 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
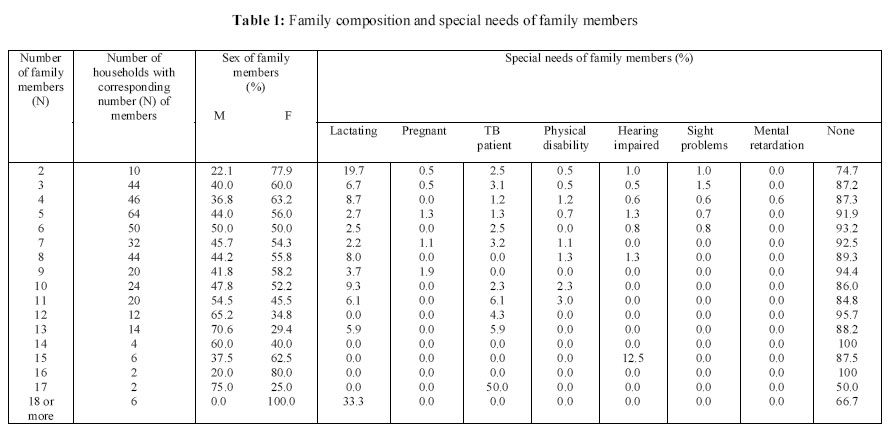
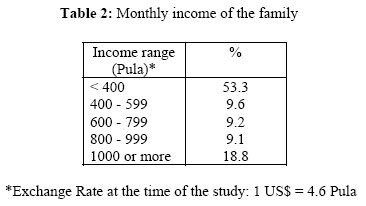
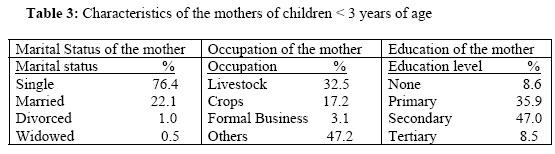
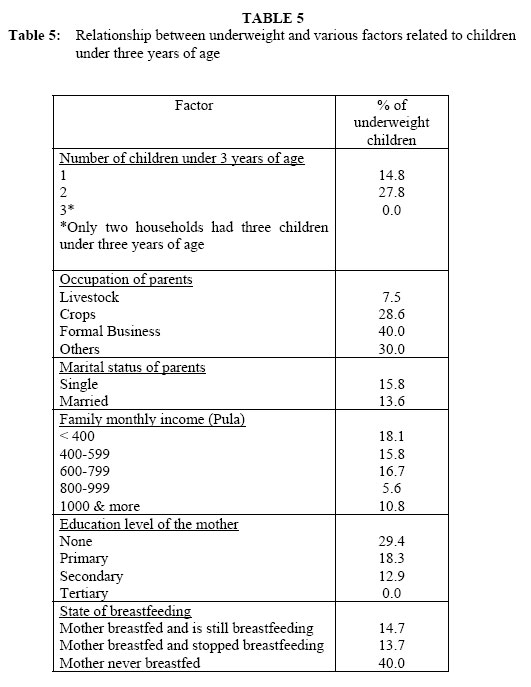
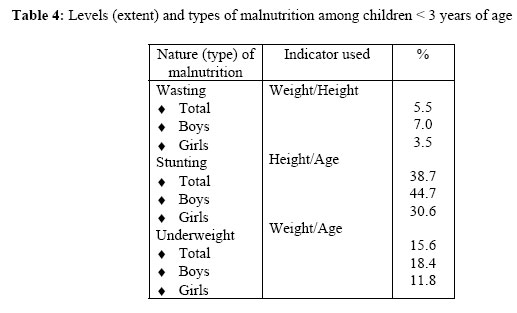
African Journal of Food Agriculture Nutrition and Development, Vol. 6, No. 1, 2006 FACTORS AFFECTING PREVALENCE OF MALNUTRITION AMONG CHILDREN UNDER THREE YEARS OF AGE IN BOTSWANA ETENDUE ET TYPES DE MALNUTRITION ET LES FACTEURS Y RELATIFS CHEZ DES ENFANTS DE MOINS DE TROIS ANS AU BOTSWANA RÉSUMÉ Salah E.O. Mahgoub*1, Maria Nnyepi2, Theodore Bandeke3 *Corresponding Author Code Number: nd06006 ABSTRACT Malnutrition affects physical growth, morbidity, mortality, cognitive development, reproduction, and physical work capacity, and it consequently impacts on human performance, health and survival. It is an underlying factor in many diseases for both children and adults, and is particularly prevalent in developing countries, where it affects one out of every 3 preschool-age children. A well-nourished child is one whose weight and height measurements compare very well with the standard normal distribution of heights and weights of healthy children of the same age and sex. Factors that contribute to malnutrition are many and varied. The objective of the present study is to evaluate the level of malnutrition and the impact of some socio-economic and demographic factors of households on the nutritional status of children under 3 years of age in Botswana. Factors included: the number of children under 3 years of age in the family, occupation of the parents, marital status, family income, parental education, maternal nutritional knowledge, residence location (urban or rural), gender, and breastfeeding practices. The study was a cross-sectional descriptive survey using a structured questionnaire and measurements of weight and height. Four hundred households and mothers of children under three, representing the 23 Health Regions of Botswana, participated in the study. Reference standards used were those of the National Center for Health Statistics (NCHS). EPI Info software (version 5) was used for data entry and analysis. The results show that the level of wasting, stunting, and underweight in children under three years of age was 5.5 %, 38.7 %, and 15.6 % respectively. Malnutrition was significantly (p < 0.01) higher among boys than among girls. Underweight was less prevalent among children whose parents worked in the agricultural sector than among children whose parents were involved in informal business. Children brought up by single parents suffered from underweight to a significantly (p < 0.01) higher level than children living with both parents. The prevalence of underweight decreased significantly (p < 0.01) as family income increased. The higher the level of the mother’s education, the lower the level of child underweight observed. Breastfeeding was found to reduce the occurrence of underweight among children. The study findings imply that efforts for redressing child undernutrition issues in Botswana should focus on factors associated with development outcomes such as maternal income, maternal education, and the creation of employment or economic engagements that do not compromise important child care practices such as breastfeeding. Key Words: Child Malnutrition, Socio-economic Factors, Breastfeeding, Botswana, Pre-school Children La malnutrition affecte la croissance physique, la morbidité, la mortalité, le développement cognitif, la reproduction et la capacité du travail physique, et par conséquent elle a un impact sur la performance humaine, la santé et la survie. Elle constitue également un des principaux facteurs qui sont à l’origine de beaucoup de maladies aussi bien chez les enfants que chez les adultes, et elle est particulièrement prévalente dans les pays en développement où elle affecte un enfant sur trois en âge préscolaire. Un enfant bien nourri est celui qui a des mesures pondérales et des mesures de la taille qui se comparent bien avec la répartition normale standard de la taille en hauteur et des poids des enfants en bonne santé de même âge et de même sexe. Les facteurs qui contribuent à la malnutrition sont nombreux et variés. L’objectif de la présente étude est d’évaluer le niveau de la malnutrition et l’impact de certains facteurs socio-économiques et démographiques des ménages sur l’état nutritionnel des enfants de moins de 3 ans au Botswana. Ces facteurs sont notamment le nombre d’enfants de moins de 3 ans dans la famille, l’occupation des parents, l’état civil, le revenu familial, le niveau intellectuel des parents, les connaissances de la mère en matière de nutrition, le lieu de résidence (urbain ou rural), le genre, les pratiques d’allaitement. Cette étude était une enquête transversale descriptive qui s'est déroulée au moyen d’un questionnaire structuré et par des mesures du poids et de la taille en hauteur. Quatre cent ménages et mères d’enfants âgés de moins de trois ans, représentant les 23 régions sanitaires du Botswana, ont participé à cette étude. Les normes de référence utilisées étaient celles du Centre National des Statistiques Sanitaires (National Center for Health Statistics (NCHS)). Le logiciel EPI Info (version 5) a été utilisé pour l’enregistrement et l’analyse des données. Ces résultats montrent que le niveau d’amaigrissement, du retard dans la croissance et de l’insuffisance pondérale chez des enfants de moins de trois ans était de 5,5 %, 38,7 %, et 15,6 %, respectivement. La malnutrition était beaucoup plus prononcée (p < 0,01) chez les garçons que chez les filles. L’insuffisance pondérale était moins prévalente chez les enfants dont les parents travaillaient dans le secteur agricole que chez les enfants dont les parents étaient impliqués dans des affaires informelles. Les enfants élevés dans des familles monoparentales souffraient de l’insuffisance pondérale jusqu’à un niveau beaucoup plus élevé (p < 0,01) que chez des enfants vivant avec les deux parents. La prévalence de l’insuffisance pondérale diminuait sensiblement (p < 0,01) au fur et à mesure que le revenu familial augmentait. Plus le niveau intellectuel de la mère était élevé, plus diminuait le niveau de l’insuffisance pondérale observée. Il a été prouvé que l’allaitement maternel réduisait l’apparition de l’insuffisance pondérale chez les enfants. Les résultats de l’étude impliquent que les efforts visant à redresser la sous-alimentation des enfants au Botswana devraient être axés sur des facteurs associés aux résultats du développement, lesquels facteurs ne compromettent pas d’importantes pratiques des soins de l’enfant telles que l’allaitement maternel. Mots-clés: Malnutrition infantile, facteurs socio-économiques, allaitement maternel, Botswana, enfants d’âge préscolaire. INTRODUCTION The effects of malnutrition on human performance, health and survival have been the subject of extensive research for several decades and studies show that malnutrition affects physical growth, morbidity, mortality, cognitive development, reproduction, and physical work capacity [1]. Malnutrition is an underlying factor in many diseases in both children and adults, and it contributes greatly to the disability-adjusted life years worldwide [2]. Malnutrition is particularly prevalent in developing countries, where it affects one out of every three preschool-age children [3]. A well-nourished child is one with access to adequate food supply, care and health. Such a child will have weight and height measurements that compare very well with the standard normal distribution of heights (H) and weights (W) of healthy children of the same age and sex. Thus, the best way to evaluate the nutritional status and overall health of a child is to compare the child’s growth indices with the set cut-off points in the standard normal distribution of well nourished children that are associated with adequate growth [4]. Factors that contribute to malnutrition are many and varied. The primary determinants of malnutrition, as conceptualized by several authors relate to unsatisfactory food intake, severe and repeated infections, or a combination of the two [5, 6, 7]. The interactions of these conditions with the nutritional status and overall health of the child -and by extension - of the populations in which the child is raised have been shown in the UNICEF Conceptual framework of child survival [5]. Briefly, the model characterizes the correlates of malnutrition as factors that impair access to food, maternal and child care, and health care. It is these very factors that impact the growth of children. Consequently, the assessment of children’s growth is a suitable indicator for investigating the wellbeing of children, and as well as for examining households’access to food, health and care [4, 5]. The objective of the present investigation is to evaluate and report on the levels of the three commonly-used indicators of malnutrition (wasting, stunting and underweight) among children below the age of three years in Botswana, and analyse some of the factors that previous studies suggest are correlates of malnutrition. These will include the child’ birth-weight, breastfeeding patterns and duration type and frequency of food intake, especially protein-energy rich foods, family headship, parental education, maternal nutritional knowledge, residence location (urban or rural), age, and gender [8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20]. The results may help in the formulation of appropriate policies aimed at addressing factors affecting malnutrition among children in Botswana. It is hoped that relevant interventions would then be designed with the view of reducing the incidence of malnutrition in children. METHODS Study design. This study was a cross-sectional descriptive survey using a structured questionnaire and measurements of weight and height to determine the nutritional status of children aged 0 to 3 years. It was carried out in four districts of Botswana. Sampling. Sampling took into account all the 23 health regions in the country. The regions with similar characteristics, such as eating habits, ecological conditions, cultural values and activities, were grouped together. The total number of such regions was eight. One district was randomly selected from each of the eight regions. Out of these eight districts four were randomly selected. The selected districts were; Gaborone, Kweneng, Maun and Tutume. Two study sites, in both urban and sub-urban areas, were chosen in each district using the modified EPI cluster method. The sampling plan was designed to reach 50 households, having children below three years of age in each of the sites. All households with children under three years of age were included in the study. All such toddlers in the eligible households were included. Children who were visitors and were found to have stayed less than one month were excluded from the study. A focused group meeting was held with 8 - 10 respondents in each site. This group included key informants such as the Chief, the Village Development Committee (VDC) Chair, the Councilors of the area, mothers and the stakeholders from relevant government ministries such as agriculture and water development. Procedure. The research was approved by the ethical committee of the University of Botswana and letters of request to conduct the study were sent to the respective Senior District Medical Officers. Structured interviews were conducted using pre-tested questionnaires administered to heads of households. The questionnaire covered demographic information, breastfeeding practices, socio-cultural and economic factors and anthropometric data. Weights and heights of all eligible children were measured using weighing scales and height measuring boards. The research assistants were trained in basic interviewing techniques and in taking anthropometric measurements. The questionnaire was pre-tested for flow of questions and for validity. Data collection period lasted 26 days. The dependent variables for this study were the three anthropometric measurements: height-for-age (H/A), which indicates the level of stunting, weight-for-age (W/A), which indicates the level of underweight, and weight-for-height (W/H) which indicates the level of wasting. The independent variables were: education of the mother, family income, breastfeeding, number of children under three in the family, parents’ occupation, and marital status of parents. Reference standards used were those of the National Center for Health Statistics (NCHS). Each of the three nutritional status indicators are expressed in standard deviation units (z-scores) from the median of this reference population [3]. Data analysis. Data entry and analysis was performed using the EPI Info (version 5) computer software package. RESULTS Characteristics of the households Demographic and economic properties of the 400 households, which participated in the study are given in Tables 1 and 2. As Table 1 shows, two hundred and eighty (70 %) of the households studied had 3 - 8 members, with 5 being the most common number of family members. The percentage of female members in the households tends to be higher (52.2 % - 77.9 %) among households with smaller number of members (2 - 10). Male members were generally more than females among households with larger number of members (11-17). A high percentage (50 % - 100 %) of family members did not have special needs. Among those with special needs, lactating mothers formed the largest group, and TB patients came second. Mental retardation was the least reported special need, almost exclusively 0 %. Pregnancy, physical disability, hearing impairment and sight problems occurred to a low extent (mostly none or as single digit percentages). HIV infection was not checked since it is still a sensitive issue. Data given in Table 2 indicate that a little more than half (53.3 %) of the households studied, had monthly incomes below 400 Pula (equivalent to US $87), which was the lowest income range in the study. This puts them among poorer sectors in the society. The majority of households (88.6 %) had only one child under three years of age. Households with two and three children who were under three years of age constituted 10.3 %, and 1.1 % of all households studied, respectively. Characteristics of mothers of the children < 3 years of age Figures in Table 2 indicate that a high percentage (76.4 %) of the mothers participating in the study were single as compared to 22.1 %, who were married. Nearly half (49.7 %) of mothers work in the agricultural sector with 32.5 % of them involved in livestock production and 17.2 % in crop production. The rest work in formal business (3.1 %) or informal business sector (47.2 %) like transport, fisheries, beer selling, or traditional brewing. Data in Table 2 also shows that a high proportion (82.9 %) of the mothers had either primary (35.9 %) or secondary (47.0 %) level of education. Few mothers had tertiary education (8.5 %) or no education (8.6 %). Malnutrition among children < 3 years of age: levels and relationships Results of the study on the nutritional status of children < 3 years of age, the level of malnutrition based on the three indicators (W/H, H/A, and W/A), and the differences between male and female children is summarized in Table 3. The results show that the level of malnutrition among children under three years of age was 5.5 % (wasting), 38.7 % (stunting) and 15.6 % (underweight). All the three types of malnutrition were significantly (p < 0.01) more prevalent among boys than among girls. Results in Table 5 show that the percentage of underweight children among households with two children under three years old (27.8 %) was significantly (p < 0.01) higher than the percentage of underweight children among households with one child (14.8 %). Table 4 also indicates that underweight occurred to a lesser extent among children whose parents work in agriculture (7.5 % for parents involved in livestock and 28.6 % for parents working in crops) than among children whose parents were involved in informal business (40.0 %). Children in single-parent households suffered from underweight to a significantly (p < 0.01) higher level (15.8 %) than children brought up by both parents (13.6 %) (Table 4). The results in Table 4 also indicate that the incidence of underweight among children decreased significantly (p < 0.01) as income increased (18.1 % among households with income less than P400 [equivalent to US$ 87] and 5.6 % among households with income range of P800-999 [equivalent to US$ 174-217]). However, the percentage of underweight children rose again among households with incomes higher than P1000 [equivalent to US$ 218] (10.8 %). The results in Table 4 show a strong relationship between the increase in the level of education of the mother and the decrease of underweight among children. There were significant differences (p < 0.01) between each two consecutive levels of education (29.4 % for no education; 18.3 % for primary education, 12.9 % for secondary education and 0.0 % for tertiary education). Prevalence of underweight among children who were breastfed occurred to a substantially (p < 0.01) lower level (14.7 % and 13.7 %) than among children who were never breastfed (40.0 %) (Table 4). There was no significant difference (p < 0.01) between the levels of underweight among children who were breastfed for a period of time and those for whom breastfeeding was stopped (13.7 %) and among those who were still breastfed (14.7 %). DISCUSSION The present study reports on the level of malnutrition and the impact of some socioeconomic and demographic characteristics of households on the nutritional status of children under-three years of age in Botswana. Four hundred households and mothers of under-three children, representing the 23 Health Regions of Botswana, participated in the study; hence the study may be regarded as a reasonable reflection of the nutritional status of children under-three years old country-wide. A number of similar studies have been conducted in various parts of the world [12, 20, 21, 22, 23, 24]. The study reveals that malnutrition is a problem that affects 5.5 % (wasting), 38.7 % (stunting), and 15.6 % (underweight) of children under three years of age in Botswana. The results of a number of studies that show the levels of malnutrition in Botswana are reported in the literature [17, 25, 26, 27, 28, 29]. Overall, a comparison of observations from these reports indicates that the prevalence of malnutrition in Botswana, though still a problem, has declined somewhat since the late 1980s. The reports also suggest that the risk for undernutrition differs across population groups of children, with children in rural areas being at a higher risk. Some of these studies report malnutrition in general without giving details of the three indicators [28]. Other studies give figures for specific indicators of malnutrition in children under five years of age and not for children under three years of age [26, 27]. These results cannot be objectively compared to the results of the present study. A few studies provide enough detail for estimates of stunting, underweight and wasting in children under 3 years of age to be determined [17, 21, 29]. Of these, the levels of underweight reported, 17.3 % and 16.2 %, respectively, are the two most comparable to the levels found in the present study (15.6 %) [17, 21]. With regard to wasting, the level found in the present study (5.5 %) is lower than that reported (8.5 %) [21]. On the other hand, the level of stunting found in the present study (38.7 %) is higher than the level (27.4 %) reported [17, 21]. The high level of stunting in the present study may have been influenced by the fact that the sample of the present include subjects from Kweneng, a district which has previously been found to have stunting rates as high as 32,1 % for children under 5 years of age [17, 21, 27]. Even in children of ages closer to the under three year age range, Kweneng districts has previously been reported to have stunting prevalence as high as 36.6 % and 22.5 % for children 12 - 23 months and 24 - 35 months of age respectively. Therefore stunting levels reported in this study are not likely to be too far off from the true population estimates. Contrary to an earlier study, conducted in Tanzania among children under four years of age which concluded that males had better nutritional status than females, the current study indicates that the prevalence of all the three types of malnutrition was significantly (p < 0.01) higher among boys than among girls [20]. Within Botswana, this observation agrees with some studies but not with others [27, 29]. Although in some Botswana studies that report different observations, stunting and underweight rates for boys were higher than for girls, only these differences did not reach statistical significance [17, 27]. Further studies are required to definitively explain the relationship between sex and the nutritional status of children in Botswana. Such studies will assist in identifying factors that may be related to this observation and generate information that can inform the development of interventions. In studying the correlates of undernutrition in children under three years of age, our findings revealed that a negative relationship between the number of under three children in the family, family income, maternal education and the nutritional status (underweight) of children exists in this population. The protective effect of the presence of both parents in the family, parental engagement in agriculture compared to informal business such as street vending, maternal education and breastfeeding that was observed in this study may be reflective of the better resources and childcare practices in households with such protective characteristics compared to others. Observations from other studies suggest that economic engagements of parents, especially maternal income is protective against child malnutrition [13, 14]. Such economic engagements are particularly protective if parents have suitable alternative child care [14]. In the absence of suitable child minders, economic engagements that promote extended separation of children from their primary caregivers such as street vending may be detrimental to child survival [14]. The protective effects of breastfeeding on children’s nutritional status observed in this study suggest that breastfeeding is an important part of child care. However, there is need to educate mothers on safe breastfeeding and timely introduction of complementary foods because poor breastfeeding practices such as prolonged breastfeeding or failure to introduce adequate complementary foods as recommended places children at risk for stunting or underweight [12, 22]. Undernourished children were more likely to be breastfed for a longer period (over 12 months) compared to well-nourished children [21, 22]. Additional factors such as poverty and maternal literacy were considered together with breastfeeding, so the observed result may have been due to a combination of these factors [22]. In agreement with previous studies, the present study shows that maternal education is associated with nutritional status [13]. In fact, in some studies the education level of women has been used together with other indicators as a proxy for the relative position of women (women’s social status) in the society. It is argued that women with higher status in the society have the ability to make decisions that improve the nutritional status of children while those with low status do not [30]. CONCLUSIONS In conclusion, the present study confirms the observations of other studies that show higher levels of undernutrition in children under three years from single parent households, households with low earnings, low parental education or households in rural areas [17, 21, 26]. It can also be concluded that the high level of malnutrition observed in this study is unlikely to be attributed to challenges households may have in distributing time and resources between child rearing activities and providing for members with special needs such as members with TB, physical disabilities, hearing or sight problems or mental retardation as these occurred very infrequently in this population. The study findings imply that efforts for redressing child undernutrition issues in Botswana should focus on factors associated with development outcomes such as maternal income, maternal education, and the creation of employment or economic engagements that do not compromise important child care practices such as breastfeeding. Such efforts should also have clearly thought out strategies for targeting children in single parent households and in elucidating factors that place boy children at greater risk for malnutrition compared to girl children. REFERENCES
Copyright 2006 - Rural Outreach Program The following images related to this document are available:Photo images[nd06006t2.jpg] [nd06006t5.jpg] [nd06006t1.jpg] [nd06006t4.jpg] [nd06006t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}