence in different geographic areas and the crucial role of H. pylori in chronic gastritis suggest that H. pylori infection might act through its effect on gastritis and acid secretion to protect patients against the development of GERD. [16] Rajendra et al. reported H. pylori infection may protect complicated reflux disease via induction of corpus atrophy. [17] But we proposed that a neuroimmunological mechanism is responsible for the protective effect of H. pylori on GERD. [18] Furthermore, data revealed that 80% to 90% of Asian GERD patients had NERD. [14],[19] The clinical importance of the NERD group patients has increased in the last few years, primarily because of their lower symptom response rate to anti-reflux therapy when compared to ERD patients. [20] Although data show a relationship between GERD - mainly in ERD patients - and H. pylori infection, few studies have centered on NERD and CagA status. [21],[22],[23] Accordingly, we determined separately the prevalence of H. pylori infection and its virulent factor (CagA) in patients with NERD and ERD. Our study was performed in a series of 154 consecutive patients with reflux symptoms. Esophageal erosions were found during endoscopy in 85 of these patients. The overall prevalence of H. pylori-- was 75.3% (ERD: 60/85, 70.6%; NERD: 56/69, 81.2%). But it is not surprising for us that H. pylori infection was found in 75.3% of GERD cases, because the overall prevalence of H. pylori in Iran is still very high. [24] Similar findings have been reported from eastern Europe. In a study by Jonaitis et al., H. pylori infection was found in 60.4% of ERD patients and 80.4% of NERD patients (overall prevalence, 70.2%). [25] The high proportion of H. pylori-infected NERD patients in our region leads to the speculation that this esophageal hypersensitivity may be stimulated by H. pylori-induced inflammatory mediators and that NERD may have pathogenesis related to hypersensitivity of the lower esophagus to comparably short-term reflux episodes, which are not able to damage the esophagus. [25] In fact, in this study, the rate of H. pylori infection in both groups was similar to the background prevalence of H. pylori infection in our general population. Furthermore, we could not find any study about the CagA status in both NERD and ERD patients in our community; thus we could not compare our results with literature review. Our data could be the first published data about the prevalence of H. pylori infection and CagA status in NERD and ERD patients in this geographic area. In conclusion, this study showed trends and differences in the prevalence of H. pylori infection and anti-CagA antibody between ERD and NERD, but chi-square analysis did not show any statistically significant difference. Finally, the exact influence of H. pylori infection and its virulent strain on the pathogenesis of GERD subgroups - either NERD or ERD - is not fully known. However, this is an evolving area with ongoing research, and further assessments in large-sample studies are warranted. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09073t2.jpg] [ms09073t1.jpg] [ms09073f2.jpg] [ms09073f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}