 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food Agriculture Nutrition and Development, Vol. 7, No. 2, 2007 PROVISION OF VITAMIN A THROUGH UTILIZATION OF LOCAL FOOD MATERIALS IN RURAL PARTS OF WESTERN KENYA Shiundu K.M1, Oiye S., Kumbe M. and R. Oniang'o 1Kennedy M. Shiundu Msc. Nutrition, corresponding author, email: kmshiundu@yahoo.co.uk Code Number: nd07016 ABSTRACT High prevalence and the negative consequences of the deficiencies resulting from inadequate intake of iron, iodine and vitamin A have resulted in focused global efforts to alleviate them. Vitamin A deficiency which has serious consequences can be prevented by consumption of vitamin A rich foods. This study was undertaken to determine the viability of locally available foods in providing vitamin A to the impoverished populations in rural areas of Kenya. A cross-sectional survey was carried out in Butere-Mumias District of Western Province, Kenya from December 2003 to February 2004. The study compared the potential contribution of local foods to the provision of vitamin A, to the diets of children aged 12-71 months in the two divisions of Butere and Khwisero, as based on the Helen Keller International (HKI) method. Vitamin A rich foods consumed in the two study areas are dark green leafy vegetables, kales, papaya margarine, orange/yellow fleshed sweet potatoes, eggs and ripe mangoes. Butere and Khwisero divisions where the study was conducted are adjacent to each other. Butere division had an ongoing nutrition intervention project to promote African leafy vegetables, while Khwisero division did not. Of the 16 clusters surveyed, consumption of vitamin A was insufficient in the six of the eight communities in Butere, and three of the eight communities, in Khwisero. The frequency of consumption of vitamin A-rich foods in the study area fell below the threshold values of the HKI Method. Consumption of these foods was not regular as planting was done on an ad hoc basis especially in Khwisero division in areas which were not reached by the on-going campaign in the Butere division. Vitamin A deficiency was most likely a public health problem in the two divisions. This study recommends increased activities in the area to control vitamin A deficiency, prophylactic vitamin A supplementation and efforts to increase vitamin A consumption. Keyword: Vitamin A deficiency, Vitamin A-rich foods, Helen Keller Method, African dark green leafy vegetables INTRODUCTION
Micronutrient malnutrition is recognized as a serious threat to the health and productivity of people. Deficiencies in three major micronutrients iron, iodine and vitamin A have been of major nutritional concern globally. High prevalence and the negative consequences of the deficiencies resulting from inadequate intake of iron, iodine and vitamin A have resulted in focused international efforts to alleviate them [1]. Many developing countries have developed initiatives to combat vitamin A deficiency problems. Since early 1990s, the main strategy for combating vitamin A deficiency has been to distribute mega-dose vitamin A capsules [2]. Although this initiative is feasible, it is not sustainable considering that it is donor-driven. Given the situation of donor fatigue, alternative sustainable interventions need to be put in place. Food fortification has been found to work, but fortified foods are not in the affordable price range by small-scale farmers and majority of the poor in the developing world. Even the smallest price increase brought about by fortification tends to put off the poorest and yet the most needy . Food-based approaches are sustainable and cost-effective. Rural families grow fruits and vegetables in home gardens to promote diversified diets. Food based strategies are appealing because they can address multiple nutrients simultaneously including energy, protein and various micronutrients. They also have uncontested advantage of allowing for the natural interactions of micronutrients within the same food or meal. Food-based approaches with the main emphasis on foods of plant origin are relatively cheaper and are affordable by the majority of poor people in the developing countries. In Kenya, Vitamin A deficiency has been documented in 11 districts [1]. World Health Organisation (WHO) has also listed Kenya among the 72 countries in the world suspected to have low serum retinol levels [3]. The past demographic surveys show Vitamin A deficiency nationally to be at all-time high at 76 percent [4]. The Kenyan government may have recognized this fact and adopted the theme 'resource mobilization for sustainable development' in its 7th Development plan [3]. More work is still needed in creating awareness on the links between micronutrient adequacy in the population and development. This study was undertaken to determine the viability of locally available foods in providing vitamin A to the impoverished populations in rural areas of Kenya. METHODOLOGY
This was a cross-sectional descriptive study. The food consumption data was collected using food frequency method. Preliminary work was carried out to survey foods commonly consumed in the area through group discussions, informal interviews and market surveys. The main study was performed by use of a structured questionnaire, to determine the sources, and utilization of vitamin A-rich foods in the study area, the frequency of consumption, methods of preparation and forms in which the vitamin A-rich foods are consumed. The study was carried out in Butere division, where African Leafy Vegetables (ALVs) are being promoted by an NGO, Rural Outreach Program and in the adjacent division of Khwisero division, where the ALVs are not promoted. Multistage and cluster-sampling procedure was employed in this study, because it is the most practical and popular way of sampling the population at risk of VAD [5]. For assessment of consumption of vitamin A-rich foods, 16 clusters based on the existing administrative villages were randomly chosen, eight from each randomly chosen location in either the two divisions. In each of these cluster- communities, 50 mothers or primary caretakers of children from one, through to five years of age (12 - 71 months) were considered for interviewing. An attrition of 2 households per village was allowed. Thus, 832 households were visited in total. However, 15 questionnaires were destroyed due to data irregularity leaving 817 questionnaires for analysis (405 for Butere and 412 for Khwisero). The HKI method of vitamin A assessment requires, at least 15 clusters each with at least 50 households (with children aged 12 and 71 months) for every cluster. However, because of both time and financial constraints, coupled with logistical limitations, the method was modified in order to cover only 8 communities in each division. Helen Keller Food Frequency checklist questionnaire was administered to all households selected. The respondents were the mothers of children aged 12-71 months, who were questioned on how often the children ate foods rich in vitamin A in the past seven days. Before administering the HKI food frequency, food items that are rich in vitamin A content and available in the locality were identified through qualitative market survey and group discussions. All food items replaced from the standard HKI food frequency were based on the criteria suggested by HKI food frequency method. All vitamin A rich foods in the HKI frequency list (the compulsory ones) were included in the food frequency questionnaire even if some of these foods were not available locally. The final food frequency questionnaire had 28 food items. For each community, the mean frequency of consumption of vitamin A was calculated for the analysis of food frequency data. The Helen Keller method threshold values for animal sources of vitamin A and total weighted measures (the combination of animal sources and plant sources) were used to categorize clusters into those which are deficient or otherwise not deficient in vitamin A. The results of the individual clusters were used to compute the vitamin A status of the entire study area. (The Helen Keller methodology requires that for a community to qualify as being sufficient in vitamin A intake, at least 75% of the 15 (in this case 8) clusters surveyed should be sufficient in the vitamin A intake). 3. RESULTS
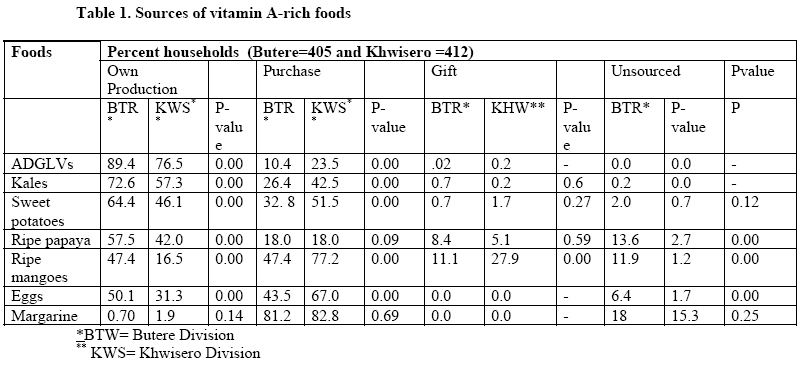
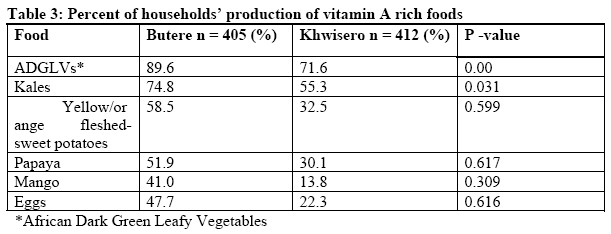
Vitamin A-rich foods (VARFs) produced in Butere-Mumias District Butere division had significantly (P<0.05), higher percentage of households who obtained their vitamin A-rich foods from own production than Khwisero division for most foods. This is in the case of African Dark Green Leafy Vegetables, kales, sweet potatoes, ripe papaya, ripe mangoes and eggs (Table 1). Conversely, households that obtained their VARFs through purchasing of ADGLVs, kales, yellow/orange-fleshed sweet potatoes and ripe mangoes were significantly (P <0.05) higher in Khwisero than Butere. The same pattern was observed in the way households obtained ripe mangoes in the form of gifts - significantly more households obtaining mangoes in form of gifts in Khwisero than in Butere. Table 2 depicts that Butere produced more amounts of vitamin A-rich foods than Khwisero, except for ripe papaya and mangoes. Butere had significantly (P <0.05), higher production of ADGLVs, and eggs per household per year than Khwisero. The results, as shown in Table 3 indicate that African dark green leafy vegetables were the most widely produced vitamin A-rich foods. This was closely followed by kales, with Butere having more households producing than Khwisero. The proportion of households producing ADGLVs and Kales, were significantly (P <0.05) higher in Butere than Khwisero . More households in Butere than in Khwisero produced sweet potatoes, papaya, mangoes and eggs but the difference was not significant (P <0.05). Purchase of vitamin A-rich foods in the area
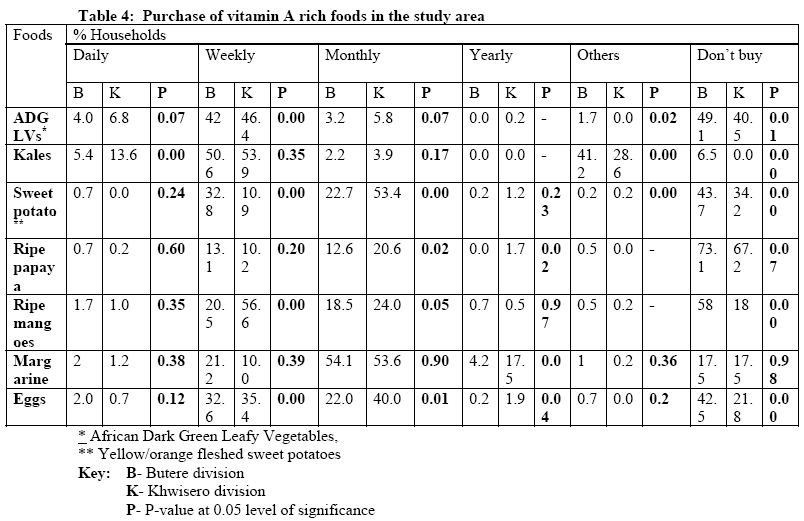
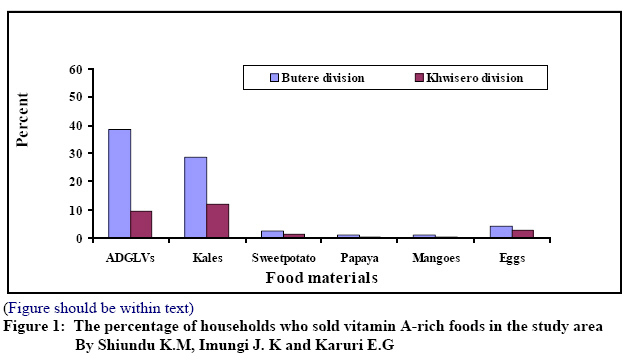
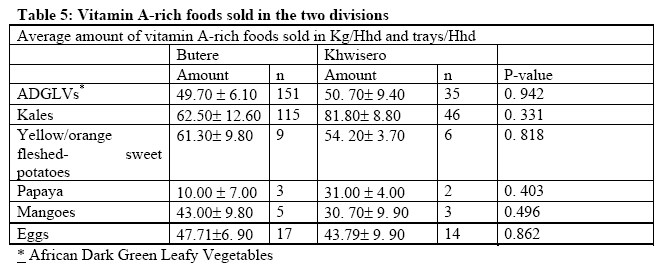
As depicted in Table 4, most vitamin A-rich foods were purchased on a weekly basis except for vitamin A fortified margarine, yellow/orange, fleshed-sweet potatoes and papaya, which were mostly bought on monthly basis. African dark green leafy vegetables were the most traded vitamin A-rich foods, with Butere having more households involved in the trade than Khwisero (Figure 1). Butere had also more people trading in kales than Khwisero. In Other words, there was significantly (P < 0.05), higher percentage of households selling ADGLVs and Kales in Butere than Khwisero. Quantitatively, as depicted in Table 5, it was noted that Butere sold more of dark green leafy vegetables, kales, potatoes, mangoes and eggs than Khwisero. There was no significant difference in the mean amounts of all the VARFs sold in the two divisions. HKI Food Frequency
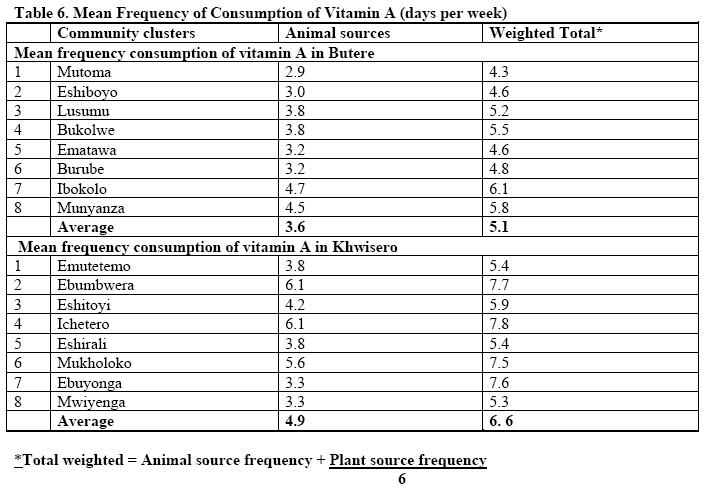
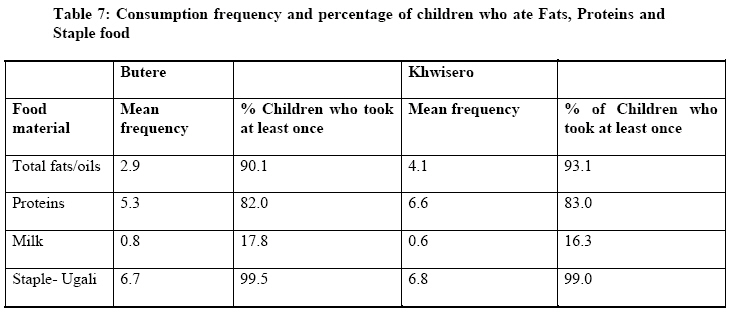
The study used Helen Keller Food Frequency Method to determine the frequency of consumption of vitamin A. Instead of the 15 clusters normally required in this method, only 8 villages were sampled in each division. The average scores for each surveyed cluster- community were obtained showing the mean frequency of consumption of vitamin A rich foods (Table 6). Based on weighted total, at least five villages in Khwisero division (out of 8 villages surveyed) could be said to be sufficient in the frequency of intake of vitamin A (above weighted total of 5.5). Only two villages in Butere division (out of 8 villages surveyed) showed sufficient intake of the vitamin A. The average frequency of intake of VARFs was significantly (P < 0.05) higher in Khwisero than Butere, both for animal based VARFs and the total weighted average frequency (both for animal and plant-based VARFs). The major sources of fat and oil in the survey were fried foods. Not a single child consumed red palm oil as it was reported not available in the community. It was found that 41 % of children in Khwisero and 27 % in Butere, consumed foods containing fat and oil, at least once, one week prior to the study. Foods cooked in oil were consumed by 80 % of children at least one day per week in Khwisero as compared to 71 % in Butere. Mean frequency of consumption of foods containing fat and oil was 1.2 days for Butere and 2.1 days for Khwisero, one week prior to the study. Mean frequency of consumption of fried foods was 1.6 days in Butere and 2.1days in Khwisero, one week prior to the study as shown (Table 7). The percentage of children that consumed at least once, fats and oils one week prior to the study were significantly higher in Khwisero than Butere (P < 0.05). This is the same case for the mean frequency of consumption of fats and oils. The Association between consumption of Vitamin A and related factors
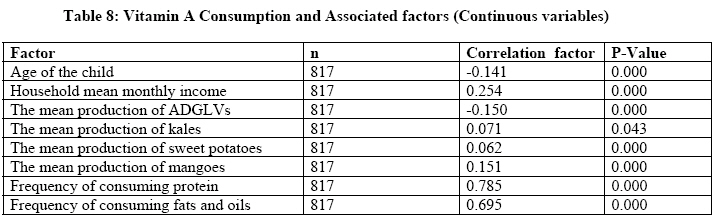
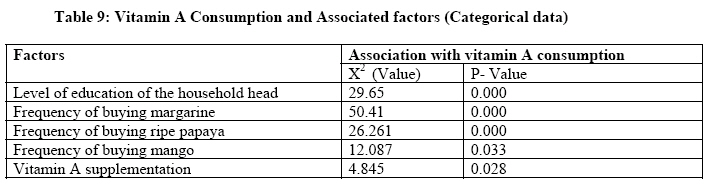
The factors as shown in Table 8 and Table 9 were found to be associated with the consumption of vitamin A in the study area. As shown in Table 8, there was positive correlation between most factors and vitamin A consumption except for age of the child and mean production of ADGLs. This meant that the higher the age of the child and mean production of ADGLs, the lower the consumption of vitamin A rich foods. Table 9 depicts the positive correlation between consumption of vitamin A rich foods and level of education, purchase of margarine, mangoes and papayas, and vitamin A supplementation. DISCUSSION Sources of vitamin A rich foods
The sources of vitamin A in the study area were mainly, own-farm food production and food purchased from the market. Animal-based vitamin A-rich foods: fish, meat, eggs and milk in this community are mainly purchased. Other food products like cooking oil and margarine are also obtained through purchasing. Sweet potatoes are partially obtained from home production and also through purchasing, because their productivity is not high in the area as it is also evident in official government statistics [6]. The study findings agrees with the views of the nutrition evaluation team from the Home Economics Offices and Ministry of Health staff in the field (Butere-Mumias District), which shows that the sugarcane zones have the highest malnutrition cases in Western province despite the fact that farmers in these areas earn better incomes than their counterparts elsewhere in the province. This implies that food availability in these areas is still poor. Butere had higher production in virtually all vitamin A-rich foods as compared to Khwisero. This can be explained by the fact that this area has been targeted by Rural Outreach Program (the local NGO) for the past ten years for agricultural extension especially for vitamin A rich foods. Butere division is also the headquarters of Butere-Mumias district and, therefore, has a relatively, well-established infrastructure (including roads) that motivates farmers to grow these foods. Additionally, Butere neighbours the more urban and industrial town and division of Mumias, which provides a ready market for their farm produce. Khwisero lacks these opportunities. Khwisero is a far-flung division and quite removed from the district's prime markets of Mumias and Butere towns. It does also have poor infrastructure and soils that are not very conducive for commercial farming [6]. It seems that agricultural extension, market availability and advocacy campaigns has resulted in increased production by framers of ADGLVs in Butere as compared to Khwisero. Purchase of vitamin A-rich foods
In both divisions, most vitamin A-rich foods were purchased on a weekly basis except for vitamin A-fortified margarine, yellow/orange-fleshed sweet potatoes and papaya, which were mostly bought on a monthly basis. The difference in the purchase of sweet potatoes in the two divisions can be attributed to the way the crop is produced. Butere has more households producing sweet potatoes and its average production per household is greater than Khwisero. The law of demand and supply would, therefore, dictate that there should be more supply of sweet potatoes in Butere than Khwisero, which helps to reduce the price hence people can buy more frequently, than is the case in Khwisero. African dark green leafy vegetables (sold by 38.3% of households in Butere and 9.5% in Khwisero) and kales (sold by 28.6% of households in Butere and 20.5% in Khwisero) were the most traded vitamin A-rich foods, with Butere having more households involved than Khwisero. The two divisions had on average 30 % of home produced VARFs sold, except for papaya and mangoes, where less than 4 % was sold. The apparent higher levels of selling VARFs in Butere could partly be attributed to efforts that have gone into the promotion of ADGLVs in Butere division as a viable income generation activity. This has helped to mobilize many farmers especially women to put into use the otherwise, idle kitchen gardens into production of the ADGLVs for both domestic consumption and for the market. It can also be argued that the presence of vibrant markets (both in Butere and Mumias towns) act as a motivating factor for farmers in Butere to produce and sell. This is unlike Khwisero, which is disadvantaged in this regard. HKI Food Frequency
Vitamin A consumption was higher in Khwisero than Butere. Foods containing fat and oil were also consumed by majority of the children but higher in Butere than Khwisero. Frequency of consumption of foods containing fat and oil and foods cooked in oil suggest that consumption is sufficient to ensure adequate absorption of vitamin A in most children. It should be noted that this survey was conducted during a dry season when most ADGLVs are in low supply (December-January). Accordingly, the results obtained would have looked, probably much better were it in the rainy season. However, the percentage of children who consumed ADGLVs and the mean consumption results, are realistic and reflect fairly the true vitamin A deficiency in the study area. It should be appreciated from the outset that adequate fats and oil consumption is needed for optimal absorption of beta carotene in the diets. Consumption of fats must be carefully considered though, because overemphasis of consuming fats and oil might, inadvertently, introduce other health issues related to excessive intake of saturated fatty acids in the diet [7]. There are two possible explanations for comparatively poor status of vitamin A consumption frequency in Butere. First, it can be argued from a general perspective that most households produce foodstuffs for selling given the relatively better infrastructure and ready market that is found in the division hence less food materials are left for households consumption. The study noted that there was higher illiteracy level among the household heads in Butere compared to Kwisero. In other words, there is an indication that lack of education/information could have affected vitamin A intake, more so in Butere. Butere division has largely been converted to a sugarcane growing area and very little is left for any purposeful food-crop farming. The introduction of sugarcane farming has in a way, reduced farm holdings to size that cannot adequately produce food crops to cater for both income and food needs of the family. The little amount produced from the already inadequate land is sold for income. It should be noted that sugarcane is essentially, a biannual crop and it takes on average, two years before farmers can earn any income. Vitamin A consumption and associated factors
The positive association between the mean production of most vitamin A-rich foods and consumption of vitamin A shows that improved promotion of specific food crops such as ALVs and yellow/orange-fleshed sweet potatoes would improve the vitamin A status in the area. On the other hand, there was no corresponding association between the number of households producing vitamin A-rich foods and vitamin A consumption, apart from kales. The implication obviously, is that the amounts of VARFs produced is more important than mere proportion of households producing vitamin A rich foods. It also means that the campaign to produce more ALVs needs to step and strengthen its nutrition messages and also put emphasis on households consumption. There was no positive association of the mean amount of vitamin A-rich foods sold, with vitamin A consumption. The proportion of households producing kales was found to have a significant positive correlation with consumption of vitamin A-rich foods. Similarly, mean amount of ADGLVs sold had a positive correlation with consumption of VARFs. This shows that most households that produce the two vegetables groups have adequate amounts of these vegetables, which they also use for households consumption. CONCLUSION AND RECOMMENDATION
Dark green leafy vegetables are major source of vitamin A in the rural parts of Kenya. Other vitamin A rich foods are kales, papaya, margarine, orange/yellow fleshed sweet potatoes, eggs and ripe mangoes. Vitamin A is a public health problem in the study area. It is thus recommended that both long and short term measures to control vitamin A deficiency should be implemented. Specifically, more work is required in promoting the production and consumption of the locally available VARFs, particularly plant-based food materials such as ADGLVs, kales, yellow/orange-fleshed sweet potatoes that have high potential in the area. This can be achieved through, strengthening of community and government extension agricultural services. Secondly, prophylactic and disease-targeted distribution of vitamin A supplements should be strengthened as a short-term measure to counteract the severe deficit in consumption of vitamin A-rich foods. Additionally, activities aimed at increasing consumption of vitamin A-rich foods and increasing fat and oil consumption among pre-school children should be implemented. ACKNOWLEDGEMENT
The authors of this paper would like to express their utmost gratitude to the Nutrition Third World of Belgium for making available the funds without which this project would not have been possible. More thanks go to Rural Outreach Program of Kenya, with special mention of the Program Founder, Hon. Prof. Ruth K. Oniang'o for personal involvement and support for this project. REFERENCES
Copyright 2007 - Rural Outreach Program The following images related to this document are available:Photo images[nd07016t6.jpg] [nd07016t5.jpg] [nd07016t3.jpg] [nd07016t2.jpg] [nd07016f1.jpg] [nd07016t1.jpg] [nd07016t7.jpg] [nd07016t8.jpg] [nd07016t4.jpg] [nd07016t9.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}