 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
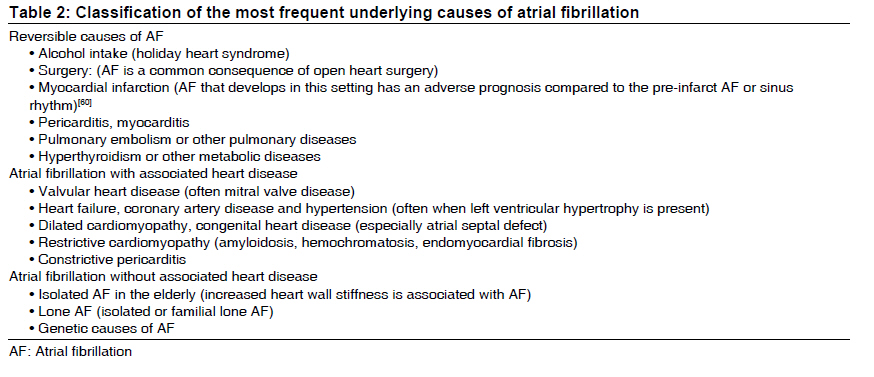
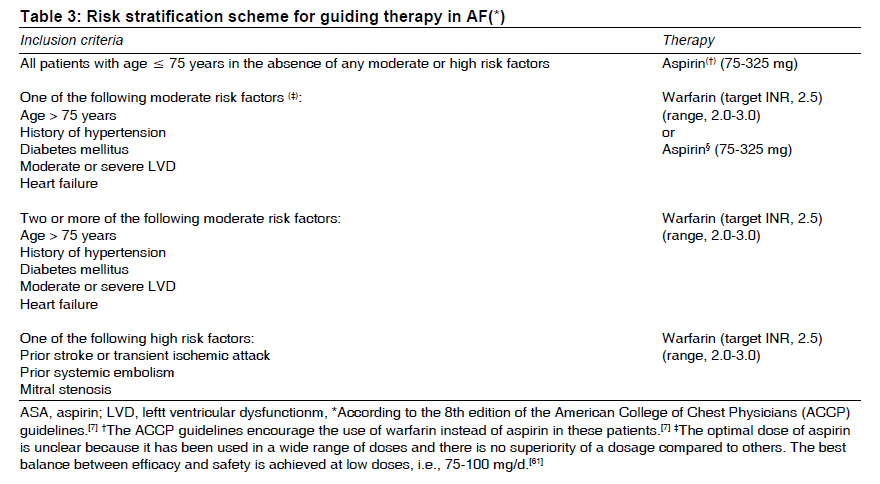
Indian Journal of Medical Sciences, Vol. 63, No. 9, September, 2009, pp. 419-430 Practitioners section Management of nonvalvular atrial fibrillation : A comprehensive approach Luigi Iuliano, Antonio Di Matteo, Giuseppe Straface Department of Internal Medicine, Unit of Vascular Medicine, Sapienza University of Rome, Rome, Italy Correspondence Address: Prof. Luigi Iuliano Sapienza, University of Rome, Unit of Vascular Medicine at Polo Pontino, Goretti Hospital, Corso della Repubblica 79. 04100 Latina. Italy Code Number: ms09079 PMID: 19805924 Abstract Atrial fibrillation is the most common arrhythmia in clinical practice, may coexist with conditions common to both cardiovascular and noncardiovascular diseases and is associated with considerable morbidity and mortality. Atrial fibrillation is often asymptomatic and diagnosed only when it has caused a potentially serious complication, such as an ischemic stroke. When atrial fibrillation has been identified, 2 objectives have to be addressed - the antiarrhythmic therapy based on rate control or rhythm control, and prevention of thromboembolism. A rhythm or rate control strategy can be chosen indifferently because they have comparable efficacy for the outcome measure of mortality, but the antithrombotic therapy is ever mandatory. The risk of stroke increases cumulatively with increasing age, previous transient ischemic attack or stroke, hypertension, diabetes mellitus, impaired left ventricular function and heart failure. Warfarin reduces the risk of stroke by about two thirds; and aspirin, by about one fifth, but its use must be weighted with the risk of bleeding. The risk of anticoagulant-associated hemorrhage increases with age, the presence of serious concomitant diseases, with poorly controlled hypertension and poorly controlled anticoagulation.Keywords: Aspirin, atrial fibrillation, stroke, thromboembolism, thrombosis, warfarin Introduction Atrial fibrillation (AF) is the most common sustained cardiac rhythm disturbance. It may cause symptoms of decreased cardiac output (i.e., malaise and effort intolerance), dyspnea or palpitations and is associated with an increased risk of worsening ventricular function and systemic thromboembolic events. Its prevalence increases with age, from about 2% in the population younger than 65 years to 5% in people older than 65 years and 10% in people older than 75 years. [1],[2],[3] The risk of stroke averages about 5% per year among all individuals with AF, which is about 5-6 times greater than the risk of stroke for people of the same age who are in sinus rhythm. It may occur as a single episode, a series of recurrent episodes or continuously, and it is often associated with structural heart diseases, even if a substantial proportion of patients with AF have no detectable heart disease. The management of AF is based on the following caveats: a) recording, classification and identification of potential underlying causes; b) choosing the antiarrhythmic strategy; c) preventing systemic thromboembolism. Classification of Atrial Fibrillation Few conditions produce a disparate range of presentations or result from so many different causes as does AF. Assorted nomenclatures have been used to describe the pattern of AF, including acute, chronic, paroxysmal, intermittent, constant, persistent and permanent, which makes it difficult to compare studies of AF or the effectiveness of therapeutic strategies based on these designations. [4],[5],[6] [Table - 1] reports a classification scheme recommended for simplicity and clinical relevance in the American College of Cardiology/ American Heart Association/ European Society of Cardiology (ACC/ AHA/ ESC) 2006 guidelines. [6] AF is also classified as valvular AF or non-valvular AF. This review pertains to non-valvular AF, which requires accurate patient evaluation for managing thromboembolic risk. Valvular atrial fibrillation carries the highest risk of thromboembolism and in the majority of cases necessitates treatment with warfarin. AF is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation associated with an irregular, frequently rapid ventricular response. The electrocardiographic signs of AF are the absence of P waves and irregular RR intervals, even if the RR intervals may be regular in the presence of a low heart rate. It can be isolated or associated with other tachyarrhythmias, such as atrial tachycardia or atrial flutter. [3] Atrial flutter is a supraventricular tachyarrhythmia characterized by an electrocardiographic pattern of atrial tachycardia ≥240/min, with a uniform and regular continuous wave form. Atrial flutter differs from atrial tachycardia in that the P-waves are separated by isoelectric lines in a rate < 240/min. [3] Unlike AF, the RR intervals in atrial flutter are often regular and atrial-ventricular conduction is frequently 2:1; but if the flutter rate is slower, conduction can be up to 1:1. The background and diseases associated with atrial flutter are similar to those of atrial fibrillation, including hypertension, coronary disease, valvulopathy, chronic obstructive pulmonary disease and myocardiopathy. [3] According to current guidelines, atrial flutter should be considered as equivalent to atrial fibrillation for thromboembolic risk and treated accordingly. [7] Identification of the Possible Underlying Causes [Table - 2] reports the most frequent causes of AF. Both cardiovascular and noncardiovascular diseases can be associated with AF. Some diseases are transient and eventually there is no need to treat AF, because the removal of the underlying cause generally resolves the arrhythmia. The term "lone AF" identifies a group of patients less than 40 years of age without structural heart diseases who have a better prognosis concerning thromboembolism and mortality. Familial lone AF, defined as a lone AF running in the family, is probably caused by genetic mutations, which are largely unknown. Recently, in 11 members of a white family of northern European ancestry with AF, a mutation in the gene encoding atrial natriuretic peptide has been identified. [8] The incidence of AF in patients who underwent cardiac surgery was found to be between 20% and 50% and usually occurred within the fifth day after open-heart surgery, with a peak incidence on the second day. [9] Patients who develop postoperative AF have a higher risk of mortality and longer hospitalization than patients without this arrhythmia. [9],[10] Generally, the postoperative AF is self-limiting, with the spontaneous restoration of sinus rhythm in more than 90% of patients within 6-8 weeks after surgery. [11] Choosing the antiarrhythmic therapy - rhythm control or rate control Two main strategies are available for management of atrial fibrillation: rate control and rhythm control. The aims of heart rate control in atrial fibrillation are to minimize symptoms associated with excessive heart rates and to prevent tachycardia-associated cardiomyopathy. [12] Although the atria continue to fibrillate, this strategy is considered an effective treatment as it can improve symptoms and reduce the risk of associated morbidity. The current guidelines recommend in atrial fibrillation a ventricular rate of 60 to 80 beats per minute at rest, and 90 to 115 beats per minute during exercise. [9] Rhythm control involves the use of electrical or pharmacological cardioversion or electrophysiological/ surgical interventions to convert the arrhythmia associated with atrial fibrillation to normal sinus rhythm. Patients who have been successfully cardioverted are generally treated with antiarrhythmic drugs in the long term to prevent recurrence of atrial fibrillation. Rhythm control strategies also require the appropriate antithrombotic treatment to reduce the risk of stroke and thromboembolism. Until recently, there were uncertainties about the most appropriate initial treatment strategy - rate control or rhythm control. Several concordant trials have now demonstrated no inferiority of rate control compared to rhythm control or vice versa for the outcome measures of mortality and quality of life. [13],[14],[15],[16],[17] The "atrial fibrillation follow-up investigation of rhythm management" (AFFIRM) study, however, found mortality to be higher for rhythm control in patients with coronary heart disease and those> 65 years old; higher incidence of stroke, arrhythmia and better outcome in younger people and in patients with left ventricular dysfunction in the rhythm control group. [14] Higher rate of hospitalizations was reported in the rhythm control group in the AFFIRM study and in the "how to treat chronic atrial fibrillation" (HOT CAFΙ) studies. [16] A secondary analysis in "the pharmacological intervention in atrial fibrillation" (PIAF) study showed a better exercise tolerance in the rhythm control group. [18] In addition, it has been reported that in patients with AF and heart failure, the routine use of a rhythm-control strategy is not associated with a lower mortality, as compared with a rate-control strategy. [19] In the PIAF study, [18] the rhythm-control strategy resulted in better exercise performance but did not affect symptoms or quality of life, and was associated with an increased number of hospitalizations for repeated cardioversion and for the adverse effects of antiarrhythmic drugs. Rate-control treatment is based on pharmacological depression of conduction through the atrioventricular node. Three classes of drugs are generally used for the rate-control treatment: β-blockers (i.e., metoprolol, propanolol), non-dihydropyridine calcium antagonists (i.e., verapamil, dialtiazem) and digoxin. [19] In the absence of pre-excitation, b-blockers and calcium antagonists are the first-choice drugs to reduce the heart rate. Esmolol is a short-acting b-blocker that can be administrated to slow the ventricular response to AF in the acute setting. [19] In patients who fail to respond to rate control-lowering drugs, nonpharmacological measures such as atrioventricular nodal ablation may be considered. [20] The rhythm-control strategy involves the attempt to restore sinus rhythm through cardioversion - pharmacological cardioversion and electrical cardioversion. Recent-onset AF reverts spontaneously within 24 hours in at least half of the patients. [21] If the paroxysm does not rapidly revert, a strategy of intervention must be chosen according to the duration of AF. Pharmacological cardioversion should be the preferred option in patients presenting with recent onset, within 48 hours, atrial fibrillation; while electrical cardioversion is regarded as the preferred strategy when the atrial fibrillation is more prolonged. In clinical practice, Vaughan-Williams class IA, IC and III antiarrhythmic drugs are commonly used for pharmacological cardioversion. [20] Beta-blockers, non-dihydropyridine calcium antagonists and digoxin are ineffective to restore the sinus rhythm. [21,22] With the exception of the b-adrenergic-blocking drugs, most antiarrhythmic agents are associated with a risk of proarrhythmia in the presence of electrolyte abnormalities and ischemic or structural heart disease. [23] No difference between the two types of cardioversions has been found regarding the efficacy to restore sinus rhythm and other issues (i.e., incidence of thromboembolism and stroke). [20],[24] As outlined by the current guidelines, [7] patients who have been in AF for less than 48 hours are eligible for early cardioversion, while patients who have been in AF for more than 48 hours should be considered for anticoagulation therapy and elective cardioversion. All the strategies require appropriate administration of antithrombotic therapy to reduce the risk of stroke and other thromboembolic events. If the onset of AF is> 48 hours, it is not possible to proceed to early cardioversion, because of the increased risk of stroke and thromboembolic events after cardioversion. There are two strategies available to minimize the thromboembolic risk due to cardioversion. The first strategy consists in the administration of anticoagulant therapy for a minimum of 3 weeks before and for a minimum of 4 weeks after cardioversion without any interruption. This recommendation is based on the evidence that left atrial thrombi grow and adhere to the endothelial surface within 2 weeks. The second strategy is based on the evidence that success in cardioversion is higher in recent-onset AF, and it considers trans-esophageal echocardiography to look at left atrial/ appendage thrombosis. In the absence of thrombosis, heparin is usually given concomitantly with cardioversion, and the anticoagulant therapy with warfarin to be given for a minimum of 4 weeks is started. Patients in whom a thrombus is identified by trans-esophageal echocardiography are considered to be at high risk of thromboembolism after cardioversion, and are usually treated with conventional therapeutic anticoagulation for at least 3-4 weeks before the trans-esophageal echocardiography is repeated. Current clinical studies suggest that trans-esophageal echocardiography-guided cardioversion has efficacy comparable to conventional strategy, [25],[26] even if some studies have demonstrated a higher incidence of thromboembolic events after trans-esophageal echocardiography-guided cardioversion, [27] probably due to undetected heart thrombosis. It should be underscored that whatever strategy is chosen, the patient must be evaluated for the long-term antithrombotic prophylaxis according to her/ his risk profile. The low efficacy of prophylactic antiarrhythmic agents and the incidence of their potentially proarrhythmic effects have promoted research of nonpharmacological strategies for prevention and control of AF, based on surgical or radiofrequency ablation at critical locations (Maze procedure types I, II and III) in order to create barriers that block electric loop circuits and eventually prevent AF. [28],[29],[30],[31] Risk Stratification for Stroke and Systemic Thromboembolism Not all patients with AF have to be treated with thromboprophylactic therapy. The decision to treat depends on the balance between the risk of thromboembolism and the risk of bleeding in each patient. Several prominent risk stratification schemes have been developed to distinguish those patients with AF who are at high risk of systemic thromboembolism from those with a low risk in whom anticoagulation might not be beneficial when considering the associated risk of bleeding. [32],[33],[34],[35],[36] The initial schemes were developed according to the multivariate analyses of data from the initial large randomized trials: the "Atrial fibrillation investigators" (AFI) and the "Stroke prevention in atrial fibrillation" (SPAF). [37],[38] A point score system based on merging AFI and SPAF schemes constitutes the CHADS2 system (Congestive heart failure, Hypertension, Age, Diabetes mellitus, Stroke). [39] The Framingham score system was based on a cohort study among 705 patients with new-onset AF to predict the 5-year risk of stroke. [40] An expert opinion panel developed a guideline for the American College of Chest Physicians (ACCP), of which the last edition (8 th edition) is summarized in [Table - 3]. [7] Some clinical and echocardiographic parameters can be used to assess the thromboembolic risk for patients with AF. [7] The clinical parameters are increasing age, history of previous transient ischemic attack or stroke, hypertension and diabetes mellitus. [7] The evidence regarding diabetes mellitus, along with gender and other patient characteristics, as a predictor of stroke risk seems less consistent according to some authors. [41] Among echocardiographic parameters, several studies have demonstrated that the moderate-to-severe left ventricular systolic dysfunction is the only independent prognostic factor. [37],[42],[43] All these risk factors are cumulative - for people younger than 65 years with no risk factors, the annual risk of stroke is about 1%, whereas for people with one or more risk factors, it is about 5%; for people aged 65-75 years with no risk factors, the annual risk of stroke is about 4%, and for people with one or more risk factors, it is about 6% per year; and for people older than 75 years with no risk factors, the risk of stroke is about 3%-4%, whereas for people with one or more risk factors, it is about 8%. Individuals less than 65 years of age with AF and having no echocardiographic evidence of any concurrent heart disease show a very low risk of a thromboembolic event (about 0.6% per year). [44] For some people, such as the elderly and those with hypertension, whose risks of stroke and bleeding are both high, the treatment decision can be difficult and may be determined ultimately by the patient's compliance. [35],[45] The different risk stratification schemes have comparable, but only limited, overall ability to predict thromboembolism, and the connected antithrombotic therapy may vary widely depending on which scheme is applied. [46] We suggest using the scheme reported in [Table - 3], prepared according to the last guidelines developed by the ACCP Consensus Conference. [7] Choosing the Anti -Thromboembolic Therapy After selecting the risk class for a given patient, antithrombotic therapy is relatively easy to choose. In fact, despite the numerous antithrombotic drugs available, in the setting of AF, only 2 drugs are indicated by the current guidelines, viz., warfarin and aspirin. Several clinical trials have shown that in people with chronic AF, warfarin reduced the risk of stroke by approximately two thirds (68%; 95% CI, 50%-79%; P< 0.001), from about 4.5% to 1.4% per year, overall. [47],[48],[49] The aim of oral anticoagulant therapy, which provides the best balance between the prevention of thromboembolic events and the occurrence of bleeding complications, is holding international normalized ratio (INR) between 2.0 and 3.0. [37],[45] In people in whom anticoagulant therapy is indicated, the risk of stroke increases substantially when the INR falls below 2.0. patients with an INR of 1.7 have twice the odds of stroke (95% CI, 1.6-2.4 times) and those with an INR of 1.5 have 3.3 times the odds of stroke (95% CI, 2.4-4.6 times) compared to those with an INR of 2.0. [37] In patients with AF, aspirin reduced the incidence of stroke by 28% (95% CI, 2%-38%), from 5.2% (placebo) to 3.7% (aspirin) per year for primary prevention (absolute risk reduction, 1.5% per year) and from 12.9% (placebo) to 10.4% (aspirin) per year for secondary prevention (absolute risk reduction, 2.5% per year). [50] It has been suggested that aspirin prevents strokes due to atherothromboembolism but not cardiogenic embolism associated with AF. This interpretation is based on the intensity of its effect, which is very similar to the effect of aspirin in patients with symptomatic atherothromboembolism of the brain, heart and limbs (about 20% relative risk reduction). [36] The association of antiplatelet treatment with a low-intensity anticoagulant therapy is less effective than the adjusted dose of warfarin alone. [51],[52],[53] The "atrial fibrillation clopidogrel trial with ibesartan for prevention of vascular events" (ACTIVE) was initiated to evaluate the role of clopidogrel plus aspirin in the prevention of thromboembolism in patients with atrial fibrillation. Active-W study, which compared clopidogrel plus aspirin with warfarin, demonstrated that oral anticoagulant therapy is superior (annual risk, 3.93%) to double antiplatelet therapy, aspirin plus clopidogrel (annual risk, 5.60%; relative risk, 1.18%-1.76%; P= 0.0003), for preventing vascular events in patients at high risk of stroke. [54] A subsequent analysis of the ACTIVE-W study indicated that the combination therapy of aspirin plus clopidogrel is not an equivalent alternative to oral anticoagulants for patients with low risk of stroke (CHADS2=1). [55] ACTIVE-A trial compared clopidogrel plus aspirin alone in patients with atrial fibrillation who were at increased risk for stroke and for whom therapy with warfarin was considered unsuitable. [56] In those patients of the ACTIVE-A trial, the addition of clopidogrel to aspirin reduced the risk of major vascular events, especially stroke, but at the cost of increasing the risk of major hemorrhage. [56] Results of the "Birmingham atrial fibrillation treatment of the aged" (BAFTA) trial showed that even among elderly patients with AF, anticoagulation with warfarin was superior to that with aspirin for primary stroke prevention. [57] A scheme of risk stratification-based antithrombotic therapy in persons with AF according to the 2008 guidelines of the ACCP Consensus Conference is outlined in [Table - 3]. Paroxysmal AF should be considered for treatment just as chronic AF because the length of AF episode is not related to the risk of stroke. [7,58] Patients taking aspirin should be followed up and eventually shifted to warfarin in the presence of emerging additional risk factors. This situation occurs in 10% to 15% of patients being treated with aspirin per year. [59] Risk of bleeding The large reduction in the risk of stroke obtained with warfarin in patients with chronic AF is associated with a little increase in frequency of major bleeding (warfarin, 1.2%; control, 1.0%) or intracranial hemorrhage (warfarin, 0.3% per year; control, 0.1% per year). [47],[48],[49] However, it should be underlined that the reported rates of bleeding pertain to patients who were carefully selected and screened and do not necessarily reflect the rates in real clinical practice. The major risk factors for anticoagulant-associated intracranial hemorrhage include previous symptomatic cerebrovascular disease, computed tomography brain scan evidence of small-vessel disease, poorly controlled hypertension, the tendency to fall and female gender. Increasing age is a potent risk factor for anticoagulant-associated hemorrhage. Among a subgroup of patients in the SPAF II trial with a mean age of 80 years, the rate of intracranial hemorrhage was as high as 1.8% per year in those allocated to warfarin therapy (target INR, 2.0-4.5) and 0.8% among those who were assigned to aspirin. [51] Although the target INR in this study was higher (INR, 2-4.5) than currently recommended (INR, 2.0-3.0), these data suggest that the low rate of intracranial hemorrhage reported in the five primary prevention AF trials [ 48],[49] may not apply to very elderly individuals. In fact, the mean age of the patients studied in the AF trials was 69 years, and only about a quarter were older than 75 years. The potential benefits of aspirin (which may reduce the risk of stroke by 0.12% per year) may be offset by an equally potential risk of aspirin-associated hemorrhagic stroke of 0.12%. [45] Aspirin was not associated with any significant excess of intracranial hemorrhage (aspirin, 0.16%; control, 0.13%) or major extra-cranial bleeding (aspirin, 0.5%; control, 0.6%). [50] In the ACTIVE-W trial, which evaluated the efficacy of warfarin vs. aspirin plus clopidogrel, rates of major hemorrhage were similar in the warfarin group and in the aspirin plus clopidogrel group; however, significantly minor bleeds occurred with aspirin plus clopidogrel therapy than with warfarin therapy. [54] In the ACTIVE-A trial, which evaluated the efficacy of the double antiplatelet therapy (aspirin plus clopidogrel) vs. aspirin alone, major bleeding occurred at a lower rate in patients receiving aspirin plus clopidogrel than in patients receiving aspirin alone (2.0% per year vs. 1.3% per year; relative risk, 1.57; 95% CI, 1.29-1.92; P< 0.001). [56] With clopidogrel, the most common site of hemorrhage was the gastrointestinal tract. With the combination of major vascular events (the primary outcome) and major hemorrhage, there was no significant difference between the overall event rate with aspirin plus clopidogrel and the rate with aspirin alone (968 vs. 996 events; relative risk, 0.97; 95% CI, 0.89-1.06; P= .54). [56] Results of the BAFTA trial showed that even among elderly patients with AF, the superiority of anticoagulation with warfarin, compared to aspirin, for primary stroke prevention was without the cost of more major hemorrhage, the rates of which were similar between groups. [57] Thus, current practice necessitates individualization of therapy after an integrated clinical assessment aimed at evaluating thromboembolic risk due to AF, other potential indications for anticoagulant therapy, risk of hemorrhage and nonmedical factors relating to compliance, capacity to have the INR monitored at least monthly, gait instability, risk of other trauma, and patient values and preferences. [39],[45],[61] References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09079t2.jpg] [ms09079t1.jpg] [ms09079t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}