 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
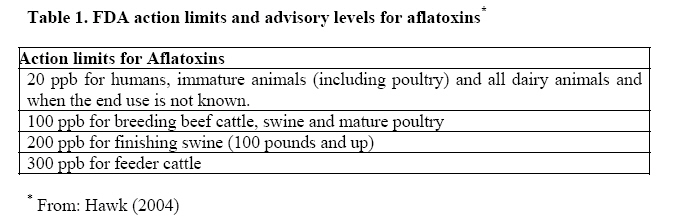
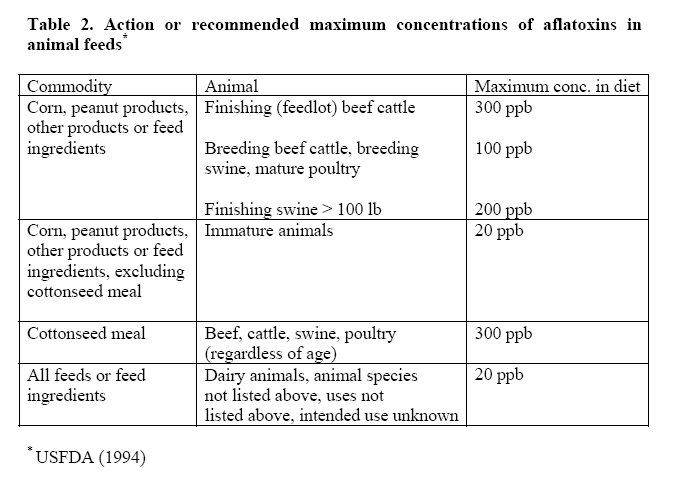
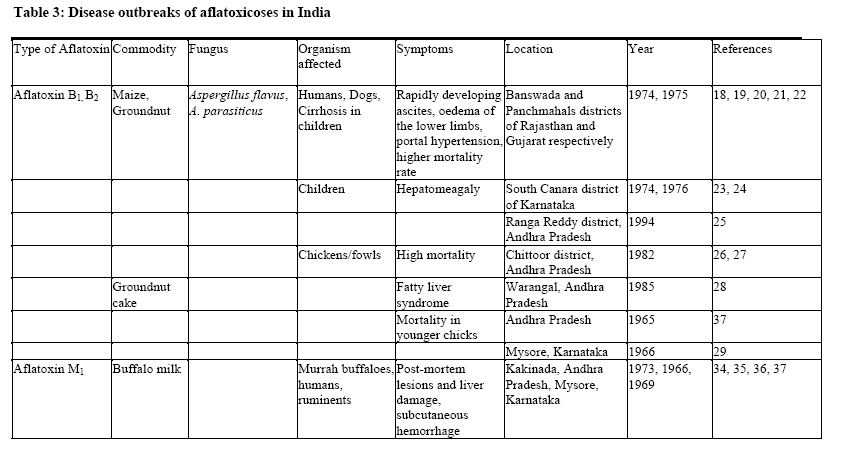
African Journal of Food Agriculture Nutrition and Development, Vol. 7, No. 5, 2007 OUTBREAKS OF AFLATOXICOSES IN INDIA Bhumi Narsimha Reddy*1 and Chinnam Raghu Raghavender1 *Corresponding author: Email: reddybn@osmania.ac.in 1Professor, Mycology and Plant Pathology Lab, Department of Botany, Osmania University, Hyderabad-500007, Ph: +91-09440115535 Bioline Code: nd07046 ABSTRACTMycotoxins particularly aflatoxins are gaining increasing importance due to their deleterious effects on human and animal health and also due to ubiquitous presence of aflatoxigenic fungi in all the agricultural commodities under field and storage conditions. In general, aflatoxins occur more frequently in tropical countries because of high temperature, moisture, unseasonal rains and flash floods. Poor harvesting practices, improper storage and less than optimal conditions during transport and marketing can also contribute to mycotoxin production. Chronic health risks are particularly prevalent in India where the diets of people are highly prone to aflatoxigenic fungi and aflatoxins. The present paper reviews the disease outbreaks of aflatoxicoses in India due to the ingestion of contaminated food and feed with aflatoxins. One of the first outbreaks of aflatoxicosis was reported from western India during 1974 with 106 deaths of indigenous people whose staple food was maize. This is perhaps the first report directly incriminating aflatoxin in food as a human health hazard at the indigenous community level. An independent study of the same outbreak was carried out subsequently also indicated that the aflatoxins were the major cause of the outbreak. Indian childhood cirrhosis, a clinical condition mainly confined to the Indian subcontinent has been attributed to aflatoxin contamination. They also found a correlation between aflatoxin contamination and fungal load on the one hand and hepatomegaly in children on the other in south Canara district of Karnataka. Another outbreak of toxic hepatitis affecting both humans and dogs was reported in India during 1974. Heavy mortality in chicks in Chittoor district of Andhra Pradesh was reported in 1982 due to aflatoxicosis. Another outbreak of aflatoxicosis in commercial poultry farms was also reported in the same district with hundred percent mortality. A case of aflatoxicosis in Murrah buffaloes from Andhra Pradesh was also reported. Occurrence of aflatoxicosis in poultry in Mysore state was first recognized in 1966 where 2219 chicks died in one week. Subsequently, several sporadic incidences were found in various poultry farms in Karnataka. Most of the outbreaks of aflatoxicoses described here are a consequence of ingestion of food that is contaminated with aflatoxins. Disease outbreaks due to aflatoxins continue to be problems of significant public health concern in India as long as people will consume contaminated food. The strict control of food quality is therefore necessary to avoid such incidences. KEY WORDS: Aflatoxicoses, Aflatoxins, Fungi, Food quality INTRODUCTIONAflatoxins are poisonous chemical compounds produced by certain fungi as secondary metabolites in agricultural products that are susceptible to mould infestation. Aflatoxicoses are the diseases in livestock, domestic animals and humans caused by ingestion of aflatoxins. Although exposure to aflatoxins is mostly by ingestion, it also occurs by the dermal and inhalation routes. The susceptibility of individuals to aflatoxins varies considerably depending on species, age, sex and nutrition. Acute mycotoxicoses can cause serious and sometimes fatal diseases [1-4]. The possibility of mycotoxin intoxication should be considered when an acute disease occurs in a large population when there is no evidence of infection with a known etiological agent and no improvement in the clinical picture following treatment [5]. Diagnosis of mycotoxicoses is difficult as they are similar to diseases with other causations. This is even more difficult in cases where more than one mycotoxin is involved because the toxins can produce additive and sometimes synergistic effects. The discovery of the hepatotoxic and hepatocarcinogenic properties of Aspergillus flavus in the early 1960s quickly followed by the elucidation of the structure of the aflatoxins changed the control strategy in the whole field of mycotoxins. A more quantitative approach is now possible, based primarily upon the chemical determination of the toxins and on studies of their effects in relation to dose. In spite of increasing knowledge concerning human aflatoxicoses, the majority of data available on aflatoxins and aflatoxicoses have been obtained from veterinary medicine. Field studies, as well as studies on experimental animals indicate that the potential toxicity of aflatoxins is great. Future investigations may well establish a causal role of aflatoxins in other human diseases besides those considered so far. [68]. Almost all plant products can serve as substrates for fungal growth and subsequent aflatoxin formation, thus providing the potential for direct contamination of human food. When farm animals are fed with aflatoxin contaminated feed, there will be not only a direct toxic effect on the animal but may also be a carry-over of the toxins into milk and meat, thus creating a further avenue for human exposure to aflatoxins. Furthermore, occupational exposure may occur through other media such as air. Since the discovery of the aflatoxins in the 1960s, regulations have been established in many countries to protect consumers from the harmful effects of mycotoxins that may contaminate foodstuffs, as well as to ensure fair practices in food trade. Various factors play a role in decision-making processes focused on setting limits for mycotoxins. These include scientific factors to assess risk (such as the availability of toxicological data), food consumption data, knowledge about the level and distribution of mycotoxins in commodities, and analytical methodology. Economic factors, such as commercial and trade interests and food security issues, also have an impact. Weighing the various factors that play a role in the decisionmaking process to establish mycotoxin tolerances is therefore of crucial importance. Despite the difficulties, mycotoxin regulations have been established in many countries during the past decades, and newer regulations are still being issued. National regulations have been established for a number of mycotoxins including the naturally occurring aflatoxins and aflatoxin M1 . International inquiries on existing legislation on mycotoxins in foodstuffs and animal feedstuffs have been carried out several times, and details about tolerance levels, legal bases, responsible authorities, and official protocols for sampling and analysis have been published. The Food and Agriculture Organization (FAO) of the United Nations [9, 10] has played a major role in providing information on worldwide regulations for mycotoxins in foods and feeds. The last comprehensive overview on worldwide regulations was published as the FAO Food and Nutrition Paper 64 in 1997. At that time, 77 countries had specific regulations for mycotoxins in different foods and feeds and 13 countries had general provisions, while about 50 countries did not have data available. The number of countries with specific regulations for mycotoxins has increased over the years. This reflects the general concerns the governments have about the potential effects of mycotoxins on humans and animal health and their implications to trade. The recent publication of the FAO [11] updated the information and described the situation of worldwide mycotoxin regulations as of December 2003, based on an international inquiry that was carried out in 2002 and 2003. The Food and Drugs Administration (FDA) action limits and advisory levels for different mycotoxins are shown in Tables 1 and 2 [12, 13]. The present paper reviews the disease outbreaks due to aflatoxins in India where the etiology of the disease is supported by aflatoxin analysis and identification of aflatoxin producing fungi [Table 3]. AFLATOXICOSESAspergillus flavus and A. parasiticus are fungi, which can potentially produce highly hazardous toxic residues known as aflatoxins. They specially affect oil seeds, edible nuts and cereals in sub tropical and tropical regions throughout the world due to inadequate storage conditions. The toxins are particularly carcinogenic in humans and eating contaminated food may result in liver cancer, amongst other diseases. Liver cancer takes time to develop but the aflatoxins act as an immunosuppressant so that affected individuals become susceptible to a wide range of diseases [2, 6, 7, 14, 15]. Livestock are also at risk and poultry are particularly susceptible. Cattle are not so susceptible but, if they are fed on contaminated feed, the toxin may pass into the milk. Besides endangering human health, aflatoxin contamination seriously affects the export potential of high value commodity crops, such as edible nuts (groundnut, pistachio, cashew and almond) and spices (turmeric and chillies), which provide an important source of income for farmers in the regions of semi-arid tropics. Diagnosing, or even preventing aflatoxin contamination will enable subsistence farmers to benefit from increased trade. It will also contribute to an improvement in the general health of people; often the poor who consume contaminated foods. Aflatoxins consist of a group of approximately 20 related fungal metabolites, although only aflatoxins B1, B2, G1 and G2 are normally found in foods. Aflatoxin B2 and G2 are the dihydroderivatives of the parent compounds. In well-developed countries, aflatoxin contamination rarely occurs in foods at levels that cause acute aflatoxicosis (diseases caused by aflatoxins). Aflatoxicosis is primarily a hepatic disease in humans. In view of this, studies on human toxicity from ingestion of aflatoxins have focused on their carcinogenic potential. The relative susceptibility of humans to aflatoxins is not known, even though epidemiological studies in Africa and Southeast Asia, where there is a high incidence of hepatoma, have revealed an association between cancer incidence and the aflatoxin content of the diet. These studies have not proved a cause-effect relationship, but the evidence suggests an association. Aflatoxins B1, M1 and G1 have been shown to cause various types of cancer in different animal species. Only aflatoxin B1 is considered by the International Agency for Research on Cancer (IARC) as having produced sufficient evidence of carcinogenicity in experimental animals [16]. Aflatoxin is a liver poison (hepatotoxin) in all species that consume it, however, ruminants tolerate it better than monogastrics or poultry. It causes liver damage at higher doses and liver cancer at lower doses. Aflatoxin exposure can depress the immune system. It may cause abortions in some instances, however, the circumstances necessary for abortions to occur are not well defined [17]. In 1974, an outbreak of hepatitis due to aflatoxicoses was reported in 200 villages in western India (Banswada and Panchamahals districts of Rajasthan and Gujarat respectively) with 106 deaths. The outbreak lasted for 2 months and was confined to tribal population whose staple food was maize. Analysis of Aspergillus flavus contaminated (6.25 - 15.6 ppm) maize samples showed that affected people might have consumed between 2000 - 6000 µg kg-1 (ppb) aflatoxins daily over a period of 1 month [18, 19]. Symptoms of the disease include rapidly developing ascites, oedema of the lower limbs, portal hypertensions and higher mortality rate. An independent study on the same outbreak also confirmed that the aflatoxins were the major cause of this disease [20]. Another outbreak of toxic hepatitis in India in 1974 affecting both humans and dogs was reported by Tandon [21]. High fever at the onset was marked but the hepatic histology was similar to that described in aflatoxicosis. The level of aflatoxin in contaminated samples was only 0.1 µg kg-1. This level of aflatoxin contamination was the same in affected and unaffected households. It was thought that other mycotoxins or combination of aflatoxin and an infection might have been implicated. A ten-year follow-up of the Indian outbreak found the survivors fully recovered with no ill effects from the experience. Childhood cirrhosis, a clinical condition mainly confined to the Indian sub-continent has been attributed to aflatoxin contamination [22]. Tandon [23] presented a strategy for investigating toxicoses of unknown origin and following a disease-oriented approach. The strategy is derived from and illustrated by experience of three large-scale outbreaks of disease involving aflatoxicoses in India, intoxication by pyrrolizidine alkaloids from Heliotrophium species in Afghanistan and from Crotalaria spp. in India. A correlation between aflatoxin contamination and hepatomegaly in children was reported in south Canara district of Karnataka [24, 25]. More than 200,000 broiler chickens died in 1994 in Ranga Reddy district of Andhra Pradesh, India after eating aflatoxin contaminated groundnut cake in feeds [26]. Heavy mortality in chicks in Chittoor district of Andhra Pradesh state, India due to aflatoxicosis was reported earlier [27]. The groundnut cake was implicated in the aflatoxicosis; groundnut cake was contaminated with aflatoxin at a level of 3590 µg kg-1. Another outbreak of aflatoxicosis in commercial poultry farms was reported in the same district with 100% mortality [28]. Aflatoxins (1400 - 3600 µg kg-1) were found in samples of maize and groundnut cake fed to the birds during the outbreak. Egg production dropped from 85 - 40% during an outbreak of aflatoxicosis in poultry during October 1985 in and around Warangal, Andhra Pradesh [29]. Post-mortem examination of dead birds revealed liver lesions of varying severity in all birds examined. An amount of 600 µg kg-1 aflatoxin was detected in these feed samples. No mortality was observed after the feed was changed and egg production increased gradually. Occurrence of aflatoxicosis in poultry in Mysore state, India was also reported earlier [30]. The disease was first recognised at the Government Poultry Breeding Unit, Hebbal, Bangalore in 1966 wherein 2219 chicks died in one week. Subsequently, several sporadic incidences were found in various poultry farms in the state. The disease was predominant in younger stocks, possibly due to increased percentage of protein in the form of toxic groundnut cake. Although humans and animals are susceptible to the effects of acute aflatoxicosis, the chances of human exposure to acute levels of aflatoxin is remote in well-developed countries. In undeveloped countries, human susceptibility can vary with age, health and level and duration of exposure. For example, an acute aflatoxicosis outbreak has occurred very recently in Kenya [31]. During January - June 2004, an aflatoxicosis outbreak in eastern Kenya resulted in 317 cases and 125 deaths. Aflatoxicosis outbreaks occurred previously in that geographical area and it was suspected that the unusually high number of patients with acute hepatic failure might have acquired aflatoxicosis from eating contaminated maize [32]. Public health officials sampled maize from the affected area and found concentrations of aflatoxin B1 as high as 4,400 ppb, which is 220 times greater than the 20 ppb limit for food suggested by Kenyan authorities [33]. Although aflatoxicosis outbreaks have occurred periodically in Africa and Asia, this outbreak resulted in the largest number of fatalities ever documented. A case control study was conducted by Azziz et. al., [31] to identify risk factors for contamination of implicated maize and for the first time quantitated biomarkers associated with acute aflatoxicosis. Aflatoxin M1 and M2are the hydroxylated metabolites of aflatoxins B1 and B2 and are produced in the milk when cows or other ruminants ingest feed contaminated with these mycotoxins. Aflatoxin M1 may also cross the placental barrier from the pregnant mother animal and thus contaminating the foetus by exposing the newborn to aflatoxin risk. Human exposure to aflatoxin M1 occurs primarily through the milk and milk products from animals that have consumed contaminated feed. IARC concluded in 1993 that there was sufficient evidence in experimental animals for the carcinogenicity of M1 and inadequate evidence in the case of humans. No additional toxicological information on aflatoxin M1 has appeared in the literature since 1993 [34]. Limited studies are available on aflatoxin M1 occurrence in milk in India. An investigation was conducted in Andhra Pradesh, India by Yadagiri and Tulpule [35] on aflatoxin contamination in buffalo milk. Out of 50 milk samples analyzed, 27 samples showed aflatoxin M1 in amounts ranging from traces to 4.8 µg/liter. Analysis of the groundnut cake, which formed 30% of the ration of cattle, indicated the presence of aflatoxin levels ranging from 1 to 3 mg/kg. The risk to infants and children exposed to aflatoxin ingestion through milk cannot be ruled out. Other outbreaks of aflatoxicoses in dairy cattle were also reported earlier from Mysore region [36] and in Murrah buffaloes from Andhra Pradesh [37]. A suspected outbreak of groundnut poisoning affecting 24 Murrah buffaloes was reported with details of the clinical course, post-mortem lesions, and histology of the liver [38]. This was the first record of groundnut toxicity in India although frequent cases of liver damage in Murrah buffaloes have been recorded in certain areas. Six buffaloes died in this outbreak. This emphasised the need for a constant awareness of the problem and the necessity for periodical screening of cattle feed and milk samples from different dairy products. Such a measure becomes imperative to prevent the possible risk of exposure to aflatoxin in infants who form the most vulnerable group of the population [35]. However, it is reassuring that in experiments carried out on lactating monkeys, administration of 500 µg of aflatoxin per day over a period of 18 weeks did not produce any toxic effects in suckling young ones although, their mothers showed hepatic lesions attributable to aflatoxin [39]. Aflatoxin has been shown to cross the placental barrier in humans [40]. Denning et. al. [41] reported the quantity of aflatoxin B1 and G1 in human cord sera obtained at birth and in serum obtained immediately after birth from the mother. The subjects of the study were residents of Songkhla, Thailand. Of the 35 samples of cord sera, 17 (48%) contained aflatoxin in concentrations from 0.064 to 13.6 nmol/ml, with a mean of 3.1 nmol/ml. By comparison only two (6%) of 35 maternal sera contained aflatoxin (mean 0.62 nmol/ml). These results demonstrate transplacental transfer and concentration of aflatoxin by the feto-placental unit, which may be of biological importance. An enzyme-linked immunosorbent assay (ELISA) developed to determine aflatoxin in food was adapted to analyse rapidly human serum for aflatoxin [42]. Sera from subjects in the U.K., Nigeria and Nepal were studied. No aflatoxin was found in U.K. sera, whilst 76% and 100% respectively of Nigerian and Nepalese samples were found positive for aflatoxin. Study was also made of maternal and cord sera from Thai subjects. Only 6% of maternal blood had detectable aflatoxin whilst 49% of cord sera were found positive for aflatoxin. This is evidence of trans-placental transfer of aflatoxin in humans and possibly of concentration of aflatoxin by the feto-placental unit. Maternal to child exposure of aflatoxin M1 in breast milk is an under evaluated risk factor from dietary exposure to aflatoxin B1 [34, 43, 44]. A molecular dosimetry study in The Gambia, West Africa, was initiated to explore the relationships between dietary intake of aflatoxins during a 1-week period and a number of aflatoxin biomarkers including aflatoxin metabolite excretion into breast milk. Detection of aflatoxin M1 in cord sera has been reported from Thailand, Ghana, Nigeria and Gambia. Several studies have demonstrated the presence of aflatoxin M1 in human milk. It was observed that only a small percentage of dietary aflatoxin intake was excreted in milk. [45]. Aflatoxins act very slowly and prolonged consumption can lead to liver cancer in humans. A person's chances of developing cancer are compounded significantly if he/she also carries the hepatitis B virus, which causes jaundice. In India, an estimated 20 million people are hepatitis B carriers. Importantly, the most commonly used cooking products are frequently contaminated. One of the major drawbacks in fighting aflatoxins is the fact that there is no awareness about these toxins in India. Western countries, on the other hand, have strict regulations governing the testing of food products for aflatoxins [11]. CONCLUSIONThe experience of the past 25 years indicate that, it is possible to maintain present food consumption levels by increasing overall food supplies in quantitative terms. However, in terms of providing food of the right quality, which is nutritious and free from environmental contaminants, the task ahead is challenging, particularly in highly populated parts of the world. Aflatoxins in general occur more frequently under tropical conditions and diets in many developing countries are more heavily concentrated in crops susceptible to mycotoxins. Chronic health risks are particularly prevalent in developing countries like India. In tropical conditions such as high temperature and moisture, monsoon, seasonal rains and flash floods leads to fungal proliferation and mycotoxin production. Poor harvesting practices, improper storage and less than optimal conditions during transport and marketing can also contribute to fungal growth and mycotoxin production. Most of the outbreaks of the aflatoxicosis described here are consequences of the ingestion of food that is contaminated with aflatoxins. The strict control of food quality is therefore necessary to avoid such outbreaks. Disease outbreaks due to mycotoxins continue to be problems of significant public health importance in India. In a majority of the cases, such outbreaks may be missed or misdiagnosed due to paucity of information in this regard. Sufficient attention to such disease outbreaks has not been focused in view of remoteness of the areas of such outbreaks [20]. Nearly 40% of the population in India live below the poverty line. It is very difficult to imagine their access to complete safe and toxin free food since people are forced to consume less expensive, poor quality food grains because of poor purchasing power. Aflatoxin contamination is therefore, unpredictable which makes it a unique challenge. REFERENCES
© Copyright 2007 -Rural Outreach Program The following images related to this document are available:Photo images[nd07046t3.jpg] [nd07046t2.jpg] [nd07046t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}