 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
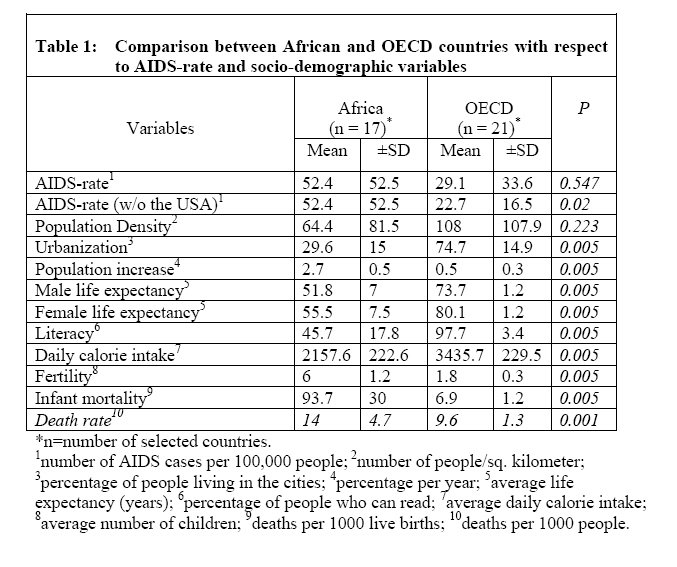
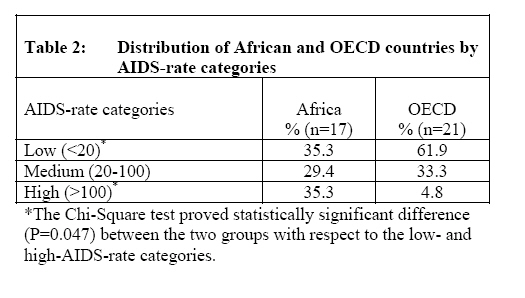
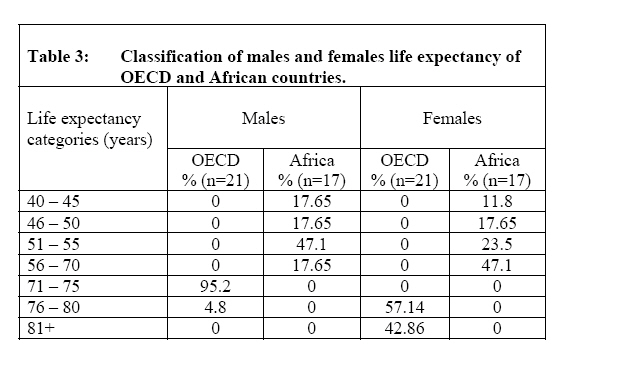
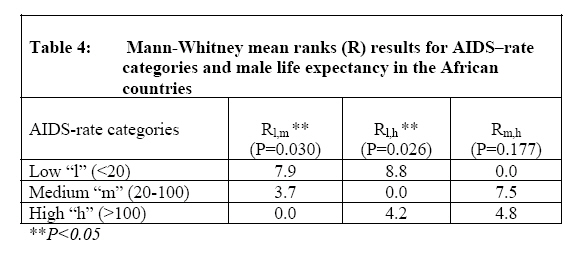
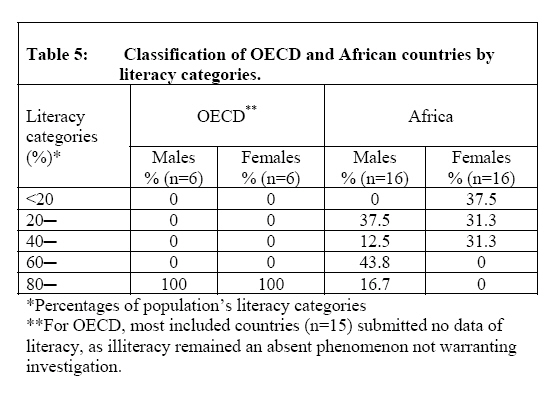
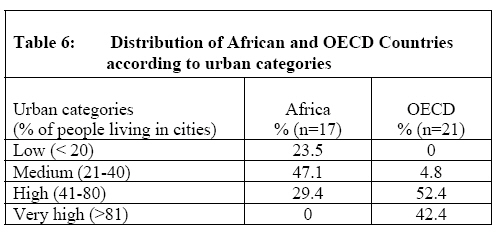
African Journal of Food Agriculture Nutrition and Development, Vol. 8, No. 1, March, 2008, pp. 1-16 Socio-Demographic Variables Associated with Aids Epidemic: Evidence From the Organization for Economic Cooperation and Development and the African Countries El-Asfahani AM1* and JT Girvan2 *Corresponding author Email: elasfahani@yahoo.com 1 Aida M. El-Asfahani, PhD, RD, Professor of Nutrition and Dietetic, Department of Agricultural Economics & Extension, Faculty of Science and Agriculture, The University of the West Indies, St. Augustine, Trinidad, West Indies. Code Number: nd08003 ABSTRACT The Human Immunodeficiency Virus (HIV) has been spreading rapidly worldwide for the past two decades, causing a variety of symptoms known as the Acquired Immune Deficiency Syndrome (AIDS), which has killed millions of people, and which looks likely to kill millions more. Generally, HIV infection rates are currently decreasing in several countries, but globally the number of people living with HIV/AIDS continues to rise both geographically and among specific demographic groups. For example, despite the remarkable efforts that are being made throughout Africa to avert the spread of HIV and reduce its impact, the HIV/AIDS pandemic in Africa continues to spread obstinately. Among the vexing issues related to the AIDS epidemic are the insufficient provisions of planners, policy makers and the public in general in curbing its devastating consequences to the health sector, households, schools, workplaces, economies and the quality of life as a whole. This paper presents information on the association between socio-demographic variables and AIDS prevalence in some African and the Organization for Economic Cooperation and Development (OECD) countries. The studied variables included size of population; population density; urbanization; average life expectancy; average female life expectancy; average male life expectancy; literacy; female and male literacy; population increase; infant mortality; average daily calorie intake; gross domestic product (GDP) per capita; religion; fertility rates; death rates; and AIDS-rate. Several parametric and nonparametric statistical techniques were adopted including Kruskal-Wallis, Mann-Whitney and Chi-square tests. Insignificant difference in the means of AIDS-rates between the OECD countries and the African group was found, but the difference was significant when the USA was excluded from the analysis. As initially expected, life expectancy in the OECD countries was significantly higher than that of the African group while the average rates of infant mortality, population growth, fertility, and death were significantly higher within the African group. Significant association between AIDS-rate and life expectancy was only found for African males, while association with fertility, infant mortality, population density, and calorie intakes was statistically insignificant. No clear difference between urban and rural areas with respect to AIDS-rates was discerned. Communities of Muslims were less subject to the AIDS problem. In conclusion, future studies should devote more attention toward impacts on HIV/AIDS prevalence of other equally important variables such as access to social and health care services, cultural norms, ethnic diversity, and educational facilities. Key words: Human Immunodeficiency Virus, Africa, Mortality INTRODUCTION Recent data show that, rates of people living with Human Immune-Deficiency Virus (HIV), the virus causing AIDS disease, continue to increase worldwide despite the efforts of governments and international organizations to prevent and reduce this trend. In 2005, the Joint United Nations Programme on HIV/AIDS (UNAIDS) indicated that globally about 40 million adults and children are living with HIV/AIDS, while 3.1 million people died of AIDS-related illnesses, bringing up the total death toll of AIDS since 1981 to about 25 million. An additional 4.9 million people globally became infected with HIV during 2005, indicating that the death cost will rise steeply in future years [1, 2]. The prevalence of HIV/AIDS was also shown to follow a regional pattern. Although sub-Saharan Africa (SSA) shares just over 10% of the world’s population, it is home to nearly two-thirds of the world's HIV-positive cases - almost 25.4 million. In 2004, approximately 3.1 million new infections occurred, while 2.3 million adults and children died from AIDS [1]. The United States Bureau of Census reported that the percentage of infected people in southern African cities of Zimbabwe, Botswana, Namibia, South Africa, and Swaziland almost quadrupled between 1993 and 1997, almost reaching a fourth of the population. In the same period, the HIV infection rate almost doubled in provincial areas to reach 16% of the population, which was not expected by researchers [3, 4]. As a growing number of people falling ill and eventually dying from AIDS goes up, there will be a tremendous impact on many parts of the society. The literature indicates that several socio-demographic variables such as literacy [1], population size [5-7], population natural increase rate [8], fertility [9], life expectancy [8, 10, 11], infant mortality [12, 13], religion [14], and urbanization [15-17] are associated with levels of HIV infection and the subsequent number of deaths from AIDS among young adults and children. Other variables may be relevant as well including population density. This is since “crowds” and overpopulated areas would logically enhance the spread of endemic diseases, AIDS included [18]. Considering the grave and serious worldwide situation of HIV/AIDS prevalence, particularly in Africa, this study will devote its attention to exploring the relative African conditions compared to those of a group of the most developed countries. In this respect the study will investigate the socio-demographic variables associated with rates of AIDS disease in countries of both the Organization for Economic Cooperation and Development (OECD) group and selected African countries. METHODS Data source Data used in this study was drawn from the file “world95.sav” which is a sample data set, supplied by SPSS, containing social, economic and demographic information for 109 countries worldwide [19]. For the purpose of this study some socio-demographic variables of selected African and OECD countries were extracted from the “World95.sav” data set. The OECD countries include: Finland, Norway, Greece, Iceland, Ireland, Sweden, New Zealand, Germany, Austria, United Kingdom, Belgium, Portugal, Netherlands, Denmark, Canada, Italy, France, Switzerland, Spain, Australia, and the United States. The socio-demographic variables in some countries, such as Japan, have not been studied and as such, this information has been excluded. The selected African groups include: Somalia, Morocco, Nigeria, Liberia, South Africa, Senegal, Cameroon, Ethiopia, Gambia, Gabon, Burkina Faso, Botswana, Kenya, Central African Republic, Burundi, Tanzania, and Rwanda. This study examined socio-demographic variables, whether affecting or affected by AIDS-rate (number of AIDS cases per 100,000 people) including: size of population (in 1000); density (number of people/sq. kilometer); urbanization (percentage of people living in the cities); average life expectancy (years); average female life expectancy (years); average male life expectancy (years); literacy (percentage of people who can read); female literacy; male literacy; natural population increase (percentage per year); infant mortality (deaths per 1000 live births); average daily calorie intakes; gross domestic product (GDP) per capita; religion; fertility rates (average number of children); and death rates per 1000 people. For the purpose of analyses, the AIDS-rate and urbanization variables were methodologically reclassified into categorical variables. AIDS-rate categories were low (<20 per 100,000), medium (20 - 100 per 100,000), and high (>100 per 100,000). Urban categories were low (<20%), medium-(21-40%), high (41-80%), and very high (81-100%). Religion was indicated through the use of three dummy variables: “1, 0, 0” for countries with dominant Islamic religion; “0, 1, 0” for countries with dominant Christianity; and “0, 0, 1” for “other” dominant religions (Tribal, Buddhism, Taoism, Hinduism, Judaism, and Animism). Statistical Analysis Mode Standard parametric and nonparametric statistical techniques were applied wherever deemed useful. The t-test, Kruskal-Wallis, and Mann-Whitney were used to examine the differences in means among groups. The Chi-square independence test was applied to test differences between distributions of African and OEDC countries among AIDS-rate categories. Pearson correlation coefficient was calculated to study strength of the linear relationship between AIDS-rate and the socio-demographic variables. Statistical analyses were performed using the Statistical Package of Social Science for Windows, version 10.0.5 (SPSS, Chicago, IL, U.S.A.). RESULTS The OECD group had statistically significant (P=0.005) higher mean rates of urbanization, literacy, female life expectancy, and male life expectancy than those of the African group. Conversely, infant mortality, population growth, fertility, and death rates were significantly (P=0.005) higher in the African nations. It seems that the relatively high AIDS-rate in the USA has affected the statistical difference between the average estimate for the OECD countries and the corresponding estimate of the African group (P=0.547). When the USA data was excluded (see table 1), there was a significant difference between the OECD countries and the African group (P=0.02). Table 2 reveals that the African countries were almost equally distributed among the three AIDS-rates categories. Countries of low AIDS-rate category (n=6, 35.3%) included Somalia, Morocco, Nigeria, Liberia, South Africa, and Senegal. The medium AIDS-rate category (n=5, 29.4%) involved Cameroon, Ethiopia, Gambia, Gabon, and Burkina Faso. Countries with the high AIDS-rate category (n=6, 35.3%) were Botswana, Kenya, Central African Republic, Burundi, Tanzania, and Rwanda. On the other hand, about 62% of the countries in the OECD group fell in the low AIDS-rate category including Finland, Norway, Greece, Iceland, Ireland, Sweden, New Zealand, Germany, Austria, United Kingdom, Belgium, Portugal, Netherlands, and Australia. Countries (n=6, 33.3%) with the medium AIDS-rate levels were: Denmark, Canada, Italy, France, Switzerland, and Spain. Only the United States of America fell in the highest AIDS rate category. The Chi-Square test proved a statistically significant difference (P=0.047) between the OECD and African groups with respect to the low- and high-AIDS-rate categories A much lower percentage of OECD countries fell within the lowest AIDS-rate category, while the relative importance of African higher AIDS-rate was statistically proven. Table 3 shows that in all of the OECD countries the average life expectancy of males exceeded 70 years of age, while falling below this figure in all of the African countries. Furthermore, in African nations, 82% of the male and 53% of the female life expectancies was below 55 years of age. Using the Kruskal-Wallis test, the relationship between AIDS-rate categories and life expectancy indicated that the differences in life expectancy levels according to AIDS-rate categories were only statistically significant (P=0.024) for males in the African group. The Mann-Whitney test shows that the lowest AIDS-rate category advantaged a statistically significant higher life expectancy level than that of the medium and high AIDS-rate categories (P=0.03, P=0.026, respectively), while the last two were indifferent in this respect, as shown in table 4. Accordingly, the hypothesis of AIDS negative impact upon life expectancy is accepted for the sole case of African males. Table 5 shows that literacy rate is about 85% or above in all OECD countries and is 76% or below in all of the studied African countries. Furthermore, a literacy rate of less than 60% occurred for men in 50% of selected African countries, and in 100% for women. Moreover, Kruskal-Wallis test showed that the differences in the means of literacy rates among AIDS-rate categories were statistically insignificant (P>0.05) in all cases. As such, a hypothesis of AIDS-rate strong link to illiteracy should be rejected. As for urbanization, as presented in table 6, 42.4% of OECD group populations live in the highest urbanized class, while the lowest urbanized category included 23.5% of the African population and none of the OECD. Testing the association between urbanization categories and AIDS-rate categories of the two country groups combined was found to be significant (P=0.004). However, this result was not reached when testing for each country group separately (P>0.05). Hence, the significant overall relationship may be elusive, and an assumed AIDS-rate link to urbanization should be rejected for the country groups being studied. Considering infant mortality, assuming the influence of AIDS, tests revealed negative results. Where overall samples for the two groups combined presented statistically significant (P=0.045) results, it was proved to be a statistical illusion, similar to urbanization effect. Analyses for the OECD and African country groups separately reveal statistically insignificant (P>0.05) impact of AIDS-rate categories on infant mortality. Therefore, a hypothesized positive impact of AIDS-rate on infant mortality should also be rejected. Likewise, tests for impact of population density on AIDSrate were statistically insignificant (P>0.05). Considering religion distribution in the OECD group and African countries separately, it was found that all the OECD countries are predominantly Christian, while in the African group six countries (37.5%) are predominately Islamic, five countries (31.25%) are predominantly Christian, and the rest fall in the “other” religion group (South Africa was excluded due to missing religion classification). A combined detailed analysis of the two country groups shows that the difference in the means of AIDS-rates between Muslim and Christian communities was statistically significant (P=0.032). Also, the difference in the means of AIDS-rates between countries with predominately Islamic and the countries that fall in the “other” religion group was statistically significant (P=0.002). A statistically significant (P=0.012) difference in AIDS-rates between the three religion groups was discerned. Moreover, Mann-Whitney test shows that the difference in the means of AIDS-rates between countries with a predominantly Muslim population and those countries with a predominantly Christian population was statistically significant (P=0.004). On the other hand, detailed analyses revealed that followers in the “other” religious group are not distinguished from Christian communities with respect to levels of AIDS-rate. As such, Muslim communities seem to suffer the least from the AIDS outspread. This was verified using Pearson correlation coefficient between AIDS-rate and either number of Islam or Christianity followers, reaching almost -0.68 for the first and 0.64 for the second. Likewise, there were negative significant correlations between AIDSrates and each of urbanization (r=-0.51, P=0.05), female life expectancy (r=-0.51, P=0.05), and male life expectancy (r=-0.65, P=0.01). On the other hand, AIDS-rate relationships with infant mortality, fertility, literacy, or average daily calorie intake variables were found to be statistically insignificant for both the OECD countries and the African group. DISCUSSION The objective of this study was to identify socio-demographic variables associated with AIDS-rates in selected African countries, compared to USA, Canada and Western Europe. Although not all the highly HIV infected African countries were included, AIDS-rates were found significantly higher in the African group than in the OECD countries without the USA. Such results coincide with other studies indicating that Africa remains the most affected region of the world by HIV/AIDS epidemic [1, 20, 21]. The revealed drop of African male's life expectancy with increased AIDS-rates, in the current study, is compatible with earlier studies emphasizing the impact of such fatal disease on lives of many adults in the African regions [11, 22, 23]. In Swaziland, Zambia, and Zimbabwe, it is projected that the average life expectancy of people born during the next decade will decline below 35 years, levels not seen since the end of the 19th Century [24]. The strong influence religion has in traditional societies seems to have played a key role in combating AIDS. The difference between Muslim and Christian dominant communities concerning AIDS-rates in favor of the first may be due to Islamic religious injunctions for strict avoidance of any extramarital sexual contacts, or abnormal contacts not targeting reproduction as being considered sinful. It also relates to the necessity of physical purification during Muslims’ daily prayers [14, 25, 26]. One of the most dramatic demographic consequences of AIDS is the increase in deaths, coinciding with previous studies [27, 28]. In the current study, the link between the death rate and AIDS-rate among the African group will most likely be significant in diminishing the size of the African population. It is worth mentioning that the United Nations Population Division indicated that unless AIDS disease is tackled rapidly, the size of 38 African countries will decrease in the following years by 14% [24]. When observing patterns of HIV/AIDS disease burden in relation to urbanization, the present study found an inverse significant correlation between urbanization and AIDS levels in the African countries. This result is inconsistent with other studies which indicated that urban areas and trading centers along the main roads generally show considerably higher prevalence of HIV infection than rural areas [28]. In developing countries, possible biases that should be considered when interpreting this result include rural poverty motivating people to migrate to urban areas in the hope of finding improved economic opportunities [29, 30]. They live in slums in large cities where they are at higher risk to become infected with HIV virus [31]. Indeed, seriously ill individuals return to their village of birth to die, as such the migration back to rural areas may interpret the underestimation of AIDS levels in urban areas and the high AIDS-related deaths among the rural Africans [23, 30]. Moreover, as statistics are often curtailed to simple urban –rural dichotomies, it is difficult to examine differences in AIDS rates among or within urban areas. This is due to the fact that the population in the city includes extremes of both wealthy people and those who are very poor. Recent research has demonstrated that residents of a small city and/or a slum have inferior access to public facilities compared to living in larger settlements; likewise the poor are at a disadvantage compared to those who are in better living conditions [18]. Urbanization, according to the present study, has a negative influence on African people with respect to the AIDS epidemic. Where crowded and high density areas are expected to be more suitable for the outspread of diseases, AIDS included, the insignificance of the population density effect in this study was unexpected. This contradicts Zieler et al. study which has shown that in Massachusetts as poverty increased (from 84 to 411 cases per 100,000) and as population density grew (from 66 to 746 cases per 100,000) the incidence of AIDS among white men rose steadily[ 18]. The general density figure the African countries in this study could be illusive, as based on the inclusion of vast uninhabited jungles and forests beside highly populated villages and cities. This may explain the revealed positive relationship between population increase and AIDS prevalence, in the current study, which most likely has reflected the population distribution more than the population density variable. In Africa, the drop in life expectancy reflects not only the death of people in young adulthood, but also an increase in infant mortality, as recent projections have shown that in Zimbabwe, South Africa and Namibia, more infants will die from HIV infection in 2010 than from all other causes [32]. However, the absent linkage between infant mortality and AIDS-rate in this study has contradicted findings of earlier studies [13, 33]. This could be explained by the interfering of many other infectious diseases such as malaria, measles, and diarrhea, particularly in the African countries [34]. In addition, because a precise monitoring of infant and child deaths is difficult in developing countries, they are more likely to be under-reported, Sub-Saharan Africa included. However, susceptibility to HIV/ AIDS in respect to poverty, ignorance, and illiteracy is expected in many developing countries including those in Africa [35]. Moreover, literacy in this study does not reflect a level of education permitting higher health consciousness or any educational protective measures against AIDS epidemic. Illiterate people do not have an adequate awareness to help protect them from HIV infection [36]. In fact, literacy, as just being able to read, though fairly prevalent for African people, is not enough to equip and empower them to combat AIDS disease. However, evidence shows a decline in HIV infection rates occurring among people with primary and post-primary education, even in countries where the overall HIV prevalence rate is still escalating [37]. A higher level of education will facilitate the understanding of HIV/AIDS specific information, and thus contributing to reduction of the risk of the disease [38]. It seems that including the USA, characterized by the highest both individual income and AIDS incidence among the OECD group has led to an expected positive correlation between per capita income and AIDS rate. On the contrary, in the most affected developing countries, there is a direct correlation between the extent of AIDS prevalence and the severity of negative GDP per capita trend [39- 41]. Cuddington [42] suggests that due to AIDS positive impact on morbidity and mortality rates, a reduction in the GDP in Tanzania in 2010 by 15 to 20 percent might occur compared to the no-AIDS scenario. CONCLUSION Several findings in this study were compatible with those of previous studies. Even where some results contradicted earlier findings, they could be at least partially explained by the interference of other factors beyond the scope of this study. They may include the spread of many fatal communicable diseases, the lack of public awareness of HIV/AIDS and dire poverty as in the African country group. Given the lack of epidemiological data, this study suggests that future detailed statistics concerning the complex environmental factors interrelated with HIV/AIDS epidemic are warranted in order to better control the spread of the disease globally. For example, it is necessary to neutralize, as far as possible, the interfering impacts of other endemic diseases such as malaria and diarrhea. Likewise the negative impact of crowdedness in urbanized areas should be separated from the positive impact of quality of life in urban areas. Characteristics of urban areas counteract each other with respect to the AIDS outspread. ACKNOWLEDGEMENT The authors would like to thank Prof. Amin I. Abdou at the National Research Center for his helpful comments on an earlier version of this article. REFERENCES
© Copyright 2008 -Rural Outreach Program The following images related to this document are available:Photo images[nd08003t1.jpg] [nd08003t5.jpg] [nd08003t4.jpg] [nd08003t2.jpg] [nd08003t6.jpg] [nd08003t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}