 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
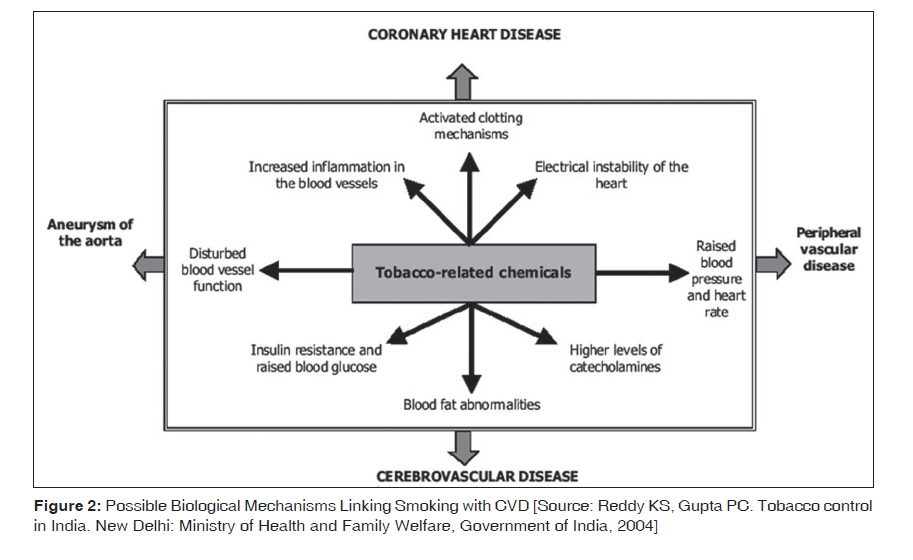
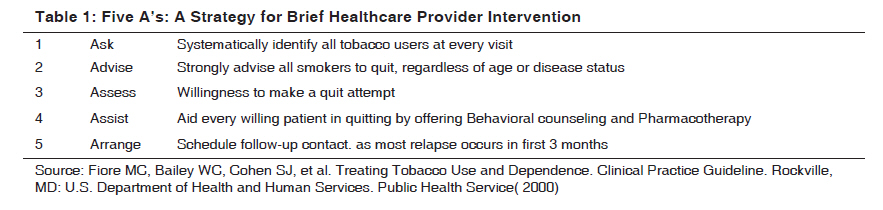
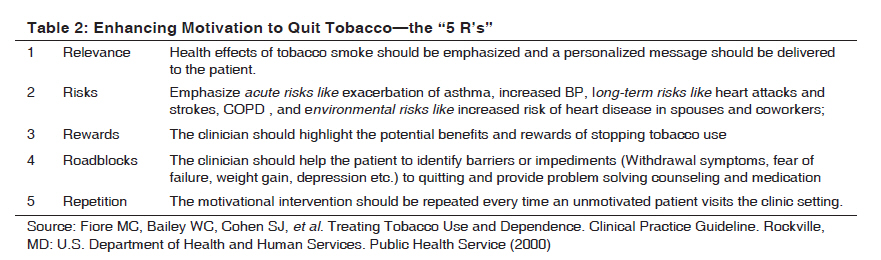
Indian Journal of Medical Sciences, Vol. 63, No. 11, November, 2009, pp. 520-533 Practitioners section Smoking and cardiovascular health: A review of the epidemiology, pathogenesis, prevention and control of tobacco Prasad DS, Kabir Zubair, Dash AK, Das BC Sudhir Heart Centre, Berhampur-760 002, Orissa Code Number: ms09097 PMID: 20075556 DOI: 10.4103/0019-5359.58884 Abstract The causal associations between cigarette smoking and human diseases are irrefutable. In this review, we focus on the epidemiological pattern of cigarette smoking on cardiovascular risk, the underlying mechanistic process of such a causal link, how to prevent premature cardiovascular morbidity and mortality particularly through smoking cessation, and the health benefits of such cessation measures. Finally, we conclude our review summarizing a few of the proven evidence-based tobacco control strategies and policies from across the globe. We did not conduct a systematic review but followed a similar structure. We abstracted the most relevant published literature on the electronic databases, namely, PubMed, Embase and the Cochrane Library applying specific search terms. We also searched gray literature and consulted experts in the field for cross-references. Smoking has been estimated to cause about 11% of all deaths due to cardiovascular disease. Smoking contributes to the pathogenesis of coronary artery disease and sudden death through a variety of mechanisms, including the promotion of atherosclerosis, the triggering of coronary thrombosis, coronary artery spasm, and cardiac arrhythmias, and through reduced capacity of the blood to deliver oxygen. Smoking cessation also confers substantial benefits on people with serious heart disease. Smoking cessation should be viewed as therapeutic rather than preventive intervention, similar to treating asymptomatic hypertension. Smoking cessation is highly cost-effective relative to other frequently used medical and surgical interventions. Tobacco related illnesses are important public health issues worldwide. It has been estimated that there are1.1 billion smokers worldwide and 250 million of them live in India. Keywords: Cardiovascular disease, risk factor, smoking Introduction Cardiovascular disease (CVD) is the leading cause of death worldwide. [1] Cigarette smoking is a major modifi-able risk factor for CVD, including coro-nary artery disease (CAD), stroke, peripheral vascular disease, and congestive heart failure. [2],[3] The relationship between cigarette smoking and many established risk factors for CVD have been studied. Cigarette smoking has been associated with higher serum levels of cholesterol, coronary vasomotor reactivity, platelet aggregation, and a prothrombotic state [4],[5],[6],[7] By the year 2030, cigarettes will kill 10 million people per year, 70% of them in low- and middle-income countries [8] There are multiple and interacting determinants that affect smoking [9] These are physiological factors (nicotine addiction), personal characteristics (demographics, personality, education, information), cognition and skills, environment (social, cultural, economic and political) and other concurrent habits (drinking alcohol, coffee etc). [10] In children the main influences in smoking initiation are environmental factors and personal characteristics. [10] Tobacco related illnesses are important public health issues worldwide. The need for a comprehensive review of this particular topic has arisen in view of the ever increasing incidence of this entity and consequent avoidable cardiovascular morbidity and mortality especially in our developing nations. In this review, we focus on the epidemiological pattern of cigarette smoking on cardiovascular risk, the underlying mechanistic process of such a causal link, how to prevent premature cardiovascular morbidity and mortality particularly through smoking cessation, and the health benefits of such cessation measures. Finally, we conclude our review summarizing a few of the proven evidence-based tobacco control strategies and policies from across the globe. We did not conduct a systematic review but followed a similar structure. We abstracted the most relevant published literature on the electronic databases, namely, PubMed, Embase and the Cochrane Library applying specific search terms such as "smoking"; "tobacco use"; "CVD"; "CHD"; "AMI"; tobacco cessation; secondhand smoke; environmental tobacco smoke; passive smoking; active smoking; smoke free policies; bans; taxes. We also searched articles unpublished on the Pub Med; abstracts of conference/meetings; consulting authors/experts in the field; text books; publications of governmental/non-governmental organization. Articles only in English language were considered. Smoking Prevalence Tobacco use is a major health and social problem worldwide. [11] Smoking is one of the most potent and prevalent addictive habits, influencing behavior of human beings for more than four centuries. The scientific term for tobacco, Nicotiana, and the alkaloid in tobacco responsible for addiction, nicotine, owes to French Ambassador to Portugal, Jean Nicot who popularized the idea that tobacco had curative powers. [12] Nicotine is a powerful pharmacologic agent with a wide variety of stimulant and depressant effects involving the central and peripheral nervous, cardiovascular, endocrine, and other systems. These effects contribute to nicotine′s addictive properties. [13] Smoking is now increasing rapidly throughout the developing world with approximately one-third of smokers living in China [14] and is one of the biggest threats to current and future world health [15] There are 47.5% of men and 10.3% of women are current smokers and Tobacco continues to be the second major cause of death worldwide. [16] Furthermore, while the prevalence of tobacco use has declined among men in some high income countries, it is still increasing among young people and women [17] Cigarette smoking is the most widespread type of tobacco use world over but in India it is chewing tobacco and bidi are the dominant forms of tobacco consumption. [18] Smoking causes a huge and increasing number of untimely deaths in India. [19] Fatality from CAD in India is exacerbated by smoking of bidis or cigarettes. [20] India′s tobacco use is complex. [21] The prevalence of smoking and tobacco use in India has been inadequately reported. Smokers in India consume tobacco in various forms- rolled tobacco leaves (bidi), Indian pipe (chillum, hookah), cigarettes and tobacco-chewing -and more than one form is used by many making it difficult to accurately measure the amount of tobacco consumed. [22] There are currently 240 million tobacco users aged 15 years and above (195 million male users and 45 million female users) in India. [18] The prevalence of tobacco use is higher in rural population compared to that in urban areas. [18] Systemic Effects of Smoking Smoking affects numerous organ systems resulting in various tobacco-related diseases. The well known health hazards of tobacco smoking concern to diseases of the respiratory tract such as COPD, pneumonia and cancer, particularly lung cancer and cancers of the larynx and tongue. [23],[24] It is now clear that tobacco smoking has been implicated in etiology of cardiovascular diseases like CAD, aortic aneurysm, stroke and peripheral vascular diseases. [14] It has also been implicated in cancers of bladder, pancreas, esophagus, stomach, kidney, leukemia to a substantial extent. [14] Non-fatal diseases, such as cataracts, hip fracture, and periodontal disease are also caused by smoking. [14] Pulmonary effects of smoking are due to direct chemical exposure and chronic systemic diseases like atherosclerosis and COPD are due to indirect consequences of the exposure, even though the specific mechanism for the same is yet to be clearly delineated. [25] Environmental Tobacco Smoke (ETS) or Second hand Smoke (SHS) Exposure to ETS is associated with an increased risk of death from heart disease, lung cancer, and an increased frequency of respiratory infections in children. [26] It is clear from epidemiologic studies that exposure to ETS increases the risk of CAD by 20 to 30%. [26] Individuals with CAD who are exposed to ETS have increase in heart rate, blood pressure, carboxyhemoglobin; and they experience an approximately 20 to 40% reduction in exercise capacity. [27] Moreover, physiologic and biochemical studies have documented deleterious effects of ETS on platelets, endothelial progenitor cells, endothelial function, and cellular respiration. [28],[29],[30] Recent studies have concluded that even brief exposures to ETS may cause significant adverse effects on numerous systems of the human body and represent a significant health hazard. [31] Smoking and Cardiovascular Disease Smoking and exposure to passive smoke are both major preventable causes of cardiovascular morbidity and mortality. [32],[33] The hazardous effects of smoking on the cardiovas-cular system is due to the acute effects on platelets, function of endothelial progenitor cells, vascular endo-thelial function, and heart rate variability whether it is in active smokers or in passive smokers. [29],[30] These effects, both, increase the likelihood of an acute event as well as contribute to long-term development of CAD. Both the adverse effects of cigarette smoke and the benefits of smoking cessation on cardiovascular health occur rapidly. The risk of myocardial infarction falls by half within a year of cessation. [34] Cigarette smoking is a major risk factor for all manifestations of CAD, stroke, aortic aneurysm and peripheral artery disease. [35],[36] The risk for CAD among smokers is dose-related, [35] and smoking as little as one to four cigarettes per day significantly increases risk. [37] Women whose smoking patterns are similar to patterns of men have a similar increased risk of CAD morbidity and mortality. [37] Smoking increases the risk of all CVD; however, the magni-tude of increased risk differs by CVD type. [38] Because of the acute effects of smoking, preoperative smoking increases the risk of cardiovascular and wound-related complications during general surgery. [38],[39] SHS has similar effects and operates through the same biologic pathways as active smoking. [29] Evidence of Smoking-induced Cardiovascular Disease Tobacco and CVD (Global evidence): As per global epidemiological studies like Multinational INTERHEART study, [40] the WHO MONICA (multinational monitoring of trends and determinants in CVD), [41] the International Studies of Infarct Survival (ISIS), [42] Malaysian study [43] and Italian study [44] to name a few, smokers were found to be at increased risk of CVD compared to non-smokers. The evidence was consistent across countries. These studies also revealed a dose-response relationship. Similarly passive smoking both acute and chronic is also associated with significant cardiovascular effects. [45],[46] Tobacco and CVD (Indian evidence): The association between tobacco and CVD has not been extensively studied in the Indian context. The evidence comes mostly from cross-sectional surveys and case-control studies. [20],[40],[47],[48] These studies have several methodological limitations in assessing causation: survival bias. Tobacco control and CVD risk reduction: There is evidence of CVD risk reduction with comprehensive tobacco control laws. [49],[50] Pathophysiology of Smoking and Cardiovascular Disease The mechanisms by which cigarette smoke causes CVD are multiple and are synergistic. [29],[30],[31] They include thrombosis, endothelial dysfunction, atherosclerosis, and hemodynamic effects. [29],[30],[31] In addition, tobacco smoke may also cause insulin resistance, a risk factor for diabetes and CVD. [51] The same mechanisms responsible for CVD in active smokers are nearly as large in passive smokers. [29] Many of these effects occur immediately after a smoker or nonsmoker inhales cigarette smoke. [30],[31] Smokers also have a higher risk of recurrent ischemia after coronary artery bypass graft surgery and of re-occlusion after an acute myocardial infarction. [52] Cigarette smoke has more than 4800 identified chemical compounds and 69 carcinogens. [53],[54] Side-stream smoke contains relatively higher concentration of toxic gaseous components than mainstream smoke. [55] Nico-tine is the component responsible for the addiction, but is probably not the only major agent acting on the cardiovascular system. [56] The specific ingredients of cigarette smoke respon-sible for its cardiovascular effects are not fully recognized, but include the polycyclic aromatic hydrocarbons, [28] oxidiz-ing agents, [52] and particulate matter. [57] Possible Biological Mechanisms Linking Smoking with CVD [Figure - 2] [18] Each of these mechanisms are described in following sections. Please see [Figure - 2]. [18] Atherosclerosis Hastening of atherosclerosis due to smoking is attributed to a number of mechanisms: direct endothelial damage, increased proliferation of smooth muscle in atherosclerotic lesions, decreased endothelium-dependent coronary vasodilatation, and reduced levels of high-density lipoprotein cholesterol (HDL-C), [35] lipid levels and inflammation, both key players in the ath-erosclerotic process, are affected by tobacco smoke. Cigarette smokers have a more atherogenic lipid profile than non-smokers. [33] The antiatherogenic subfraction HDL 2 is lower in smokers and passive smokers. [52],[58],[59] Smokers and passive smokers have higher levels of products of lipid peroxidation and oxidized LDL compared to those nonsmokers. [33],[60] Smoking induced endothelial injury may result from oxidative damage caused by lipid peroxidation and production of free radicals. [61],[62] There is evidence that inflammation and hyper homocysteinemia may be important mechanisms by which smoking promotes atherosclerotic disease. [63] Subclinical and clinical atherosclerosis have been consis-tently associated with smoking in a dose-response relation-ship. [33] Subclinical atherosclerosis, measured as the carotid intimal-medial thickness (IMT), was increased in smokers in the Atherosclerosis Risk in Communities Study. [64] Clinical atherosclerosis, manifested as intermittent claudication, is increased in smokers. [33],[65] Thrombosis Smoking promotes thrombosis by multiple mechanisms. [38] In addition to effects of smoking on atherosclerosis, smoking promotes coronary artery thrombosis by increasing platelet adherence to endothelium and platelet aggregation [35] Platelet activa-tion is one of the major factors by which tobacco smoke medi-ates the pathogenesis of CVD, which may be related to endothelial dysfunction and/or direct effects of oxidant chemicals. [38],[66] Smoking-related endothelial dysfunction results in reduced release of nitric oxide, which normally inhibits platelet activation, [67] and Impaired coronary tissue plasminogen activator (tPA) release associated with coronary atherothrombosis [68] and increased secretion of plasminogen activator inhibitor-1(PAI-1), [69] which result in impaired fibrinolysis. There is recent evidence that ETS may affect the vascular endothelium both by direct injury and interference with vascular repair. [31] Coronary Artery Spasm Smoking, both chronic and acute, induces vasoconstrictor effects on coronary vasculature. [35] Current smokers have 20 times the risk of vasospastic angina compared to never-smokers. Smoking-associated vasoconstriction is mediated by an alpha-adrenergic increase in arterial tone and by smoking-associated increases in platelet and plasma vasopressin, vasopressin carrier protein, and oxytocin. [35] Arrhythmias and Reduced Oxygen-Carrying Capacity Nicotine-induced release of catecholamines increases blood pressure and heart rate and may produce a lowered threshold for ventricular arrhythmias. The combination of increased myocardial oxygen demand due to nicotine′s sympathetic effects and impaired oxygen exchange due to increased carboxyhemoglobin can produce or exacerbate myocardial ischemia. These effects on oxygen delivery may also lower the threshold for ventricular arrhythmias. [35] Heart rate variability (HRV) is reduced by passive exposure and cessation of the same leads to an increase in HRV. [70],[71],[72] Effects on Energetics The ability of the myocardial muscle to convert oxygen into the energy molecule adenosine tri-phosphate is impaired by smoking. [73] It is because the activity of the enzyme that mediates this process, cytochrome oxidase declines with acute and chronic exposure to tobacco smoke. [74],[75] Hemodynamic Function Increased arterial stiffness, a measure of arterial wave reflection that is closely related to aortic stiffness, has been found in smokers and passive smokers. [76],[77] This effect on arterial stiffness occurs very quickly in both active and passive smokers. [78],[79] There is evidence of elevated levels of C-reactive protein (CRP), fibrinogen, and interleukin-6, leucocytosis and altered rheologic, coagulation and endothelial function markers like hematocrit, blood and/or plasma viscosity in chronic cigarette smokers. [25] Extracardiac Vascular Disease Tobacco smoking noticeably accelerates atherosclerosis in the abdom-inal aorta, and occlusive disease of its branches is also increased. Abdominal aortic aneurysm, peripheral vascular disease, and renal artery stenosis are increased in smokers. [33],[80] Moreover, smoking is an important cause of stroke. [69] Erectile dysfunction, resulting from endothelial dysfunction and atherosclerosis, has been associated with cigarette smoking and improvement of impotence has been observed with smoking cessation. [81] Interaction of Smoking with Other Risk Factors for CVD The cardiovascular risk imposed by smoking is magnified by the concomitant presence of several other coronary risk factors. Tobacco smoking alone imposes a risk for CVD that is independent of other risk factors. However, when another risk factor (e.g., hypertension or high cholesterol) is present in a smoker the risk of CVD is further increased. These observations are confirmed from the multinational INTERHEART study. [40] Smoking Cessation and Reduction of Cardiovascular Disease Risk Smoking cessation after the development of symptomatic CAD reduces the risk of mortality. Although the risk of CAD after smoking cessation drops by approximately 50% one year after cessation, it approaches that of a person who has never smoked within three to four years. [35] The benefits of quitting on CAD risk are not limited to younger smokers. Even individuals older than 60 years experience significantly reduced CAD risks after smoking cessation. [35] Smoking cessation also confers substantial benefits on people with serious heart disease. [82] Quitting smoking reduces the risk of all-cause mortality by about 29% among patients with established CAD. [83] Cessation in smokers with heart failure reduced mortality, [84] by as much or more than treat-ment with beta-blockers, [85] aldosterone inhibitors, [86] or angiotens in converting enzyme inhibitors. [87] Further epidemiologic and genetic studies are essential to assess the role of smoking itself and possible gene/environment interaction in initiation and development of smoking-induced health ailments affecting mankind. [25] Smoking cessation should be viewed as therapeutic rather than a preventive intervention, [82] as is treating asymptomatic hypertension. Smoking cessation is highly cost-effective relative to other frequently used treatments. [82],[88] Role of Health Care Providers in Smoking Cessation Physicians can play a vital role in reducing the morbidity and mortality associated with cigarette smoking. Primary care providers/family physicians have multiple opportunities over several years to intervene with their patients who smoke and they are in a unique position to provide smoking cessation advice and treatment. Moreover, because physicians frequently encounter patients in the setting of an acute cardiovascular event, they have the opportunity to take advantage of these "teachable moments," when patients may be most receptive to smoking cessation advice or intervention. [89] The Clinical Practice Guideline on Cardiac Rehabilitation, published by the Agency for Healthcare Policy and Research and the National Heart, Lung, and Blood Institute, recommends the inclusion of smoking cessation interventions as an essential component of cardiac rehabilitation programs. [90] Even if the patient is asymptomatic, healthcare providers can link the patient′s smoking to increased risk for disease in the future (e.g., heart disease, if the patient has a family history of early CAD). Finally, the widespread adoption of smoke-free policies in hospitals and other health care institutions provides additional new opportunities for healthcare provider intervention. Although physicians recognize the importance of smoking cessation as a disease-preventive measure, few physicians are confident in their ability to help patients stop smoking. [91] Moreover, less than half of smokers report that they have ever been advised to quit smoking by their physician. [92] There are number of ways by which physicians can help smokers with quitting. Even brief advice has been shown to increase quit rates by 70%. In this regard, physicians can apply the "5A′s" Stratagem as a framework for smoking cessation intervention to their patients in medical care settings. [88] The five steps are enumerated in[Table - 1]: Five A′s: A Strategy for Brief Healthcare Provider Intervention. It is also important to emphasize that although most patients know that smoking increases the risk of disease, the absolute risks are much higher than people believe. [93],[94] Patients should be particularly counseled about the immediate and large effects of both active and passive smoking on the heart and vascular system, because most people think of cancer rather than heart disease when they think about smoking, even though CVD accounts far more smoking induced deaths than cancer. [88] For the patients who are not ready to quit, clinicians should apply "5R′s". [88] They are summarized in [Table - 2]: Enhancing Motivation to Quit Tobacco- the "5 R′s"[Table - 2] Physicians, as healthcare providers, play a crucial role in the prevention of smoking uptake as well as in the treatment of nicotine addiction. Early in 1996 the Agency for Health Care Policy and Research (AHCPR) Tobacco Ces-sation Guideline suggested that even simple advice from a physician is effective in promoting long-term cessation and gave cessation counseling its highest recommendation. [88] Despite this recommendation-and the strong evidence for rapid benefits in terms of CVD-most physicians still fail to intervene to help their patients stop smoking despite overwhelming evidence of this highly cost effective intervention in preventive cardiology is a serious shortcoming in current clinical practice. The real challenge remains integrating this knowledge with routine clinical practice at all levels of medical care system, to make treatment of tobacco addiction as routine and expected as checking blood pressure and treating hypertension when it is identified. [95] It is more relevant in India where resources for tertiary care are limited [96] and smoking cessation should be promoted by one and all. Tobacco Cessation Smoking can be effectively addressed within a busy clinical practice using strategies similar to those used to manage other chronic medical conditions. By opening up a relatively brief dialogue, clinicians can engage and reengage patients in tobacco dependence treatment. Nicotine replacement therapies (e.g., gum, transdermal nicotine, inhaler, and nasal spray), bupropion SR, varenicline, and combinations of these therapies may motivate smokers to make a quit attempt and relapsed smokers to try again. Among behavioral or psychosocial treatments, problem solving and skills training, clinician-delivered social support, and aversive therapies have the most evidence of efficacy. [13] Conclusion Tobacco use in India is complex, but in this review we attempt to highlight the burden of tobacco use in India and its potential impact on cardiovascular health. Smoking contributes to pathogenesis of CVD through a variety of mechanisms and it is also encouraging that tobacco control is the single most cost-effective preventable cause of premature cardiovascular mortality and morbidity. In addition, majority of the adverse health effects of smoking are reversible. Tobacco dependence is considered a chronic disease and cost-effective smoking cessation tools are available. Unfortunately, there is no mechanism in place, especially in India, to help patients towards smoking cessation. In concert with proven strategies of tobacco control, the physicians′ active involvement in tobacco dependence treatment is equally crucial to bring in a reversal in smoking rates across different population settings, including India. References
Copyright 2009 - Indian Journal of Medical Sciences The following images related to this document are available:Photo images[ms09097f2.jpg] [ms09097f1.jpg] [ms09097t2.jpg] [ms09097t1.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}