 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
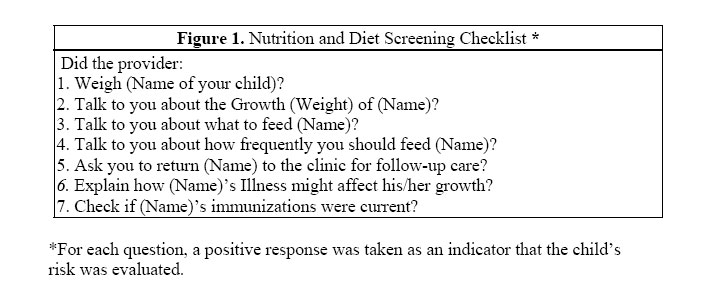
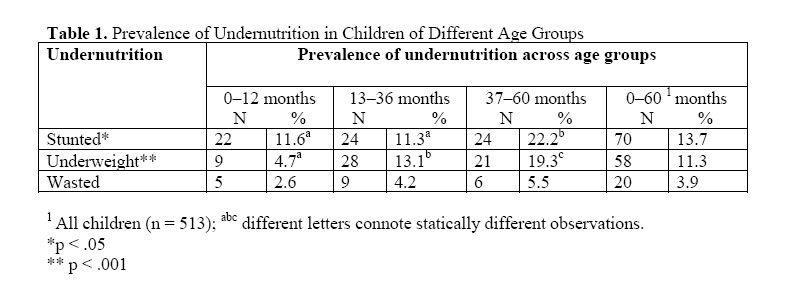
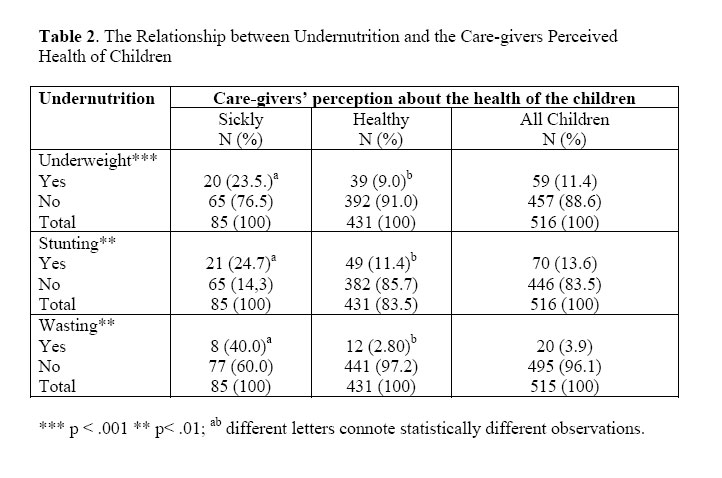
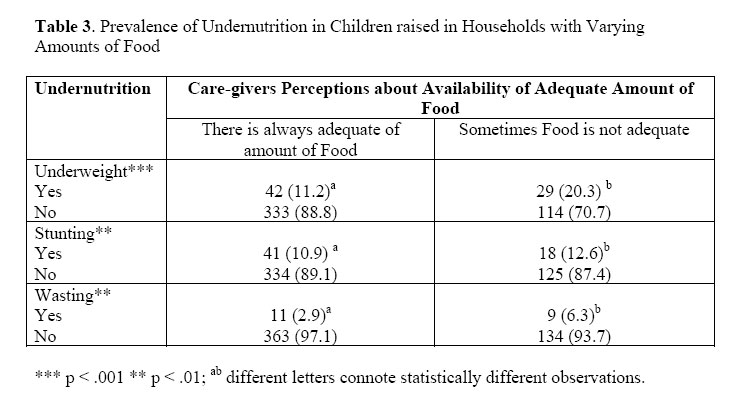
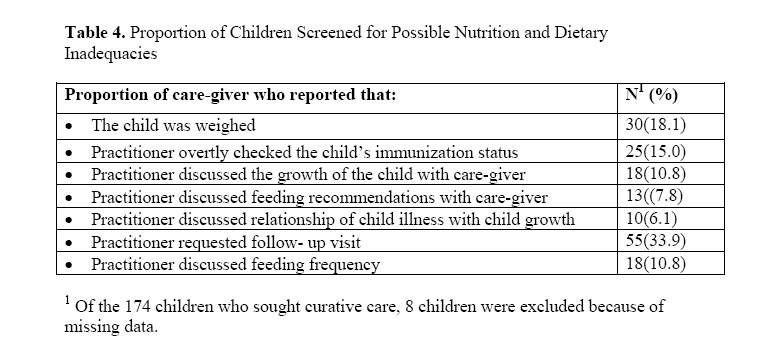
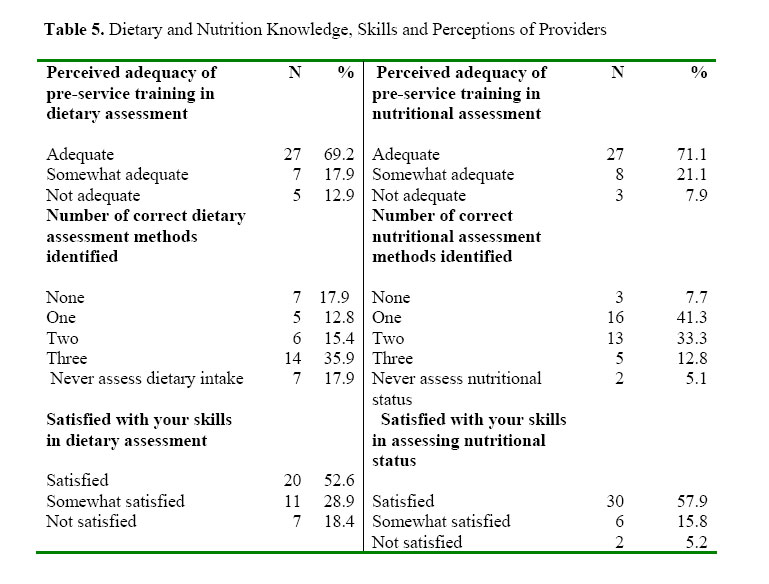
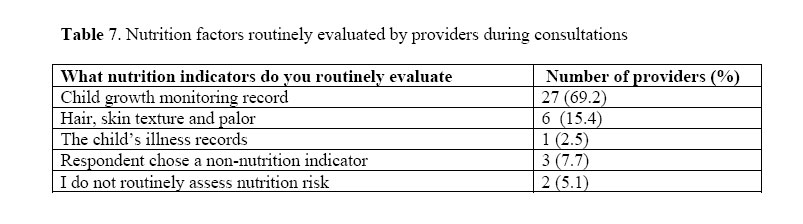
African Journal of Food Agriculture Nutrition and Development, Vol. 6, No. 2, 2006 DIETARY AND NUTRITION SCREENING FOR CHILDREN SEEKING CURATIVE CARE IN HEALTH FACILITIES IN BOTSWANA DÉPISTAGE DIÉTÉTIQUE ET NUTRITIONNEL SUR LES ENFANTS A LA RECHERCHE DE SOINS CURATIFS AUPRÈS DES FACILITÉS SANITAIRES AU BOTSWANA Dr. Maria S. Nnyepi Department of Home Economics Education Private bag UB 00702 Gaborone, Botswana E-mail: nnyepima@msu.edu Code Number: nd06019 ABSTRACTThe extent to which nutrition and dietary screening performed in children seeking curative care in health facilities in Botswana was investigated using a cross-sectional survey design. Dietary screening, illness status, demographic and anthropometric data was obtained from a random sample of 522 children in 13 health facilities through structured interviews and actual anthropometric measurements. Amongst these, caregivers of children seeking curative care (n =174) completed a nutrition and dietary screening checklist designed to establish the proportion of ill children screened. Additionally, a self-administered questionnaire was used to examine the knowledge, attitudes, and perceptions of providers in the study clinics about nutrition and dietary screening and the types of indicators routinely used. Data was collected from all providers (n = 39) on duty. The results show that malnutrition was prevalent, with 13. 7%, 11.3 % and 3.9 % of children estimated to be stunted, underweight and wasted respectively. The prevalence of stunting and underweight was higher (p < .05) in older children (37-60 months), children perceived as sickly, or raised in households with periodic shortage of food compared to children under one year of age, children perceived as healthy or raised in households with adequate amounts of food at all times. Less than 20 % of children who sought curative care were screened for possible compromised dietary intake or nutritional status. Only 18 % of children had their weight measured during consultations. Only 10.8 % of providers were reported to have discussed the children’s growth indicators with care-givers. Similarly, few providers specifically discussed the feeding recommendations (10.8%) and feeding frequency (7.8 %) of children with care-givers. The providers’ knowledge about nutrition and dietary screening was low. Most providers (70 %) perceived their didactic training to be adequate and over half of them were satisfied with their skill level in assessing the dietary intake (53 %) and nutritional status (57.9 %) of children. Fewer providers were able to correctly list three indicators of nutritional status (35.9 %) or dietary intake (12.8 %). Study observations show that a large proportion of children seeking curative care in the health clinics are rarely screened for possible compromised dietary intake and nutrition status. Also, a large number of health providers are not satisfied with their skill level in dietary and nutrition screening. Since nutritional problems are often juxtaposed to health problems, efforts should be taken to integrate nutrition screening into the medical care for under-fives. Key words: Dietary screening, nutrition assessment, Child Survival Programs, malnutrition, under-fives RÉSUMÉ L’étude sur le dépistage diététique et nutritionnel réalisé sur les enfants cherchant des soins curatifs auprès des facilités sanitaires dans les facilités de santé au Botswana a été réalisée grâce à l'utilisation d'un modèle d’analyse transversale. Le dépistage diététique, l’état de maladie, les données démographiques et anthropométriques ont été obtenus à partir d'un échantillon aléatoire de 522 enfants dans 13 centres de santé à travers des entretiens structurés et des mesures anthropométriques réelles. Parmi ces dernières, les soignants des enfants à la recherche de soins curatifs (n = 174) ont complété une liste de vérification pour le dépistage diététique et nutritionnel conçue en vue d’établir la proportion des enfants malades soumis au dépistage. En outre, un questionnaire volontaire a été utilisé afin d’examiner les connaissances, les attitudes et les perceptions des prestataires au sein des cliniques d'études sur le dépistage diététique et nutritionnel ainsi que les types d'indicateurs utilisés régulièrement. Les données ont été recueillies de tous les prestataires (n = 39) de service. Les résultats montrent que la sous-alimentation était prévalente avec respectivement 13,7%, 11,3% et 3,9% d'enfants estimés comme souffrant d’un retard de croissance, d’une insuffisance de poids et d’émaciation. La prédominance du retard de croissance et de l’insuffisance de poids était la plus importante (p <. 05) parmi les enfants plus âgés (37-60 mois), les enfants perçus comme étant malades ou élevés dans des ménages sujets à un manque périodique de nourriture en comparaison aux enfants de moins d’un an, les enfants perçus comme étant sains ou élevés dans des ménages disposant de quantités suffisantes de nourriture à tout instant. Moins de 20% des enfants qui ont cherché des soins curatifs ont été examinés afin de constater une éventuelle consommation diététique compromise ou leur situation nutritionnelle. Dix-huit pour cent seulement des enfants ont été pesés au cours des consultations. Il a été rapporté que 10,8% seulement des prestataires ont discuté avec les soignants des indicateurs de croissance des enfants. De même, peu de prestataires ont discuté en particulier des recommandations alimentaires (10,8%) et de la fréquence de l’alimentation (7,8%) des enfants avec les soignants. Les prestataires disposent d’un niveau faible de connaissances sur la nutrition. La plupart des prestataires (70%) perçoivent leur formation didactique comme étant suffisante et plus de la moitié d’entre eux sont satisfaits de leur niveau de compétence d’évaluation de la consommation diététique (53%) et de la situation nutritionnelle (57,9%) des enfants. Moins de prestataires pouvaient correctement énumérer trois indicateurs de la situation nutritionnelle (35,9%) ou de la ration diététique (12,8%). Les observations de l’étude montrent qu'une grande partie des enfants cherchant des soins curatifs auprès des cliniques de santé sont rarement examinés sur la possibilité d’une prise alimentaire compromise et sur leur condition nutritionnelle. En outre, plusieurs prestataires de santé ne sont pas satisfaits de leur niveau de compétence en matières de dépistage diététique et nutritionnel. Etant donné que les problèmes liés à la nutrition sont souvent juxtaposés aux problèmes de santé, des efforts devraient déployés afin d’intégrer le dépistage nutritionnel aux soins médicaux des enfants âgés de moins de cinq ans. Mots-clés : dépistage, évaluation de la nutrition, Programmes de Survie des Enfants, sousalimentation, enfants de moins de cinq ans. INTRODUCTIONYear 2020 projections suggest that malnutrition will continue to be a significant problem in sub- Saharan Africa [1, 2]. In children under five years, Child Survival Programs have remained the primary framework within which malnutrition and other child survival problems are addressed. These programs have not only been used to tackle malnutrition and childhood illnesses since their offshoot from the more global primary health care approach, but they have also served as a base for the launching of newer strategies such as the Integrated Management of Childhood Illnesses and generated outcome measures for target goals of development programs or objectives [3, 4, 5,6]. Within the Child Survival Programs, the Growth Monitoring Program is credited for facilitating the prevention of malnutrition in children and promotion of nutrition education for care-givers and has, as a result, attracted many evaluation studies [7]. Surprisingly, the findings of these evaluation studies suggest that the benefits of Growth Monitoring Programs are minimal, inconsistent, and at times imperceptible [8, 9, 10, 11]. Hence, the efficacy of growth monitoring in preventing malnutrition has been questioned [8, 9]. Other perspectives suggest that the reported poor efficacy of Growth Monitoring Programs results from the inherent associative problems and not the basic programs [12]. Problems such as the exclusive use of anthropometric measurements—while neglecting other indicators of nutritional status (the presence of illness and the poor dietary practices of children), the lack of adequately trained providers, poor supervision of providers, and the general failure of providers to provide follow-up care for children at risk, compromise comprehensive nutrition risk assessment and administration of timely interventions—both of which are central to a good Growth Monitoring Program [12, 13, 14]. As the debate over the efficacy of the monthly Growth Monitoring Programs continues, the role of the curative component of the Child Survival Programs in addressing malnutrition in children has received less attention. Yet, nutritional problems are often juxtaposed to health problems and very often malnutrition is a predisposing factor in many childhood illnesses [15, 16, 17, 18, 19]. Though often overlooked, curative clinics present providers with opportunities not only to address illnesses, but also to assess malnutrition in children. In fact, if dietary and nutrition screening is performed routinely, curative clinics create more opportunities for screening and timely intervention, because children have more frequent contact with health providers in curative clinics than in preventive clinics. Despite this added advantage that curative clinics offer, the extent to which providers in Botswana take advantage of this opportunity has not been studied. Hence this study was carried out, first and foremost to determine whether dietary and nutrition screening is routinely performed in children seeking curative. Secondly, it attempted to establish whether dietary and nutrition education is routinely offered and thirdly, whether nutrition education, if provided, addressed the recommended dietary intake of children, the feeding frequency and the anthropometric (weight) assessments of children. Lastly, the study also examined the knowledge, attitudes, and perceptions of providers about the provision of nutrition and dietary screening for children seeking care at the curative clinics. METHODSData was obtained from a random sample of 522 children who sought preventive or curative care from 13 health facilities in the greater Gaborone area, and the 39 health providers (nurses) who provided care in the same facilities. Clinics were selected to include the different localities in Gaborone and the surrounding villages. At each clinic, children were selected as they queued for services.All providers on duty at each clinic were enrolled. Children's age, sex, birth weight and the type of care sought was collected through structured personal interviews with primary care-givers. Clinic records were used to verify children's birth dates and weights. Current body weights and heights were measured using the UNICEF solar powered Seca scales, model 871 and a measuring board previously used by the Central Statistic Office [20]. In addition to children's data, all care-givers were asked to answer questions about the general health of the study children, the purpose of the clinic visit and the availability of adequate amounts of food for all household members. Care-givers of children who were seeking curative care (n = 174) were asked to respond to a checklist (Figure 1) of risk indicators for poor nutrition and dietary intake after consultation with health care providers. Data collected through this checklist was used to establish whether providers performed routine nutrition and dietary screening during consultations, as well as the types of dietary and nutrition indicators providers evaluated. Questions in the checklist covered indicators previously shown to be consistent predictors of nutritional status and child survival. These included growth (body weight), diet (the food the children were usually fed and the frequency of feeding), and children's health (care-givers’ perceptions of the children's general health) [13, 15, 19, 21]. Statistical analyses were carried out in SPSS 11.01 and Epi Info 2000. The children’s height-for-age, weight-for-age and height-for-weight Z-scores were generated by Epi Info, and exported into an SPSS spreadsheet for further analysis. SPSS was also used to estimate the prevalence of stunting, underweight and wasting, across children of different age groups. Pearson’s Chi- Square test was used to test the null hypotheses of independence between measures of undernutrition, and the perceived general health of children or adequacy of food for household members. Providers’ knowledge, attitudes and practices A self-administered questionnaire was developed to gather data on providers' knowledge, attitudes and practices about dietary and nutrition screening for children seeking curative care in health clinics in Botswana. Thirty nine (39) providers delivering care to under-five year old children in 13 clinics were asked to participate. Providers were further asked to rate the adequacy of their background training in preparing them to address nutrition issues in under-five year old children and their satisfaction with their skill level in the same area. All but one provider completed the questionnaire. RESULTSOf the 522 children enrolled in the study, 240 (46.0 %) were boys—one-third (174) of whom were established to be seeking curative care. Out of the total number of children participating in the study and seeking preventive/curative care, 148 of them had some form of undernutrition. The prevalence of stunting, underweight and wasting in children seeking curative or preventive care was estimated at 13.7 %, 11.3 % and 3.9 % respectively (Table 1). Children over 12 months of age had significantly higher (p < .05) prevalence of underweight than those 12 months and younger, while children 37 months and older had higher prevalence of stunting than children 0-12 and 13-36 months of age. The prevalence of all forms of malnutrition was higher amongst children who were characterized as being sickly by care-givers (Table 2), or were said to come from households in which the amount of food was often not adequate for all household members (Table 3). 85 care-givers characterized their children as sickly, while 431 characterized their children as being generally healthy. Children perceived by their care-givers to be sick more often had a significantly higher prevalence of undernutrition than children who were perceived to be healthy. The prevalence of underweight (X2 = 12.792; p <. 001), stunting (X2 = 9.22; p < .01) and wasting (X2; 8.2; p < .01) was higher in children whose care-givers perceived to be sick more often than in children who were characterized as being healthy. Similarly, children from households in which the amount of food was at times not adequate for all household members were more likely to be stunted (X2 = 7.2; p < .01) than children raised in households with adequate amounts of food at all times (Table 3). The majority of children who were seen for curative care were not screened for any of the indicators in the Checklist (Figure 1). Of the 174 children seen in curative clinics (see Table 4), 18.1 % were weighed, and providers discussed with care-givers of 10.8 %, 7.8 % and 10.8 % of the children the overall growth of the children, feeding recommendations and feeding frequency respectively. The remaining majority of the children were not evaluated for possible compromised nutrition. Providers’ perceptions about nutrition screeningAll providers had general nursing training from the Institutes of National Health Sciences in Botswana. Most providers (69.2 %) were trained as general nurses only, some (30.8 %) also had additional training in midwifery, family nurse practice, nursing administration and/ or community health. Only four providers were trained as family nurse practitioners and were therefore presumed to be qualified to provide basic curative and preventive primary health care [22]. 82 per cent of providers consulted on ill children daily, while 10.3 % consulted on children at least three times per week. The majority (59.0 %) of providers had been practicing for more than five years (data not shown). Providers in this study differed in their knowledge and perceptions about dietary and nutritional assessment of children (Table 5). All providers reported having been trained in diet and nutrition assessment, but they differed in their perceptions about the adequacy of their didactic training and satisfaction with their current assessment skills. About 70 % of providers perceived that their didactic nursing training adequately prepared them for assessing both the dietary intake (69.2 %) and the nutritional status (71.1 %) of children. About 53 % of providers felt that their skill level in assessing dietary intakes of the under-fives was adequate. More than half of providers (57.9 %) perceived their ability to assess the nutritional status of children to be adequate. All but nine providers reported that they routinely evaluated the dietary intake (n = 7) or nutritional status (n = 2) of children (Table 5). Surprisingly, when asked to list three indicators that they routinely used, only 35.9 % and 12.8 % of providers correctly listed three dietary and nutrition screening indicators, respectively. Seven (18 %) providers could not list even one correct indicator of dietary screening. The most commonly listed indicators of dietary or nutrition screening are listed in Tables 6 and 7 respectively. In screening for possible compromised dietary intake (Table 6), providers enquired about the amount (n = 10) and type (n = 4) of food the child was usually fed as well as the frequency of feeding (n = 4). Most providers (n = 27) used growthmonitoring records to assess the nutritional status of children (Table 7). DISCUSSIONWe found minimal use of routine nutrition or dietary screening in the curative clinics in health facilities. This was the case despite the high prevalence of undernutrition in children seeking care from health facilities. Older children (37-60months) were the most affected (as reflected in Table 1), partly because they are less likely to be still benefiting from breastfeeding and are also more likely to have been exposed to factors that adversely affect nutritional status for a longer duration than children under one year of age, simply because they have lived longer. Nonetheless, malnutrition in all children under five years is still a health concern in Botswana and needs more attention. Most providers reported making efforts to screen children for nutritional and dietary risk, but their efforts were largely inadequate for several reasons. For example, most providers relied only on growth monitoring records to evaluate nutritional risk during illnesses (Table 7). Yet, anthropometric indicators have been found to be less able to reflect changes in nutritional status and morbidity during illness episodes than dietary indicators, such as frequency of intake [13]. It was also evident that several providers lacked the necessary knowledge to conduct good nutrition or dietary screening. As many as nine providers in this study reported using incorrect indicators for dietary intake (Table 6; n = 6) or nutrition (Table 7; n = 3) and some did not routinely screen children for either dietary risk (n = 2) or nutrition (n = 7). Amongst the providers who did not routinely screen children, it is likely that their knowledge, skill level and sensitivity to dietary or nutrition screening were low. We make this argument because even amongst providers who routinely screened children, some providers evaluated incorrect indicators. Observations in this study also suggest that providers do not adequately discuss with care-givers about the nutritional status of their children—as is shown by the growth monitoring records. This is demonstrated by the incongruence between the large percentage of providers (Table 7) who routinely use children’s growth monitoring records to assess the nutritional status of children on one hand, and the lower percentage (Table 4) of care-givers who report that providers discuss with them about their children’s growth records on the other. Since growth monitoring records form the basis of diet and nutrition education and counseling, this lack of communication greatly undermines the objective of keeping growth records. Without their appropriate use, care-givers will be left unaware of both the children’s nutritional status and appropriate dietary interventions. Studies that examined the relationship between providers’ knowledge and delivery of services have shown that knowledge is not always translated into practice [23, 24, 25, 26]. Hence, in this study we did not only rely on providers’ knowledge and attitudes about routine nutrition screening during the provision of curative care. Rather we also used care-givers’ data to establish whether providers obtained minimal information to facilitate the nutrition and dietary screening of children in curative clinics. Even in using this approach, our study still showed that nutrition or dietary screening was seldom performed because most care-givers indicate that providers did not interview or discuss with them the basic aspects of dietary screening. Simple questions that might have generated helpful information for dietary and nutrition screening—such as those in Figure 1—were not asked. CONCLUSIONOur findings suggest that interviewing care-givers can provide valuable information for screening purposes. We found that children who were described by their care-givers as being sick more often, were more likely to have a higher prevalence of underweight and stunting than those who were described as being generally healthy. Furthermore, children in households in which care-givers reported that the amount of food was at times not adequate for all household members were more likely to have a higher prevalence of stunting compared to children in households with adequate amounts of food for all household members at all times. This information can be useful in the routine screening and preventive nutrition interventions in children. The inability of providers to perform nutrition and dietary screening observed in this study exposes a fundamental weakness in the Child Survival Programs. The programs rely on providers’ competence to identify and address the health and nutritional needs of under five year olds at each opportunity of contact. Thus when providers in one clinic (program) miss such an opportunity, as shown in this study, the advantage of pooling several programs (clinics) together under the child survival programs strategy is undermined. Though providers in this study generally did not screen ill children for nutritional risk and provide them with follow-up interventions, nutrition screening through a checklist or other means followed by appropriate intervention in different healthcare settings has been found to be very effective in improving the survival of people at risk in different settings [8, 27, 28, 29]. Finally, our findings suggest that there is limited nutrition and dietary screening in the curative clinic of health facilities in Botswana. With inadequate nutrition screening, the extent to which the curative clinics can contribute to the reduction of malnutrition is greatly compromised. It is recommended that health facilities be assisted to integrate nutrition screening into the medical care of under-fives. Greater emphasis should be placed on the pre- and post-service training of providers in the health facilities and the development of a simple nutrition and dietary screening tool that providers can routinely use in health facilities. AcknowledgementsThis research was funded by the Compton Fellowship for African Dissertations and Dr. Jenny Bond. REFERENCES
Copyright 2006 - Rural Outreach Program The following images related to this document are available:Photo images[nd06019t6.jpg] [nd06019f1.jpg] [nd06019t1.jpg] [nd06019t7.jpg] [nd06019t4.jpg] [nd06019t3.jpg] [nd06019t2.jpg] [nd06019t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}