|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
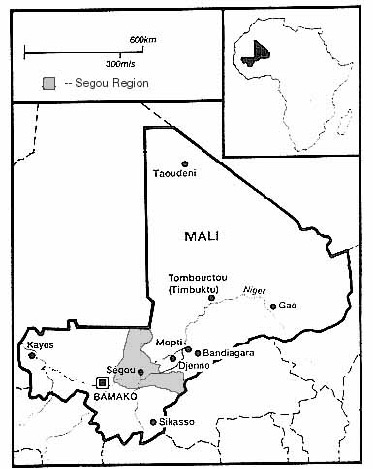
Rural Outreach Program (now African Journal of Food, Agriculture, Nutrition and Development), Vol. 3, No. 1, 2003 EXAMINATION OF URINARY IODINE STATUS FROM A SAMPLE OF MALIAN ADOLESCENT GIRLS EXAMEN DU NIVEAU D'IODE URINAIRE A PARTIR D'UN ECHANTILLON DE FILLES ADOLESCENTES MALIENNES Pawloski LR, Shier NW, Fernandez XE and PL Jamison Lisa R. Pawloski [Corresponding author] Assistant Professor College of Nursing and Health Sciences - MSN 3C4 George Mason University, 4400 University Dr. Fairfax VA 22030, USA Email: lpawlosk@gmu.edu Nathan W. Shier Associate Professor Department of Applied Health Science Indiana University 1025 E. 7th Street, HPER Bldg. 116 Indiana University, Bloomington, IN 47405, USA Email: shier@indiana.edu Xinia E. Fernandez Department of Applied Health Science Indiana University 1025 E. 7th Street, HPER Bldg. 116 Indiana University, Bloomington, IN 47405, USA Email: xfernand@indiana.edu Paul L. Jamison Professor Department of Anthropology 701 E. Kirkwood Dr., Student Bldg. 130 Indiana University, Bloomington, IN 47405, USA Email: jamison@indiana.edu Code Number: nd03004 ABSTRACT Iodine deficiency disorders are common throughout the developing world, yet they are considered one of the most preventable causes of mental retardation. Iodine deficiency has tremendous consequences on women and girls and can not only impair a woman's reproductive health, but it also has serious consequences for a growing fetus. In pregnant women, this deficiency can lead to congenital hypothyroidism in newborn infants. Congenital hypothyroidism is a disorder associated with a low IQ, deaf mutism, and neurological problems. Many studies have revealed that iodine deficiency is common throughout West Africa. While several of these studies have investigated the prevalence of iodine deficiency among women in West Africa, few have examined the problem among adolescent girls. Thus this study aimed to quantify iodine levels in a representative sample of adolescent girls aged 10 to 15 years from the Segou Region of Mali, West Africa. Casual urine samples were collected, and urinary iodine excretion was analyzed using the Sandell-Kolthoff reaction. Clinical signs of iodine deficiency, the presence or absence of goiters, were noted and ethnographic interviews were conducted to examine dietary behaviors. Mean urinary iodine excretion was 9.3 µg iodine/dl (95% CI 7.6-10.9). Forty girls were iodine deficient (66.6%, 95% CI 53.3-78.3) of whom 19 (31.7% CI 20.3-45.0) showed moderate or severe deficiency. These results show that the majority of these Malian adolescent girls are at a mild to moderate risk for iodine deficiency, however no statistically significant differences were found between girls from the urban and rural communities. These findings suggest that not only can iodine deficiency affect the individual health of these girls, but iodine deficiency can have many ramifications concerning the socioeconomic status of their communities. Because adolescent girls are still growing and preparing to have children, these findings have major implications for their health and the health for their future children. These results provide one of the first analyses concerning iodine deficiency among adolescent girls in Mali. Key words - Iodine deficiency, Mali, nutrition, adolescent girls RESUME Contexte : Les troubles dus à la carence en iode sont courants dans le Tiers-monde. Chez les femmes, cette carence peut conduire à un hypothyroïdisme congénital avec des troubles de croissance chez les nouveaux-nés, associés à un bas Q I et une surdité et aphonie. Mots clefs - carences en iode, le Mali, nutrition, adolescentes IC : Intervalle de confiance INTRODUCTION As many as 800 million people worldwide have some form of iodine deficiency [1]. Iodine deficiency is considered to be the most preventable cause of mental retardation in the world. Iodine deficiency has serious consequences on a growing fetus and can lead to a form of mental retardation, known as congenital hypothyroidism. Congenital hypothyroidism describes a condition in which the affected person has an IQ as low as 20 and can also include deaf-mutism. It is estimated that 20 million people have some degree of brain damage caused by a lack of iodine in the diet during pregnancy [2]. Iodine is part of the thyroid hormones and when deficient, the thyroid gland enlarges to entrap as many particles of iodine as possible. This enlargement causes a goiter, which is the most familiar and obvious sign of iodine deficiency. Iodine has many crucial roles, including the regulation of body temperature, reproduction, growth, the making of blood cells, and nerve and muscle function [2]. Iodine deficiency has a great impact on women of all ages. Primarily iodine deficiency can affect a woman's reproductive health. Iodine deficiency occurs more often in women in the form of goiter, and can first appear during adolescence. Among women, iodine deficiency is most common among adolescent girls and among pregnant women. Most researchers suggest the greatest prevalence of iodine deficiency is due to the greater need for iodine during growth, pregnancy, and lactation [3]. This high prevalence of iodine deficiency among women of childbearing years has great implications concerning the health of their children. Thus an examination of adolescent girls who are often preparing to have children or are already having children may provide some clues concerning intervention methods. It has been estimated that in Africa alone, approximately 227 million people are affected by iodine deficiency, with the majority of the cases being found in western and Central Africa. Of these 227 million, approximately 50 million have goiters, and nearly one million people suffer from some form of congenital hypothyroidism [3]. While the majority of iodine deficiency disorders have been seen in West and Central Africa, there is a growing body of literature suggesting severe problems related to iodine deficiency disorders in South Africa [4,5] and in northern Africa [6]. Deficiencies in iodine have also been correlated with reproductive failure and problems related to pregnancy in West Africa among women of childbearing years [7]. A recent study conducted in Cote d'Ivoire found that iodine deficiency was more common among young women than any other group [8]. The study also revealed that 68% of women of childbearing age had goiters. Latapie, Clere, Beda et al. [9] have reported that up to 80% of the women in the northwestern region of Cote d'Ivoire have goiters, and a study by Asibey-Berko, Amoah, Addo et al. [10] reported the prevalence of goiters among women and children to be as high as 77% in rural eastern Ghana. Kouame, Bellis, Tebbi et al. [11] revealed that women of childbearing years (15 to 45 years) had a higher susceptibility to developing iodine deficiency disorders. Other studies throughout West Africa have revealed similar findings [12,13]. In Mali, as in many countries in sub-Saharan Africa, a woman's worth is often based on the ability to have children. Thus, iodine deficiency not only affects the physical health of a woman and her children, but possibly her emotional health and social standing. Several studies conducted throughout villages in Mali have indicated a high prevalence of iodine deficiency, and endemic goiters are considered to be severe, such that the prevalence of goiters affects between 16% to 90% of some village populations [14,15]. It is believed that the high prevalence of goiters in Mali is primarily due to poor iodine intake. Foods commonly consumed throughout Mali have been shown to be very low in iodine content [15]. For many economic and cultural reasons, Malians rarely consume iodized salt even though it is often readily available. While salt iodization is thought to be one of the most common and effective means used to eliminate iodine deficiency in the world [16], it has not appeared to have as great an effect in Mali because the rate of iodine deficiency still remains high despite some salt iodization programs. Reasons that these programs have not been successful are most likely due to economic and cultural factors. For example, many people in Mali are unaware of such programs and do not want to buy the iodized salt due to its cost. Further, because 90% of iodized salt is imported, some associate iodized salt with western foods which are often avoided [17]. To add to the difficulty in obtaining enough iodine in the diet, Mali is an inland country and the soil content is low in iodine [17] and because of its distance from the ocean, very little seafood (often high in iodine) is consumed. Most of the research concerning iodine deficiency in Mali has been conducted in the Bwa Region in eastern Mali and has examined prevalence of goiter and congenital hypothyroidism. Other means to assess iodine deficiency include biochemical assessment such as examining urinary iodine concentration and determining serum thyroid hormones. Assessing urinary iodine concentration is often preferred to collecting serum thyroid hormones when conducting population studies in the field because it is less expensive and is less complex. This article presents one of the first analyses of urinary iodine concentration from adolescent girls living in the Segou Region of Mali. This article will describe the urinary iodine levels from a sample of Malian adolescent girls living in an urban town, Segou, and a rural village, Dioro. It is hypothesized here that: 1. The Malian adolescent girls will exhibit mild to moderate indicators of iodine deficiency. STUDY SITE AND SAMPLE POPULATION Study Site The convenience sample of adolescent girls ages 10 to 15 years (n = 60) was recruited from schools in an urban town, Segou (n=29), and a rural village, Dioro (n=31). Both of the research sites are located within the Segou administrative region. The Segou Region (see Figure I) is located approximately 200 kilometers north of the capital, Bamako, and is situated primarily along the Niger River. The Segou Region was chosen because it is fairly homogeneous in its geography, environment, ethnic population, language, and religious affiliation. Two sites are compared here, the city of Segou and the village of Dioro. Fig. 1: Map of Mali showing the Egou Region
The city of Segou represents the largest and wealthiest city in the Segou Region. Segou serves as a major trading town between the northern cities and Bamako. The main industry there is a textile factory and a military base. The town is equipped with electricity and running water, yet most people cannot afford these services, and use community pumps for water. There is also a maternity, a hospital, and several pharmacies in town. Bambara is the most prevalent ethnicity (80%) and is the major language spoken in Segou. Dioro, the rural community, is much poorer than Segou and has little industry or business. Most villagers are subsistence farmers. Dioro has fewer schools and health centers and does not have electricity or running water. Ethnically, Dioro is also predominantly Bambara. From discussions with local government officials, people living in Dioro and the town of Segou display many similar cultural characteristics, particularly pertaining to eating and working patterns. Segou exhibits a much higher socioeconomic status as evidenced by its level of industrial development, schools, access to electricity and running water, and health facilities [17]. Sample Population Concerning dietary practices, ethnographic data revealed that most girls from both Dioro and Segou eat three meals a day. Breakfast in Segou usually consisted of a piece of bread, or a millet porridge mixed with sour milk or pancakes made of millet, and coffee. In Dioro, girls mostly reported just eating the porridge. A typical lunch or dinner meal included one small piece of meat, fish, or chicken that was combined in a sauce of a beef based broth (using bouillon cube and water) with baobab leaves or a few boiled vegetables (including carrots, tomatoes, okra, eggplant, onions, and cabbage). The sauce also often included oil, salt, and hot peppers. The sauce was then poured onto a large serving of thick millet porridge or rice. In the villages, dinners and breakfast were often leftovers from the previous day's lunch or dinner. Rice, which is more expensive than millet, was more commonly consumed in wealthier families. Further, while salt is a common ingredient added to the rice and sauce, no families reported using iodized salt in the preparation of foods [17]. Iodized salt is considerably more expensive than the non-iodized salt, because non-iodized salt is widely available in Mali due to the large numbers of local salt mines. The iodized salt is primarily imported from Senegal and Russia. In Mali, men and women eat separately. They each eat from separate common pots and children will usually eat with the women. Food is most often eaten using the hands in which the rice and sauce is rolled into a small ball in the palm of the hand and eaten. Water is also consumed, but usually after the meal. Adolescent girls are often responsible for the preparation of meals and gain additional cooking responsibilities as they grow. Because of the style of eating, it is very difficult to conduct a dietary recall because the researcher cannot measure how much food has been placed on one plate. Further, it is even more difficult to assess diets among adolescent girls because girls tend to snack more frequently as they gain cooking responsibilities. However, Pawloski [17] found a sample of girls from the Segou Region to consume a mean of 2500 kilocalories per day. One other factor that affects the nutrient consumption of adolescent girls in Mali concerns their energy expenditure. Adolescent girls have tremendous amounts of responsibilities that range from gathering wood, to collecting water, to cooking, cleaning, and taking care of children. These workloads in combination with their requirements for growth and development, greatly increase their nutrient needs. Factors that have been shown to decrease their responsibilities include the presence of servants in the family and the ability to attend school [17]. Anthropometric data is presented here to show that according to the World Health Association guidelines [18,19], these girls are considered to be mildly to moderately malnourished, and thus are potentially at risk of micronutrient deficiencies. Earlier research in this community revealed that girls living in the Segou Region have mean z-scores that are below the mean reference population for both height (Mean Height-for-Age Z-score = -.79) and weight (Mean Weight-for-Age Z-score = -1.09). Further, there were statistically significant differences between the urban and rural communities for both height and weight, so that the urban girls were significantly taller and fatter than the rural girls (p < .05 and p< .01 respectively) [19]. "Z" scores are presented here because malnutrition is often defined in terms of z-scores. The value of "z" is the value of the score on the standard normal distribution which is based on samples of healthy well-nourished children. This data again indicate that these girls suffer from both chronic and acute malnutrition [18,19]. MATERIALS AND METHODS Data Collection Casual urine samples were taken from 60 adolescent girls ages 10 to 15 years. Dunn [20] recommends that at least 40 subjects be obtained to determine the mean concentration of urinary iodine in a certain region, thus a sample size of 60 was considered adequate to show a deficiency among adolescent girls in this setting (Segou Region of Mali). Because subjects came from both urban and rural settings, comparisons were made between these two groups. The conditions regarding the urine collection were difficult. For example, no bathrooms were available in the schools, thus make-shift partitions were set up to give girls privacy. The participants were explained the nature of the study and they agreed to participate; however, many girls found it completely absurd and funny that the researcher would want a small sample of their urine, but they would in no way agree to donate a 24-hour sample. Thus while a 24-hour urine collection is more reliable, this was not feasible in such field conditions because girls were not willing to participate in such an intensive data collection procedure. Further, the data was collected during the harvest season when girls have many added responsibilities, and would not have been able to provide a 24-hour urine sample. However, casual samples have been shown to accurately reflect 24-hour collections in population studies [21]. Urine samples were refrigerated and then analyzed at the Nutrition Laboratory at Indiana University, Bloomington, U.S.A. The method used was described by Dunn, Crutchfield, Gutekunst et al. [22] and was adapted and modified from Wawschinek, Eber, Petek et al. [23]. This method has been described as simple, inexpensive, and effective for assessing urinary iodine concentration [24]. It is highly recommended for the detection of iodine deficiency in the field, particularly when compared to the expensive costs and difficulties of collecting serum thyroid hormones and clinical assessment of thyroid size. These other methods require more expensive equipment and skilled technicians. This method was chosen to be done in the United States because the basic equipment was available in the United States and not in Segou, Mali. With future funding, we hope to bring this equipment to Mali and provide local training regarding iodine deficiency assessment and prevention. Dunn's method incorporates the Sandell-Kolthoff reaction in which urine is digested first with chloric acid [22]. The concentration of iodine is then determined from its catalytic reduction of ceric ammonium sulfate in the presence of arsenious acid. A simple spectrophotometer is used to examine the reduction of ceric ammonium sulfate such that the disappearance of the yellow color is proportional to the amount of iodine. A standard curve relating iodine concentration to color was first made from known standards in order to extrapolate the concentration of iodine [22]. The concentration of iodine is recorded in micrograms of iodine per deciliter. While standard purchased samples were used to determine iodine concentration, concentration of iodine was also collected and analyzed from a small sample of Indiana University students to ensure the reliability of the laboratory procedure. The presence of goiters was also noted using the classification system endorsed by the World Health Organization and the International Council for Control of Iodine Deficiency Disorders [20]. Dunn and VanderHaar [20] have defined 5 grades ranging from grade 0 (no goiter) to grade 3, in which the thyroid is greatly enlarged and is visible from about 10 meters. Grade 1A is similar to grade 1B, which indicates that the thyroid is enlarged and visible with the head is tilted back. However in grade 1A, the goiter cannot be seen, but can be felt when palpated [20]. Permission and proper research clearances were obtained prior to our visits from officials in Bamako, Mali and a Human Subjects clearance was obtained from the Indiana University Human Subjects Committee. RESULTS For the total sample (n=60), Table 1 indicates the mean urinary iodine excretion was 9.3 µg iodine/dl (95% CI 7.6-10.9). For the rural sample (n=31), the mean urinary iodine excretion was 9.1 µg iodine/dl (95% CI 6.8-11.4) and for the urban sample (n=29), the mean urinary iodine excretion was 9.5 µg iodine/dl (95% CI 6.7-12.2). While the urban sample had a mean urinary iodine excretion that was higher than the rural sample, oneway analysis of variance revealed this relationship was not statistically significant (p = 0.83). No differences were found between the urban and rural samples. Yet, there was a trend towards lower urinary iodine in the rural sample. Also, observations for clinical signs of iodine deficiency revealed that three rural girls showed small goiterous growths of Grade 1B using the classification system endorsed by the World Health Organization and the International Council for Control of Iodine Deficiency Disorders, whereas no goiters were observed in the urban girls. However, the study lacked the statistical power to detect anything other than very large differences. Given the results, the study has at most a 22% power to detect mean differences of 2 micrograms and a 43% power to detect differences of 3 micrograms between groups. Table 1 Mean urinary iodine concentrations of Malian adolescent girls
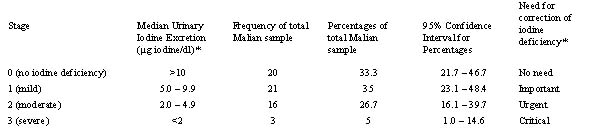
(Urban/Rural: Oneway ANOVA, F = .049, p = .826 Normal values for iodine are greater than 10 µg iodine/dl, while a range of 5-9.9 µg iodine/dl suggests a mild deficiency, 2 - 4.9 µg iodine/dl indicates a moderate deficiency, and values less than 2.0 µg iodine/dl suggest a severe deficiency in which the need for intervention is critical [3]. Table 2 demonstrates that 33.3% (95% CI 21.7-46.7) of the girls had normal amounts of iodine. However, 35% (95% CI 23.1-48.4) exhibited a mild deficiency, 26.7% (95% CI 16.1-39.7) were shown to be moderately deficient and 5% (95% CI 1.0- 14.6) were severely deficient. Table 2 Frequency of urinary iodine excretion at each stage of severity
(*Dunn JT, Crtuchfield HE, Guteknst R and AD Dunn Two simple methods for measuring iodine in urine. Thyroid 1993;3:119-123) DISCUSSION The results indicate that iodine deficiency does occur among both urban and rural adolescent girls in the Segou Region of Mali. While very few of these girls exhibit any clinical symptoms of iodine deficiency, the urinary iodine analyses suggest that many girls are at risk and are in need of intervention. Although rural girls have overall lower urinary iodine values than their urban counterparts, the difference between the two groups was not statistically significant. Perhaps, while socioeconomic indicators are greater in the urban area than in the rural area, this data might suggest that access to and consumption of iodine in both the rural and urban areas are quite similar and are not as affected by economic differences between the rural and urban areas. Thus, this data may suggest that in Mali, socioeconomic status does not have a great bearing on iodine status. Further, perhaps the comparisons between the urban and rural samples suggest that the two communities are much more similar regarding environmental conditions and traditional eating patterns. While Segou is a larger and wealthier community than Dioro, both towns lie next to the Niger River. All of the girls in the study attended school and reported having similar diets and responsibilities [17]. Pawloski [17, 19] reported recently that the adolescent girls living in an urban setting in Mali were taller and heavier, fatter and more muscular than their counterparts living in the rural setting, and these differences were shown to be statistically significantly different. Thus, it was hypothesized in this paper, that urban girls would also show improved indicators of iodine status. While perhaps girls living in the urban environment consume nutrients which more greatly affect growth and development, both urban and rural environments appear to be similarly affected by deficiency in iodine. Earlier studies have shown a high incidence of iodine deficiency in Mali, but none have examined adolescent girls. This data suggests that these girls are at risk from complications of iodine deficiency and because they are preparing for marriage and childbirth, their future children may also be at great risk for congenital hypothyroidism. Congenital hypothyroidism is not uncommon in Mali and one study has shown it to have a prevalence of close to 1.2% in eastern Mali [14]. Adolescent girls are even at greater risk because they are still growing and have therefore greater iodine needs. Malians in general are at high risk of iodine deficiency because of the lack of iodized salt in the diet, low amounts of iodine in the soil, and low intake of sea fish. Malian adolescent girls primarily eat a meal that is high in rice and millet with a small amount of sauce that includes boiled vegetables, and small pieces of meat. While salt is added to most foods during preparation, it is rarely iodized. Malians also commonly add bouillon cubes (Maggi Cube) to prepare sauces. Although these cubes do not contain iodine, many relief workers have suggested that because these are so commonly consumed, iodizing Maggi Cubes could have a significant effect on the occurrence of iodine deficiency. In most urban areas in the Segou Region, iodized salt is readily available due to recent governmental efforts to try to reduce the prevalence of iodine deficiency. Ethnographic evidence revealed that many people did not want to buy iodized salt because not only was it too expensive, but many people viewed it as a kind of "western" food and felt it was unnecessary. The price of iodized salt in Mali is approximately $4.00 US per kg and the price of uniodized salt in Mali is approximately $.50 US per kg [12, 13]. Further, in villages, salt was often traded for other items rather than purchased. Many Malians said that westerners eat over-priced foods that are not necessary to live, and thus they avoided them. Interestingly enough, iodized salt is manufactured in nearby Senegal and a new plant is being constructed in Bamako, the capital, to iodize salt, however iodized salt still continues to be imported. Other factors that contributed to people not consuming iodized salt included the lack of education. It was observed that many projects had been conducted all over Mali which ranged from cost sales of iodized salts from United States Peace Corps volunteers to non governmental organization education programs to government sponsored oral supplementation programs. Further UNICEF is providing education programs regarding iodine deficiency prevention [13]. While most of these programs do give instruction on the importance of consuming iodized salts, many people in Segou and in surrounding villages were unaware of the connection between goiters, cretinism and iodine. Further, some participants revealed that many people with goiters did not want to talk about iodine deficiency or participate in studies which examine the goiters because they were embarrassed by and ashamed of them and did not want to draw attention to them. Other than salt fortification and nutrition education programs, several other kinds of intervention programs have been set-up throughout Africa to try to reduce the prevalence of iodine deficiency. One program that has shown success in the Central African Republic has been the combination of an iodine education project with the iodinization of well water within the communities [25]. Even with these various fortification programs, there are risks of over-consumption of iodine leading to hyperthyroidism if these programs are not safely monitored [26]. Further, some studies have shown that iron deficiency limits the successfulness of these intervention programs because iron deficiency can affect thyroid metabolism [27]. It is important to recognize that while most of these girls are mildly deficient, they and their future children, are still at risk for health complications related to iodine deficiency disorders. In Mali, having healthy children is an important part of life because children contribute tremendously to the domestic needs of a household. A woman who has few children has more domestic responsibilities. More importantly, however, a woman's worth is often based on the fact that she can bear healthy children. A woman who has no children may be divorced and may have no support system later on in life [28]. Iodine deficiency, as with malnutrition in general, can also play a large role concerning the socioeconomic situation of a community. Studies such as those conducted by Greene [29] in Ecuador showed villages which reported low frequencies of iodine deficiency were much better off economically than when compared to villages reporting high rates of iodine deficiency. Greene [29] also showed that even mild deficiencies of iodine affect quality of life within a community and ultimately the economic success of a community. Dunn [3] reported that iodine deficiency can affect the people's work output because those that have iodine deficiency are less active and mentally slower. These effects can cause a shift in the labor force, in which there are fewer individuals available to do work. Dunn [3] presented data from the effects of an iodine deficiency intervention in China and revealed that ten years after effective iodine supplementation, the community intervened had a dramatic decrease in school failure rate, and the per capita income raised from $43 U.S. to $550 U.S. [3]. Thus, not only does iodine deficiency affect the individual health of these Malian adolescent girls, but iodine deficiency can have many ramifications concerning the socioeconomic status of their communities. Because iodine deficiency can affect mental processes, these girls are at a greater risk of doing poorly in school. Further, these communities rely tremendously on the labor from adolescent girls. In Africa, women do approximately 90% of the agricultural labor requirements, and in Mali, girls participate as greatly as adult women. Thus iodine deficiency may impact agricultural production as well. This data reveals that iodine deficiency disorders do exist among adolescent girls in the Segou Region of Mali. Further, they appear to impact on both urban and rural areas, and do not more greatly affect rural girls as originally hypothesized. Because adolescents are still growing and preparing to have children, this micronutrient deficiency is not only a concern among these girls, but for the health of their future children. This research is also critical to the understanding that interventions to reduce the prevalence of iodine deficiency disorders should not only involve the adult community but also include adolescents. CONCLUSION The data presented in this study reveals that Malian adolescent girls from the Segou Region are at risk from iodine deficiency. The urinary iodine excretion data suggested about one-third of these girls are mildly at risk and one-third are at moderate to severe risk. Because they are preparing for marriage and childbirth, lack of iodine can put their future unborn children at great risk for congenital hypothyroidism. Although iodine deficiency is unheard of in the developed world because of the success of iodized salt programs, programs such as these have not been as effective in Mali. It is believed that many factors contribute to iodine deficiency in Mali including poor iodine content in foods and lack of acceptance of iodized salt. Thus these results suggest that there is a need to provide intervention programs that include adolescent girls. Education programs are needed to make people aware of the causes and problems associated with goiters and congenital hypothyroidism. Further, while iodized salt programs have not been successful throughout the Segou Region, perhaps other methods such as iodine tablets, iodization of water, or fortification of commonly used foods, like Maggi Cubes may provide a means to reduce the prevalence of iodine deficiency. ACKNOWLEDGEMENTS This study was performed as part of research for a PhD dissertation in the Department of Anthropology at Indiana University. This work was supported by a Fulbright IIE grant as well as a grant-in-aid from the Research and University Graduate School at Indiana University. I would like to thank the co-authors for their collaboration and input. Finally, I am grateful to Moussa Diarra, my research assistant in Mali and to Dr. Alyce Fly for helping to collect the control urine samples from Indiana University students. REFERENCES
Copyright 2003 - Rural Outreach Program |
| |||||||||