 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food Agriculture Nutrition and Development, Vol. 8, No. 1, March, 2008, pp. 28-47 Complementary Feeding Practices and Nutrient Intake from Habitual Complementary Foods of Infants and Children Aged 6-18 Months Old In Lusaka, Zambia Owino VO1*, Amadi B2, Sinkala M3, Filteau S4 and A Tomkins5 1Victor O. Owino, PhD., Research & Development Manager, Valid Nutrition, P.O.
Box 20375-00200 Nairobi, Kenya. Tel: +254725625720.
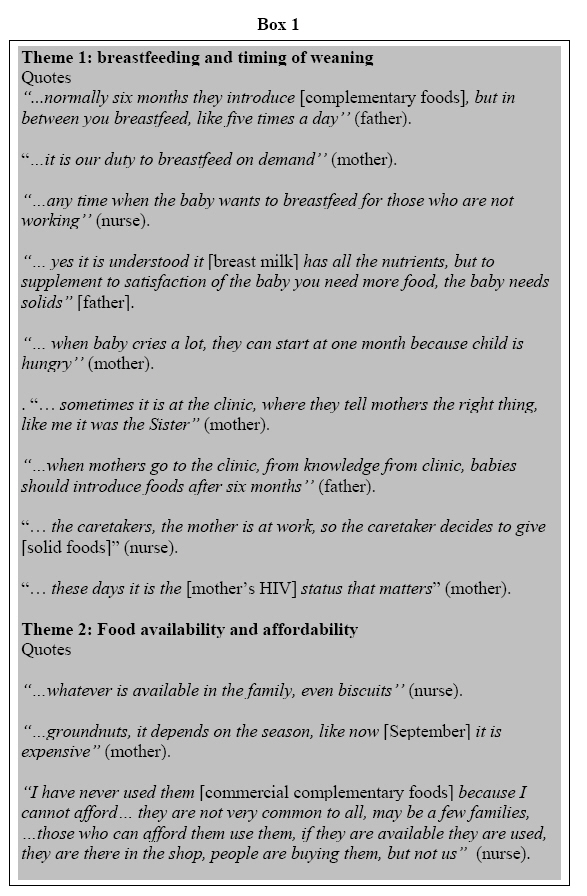
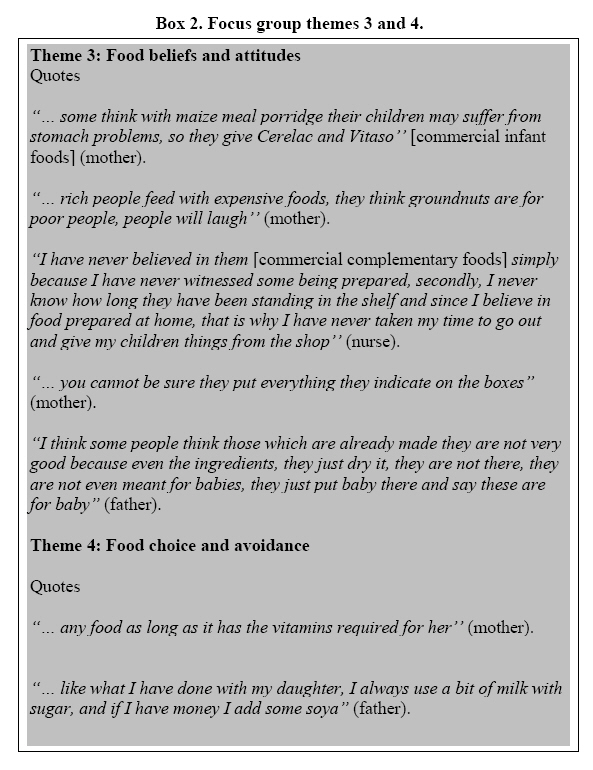
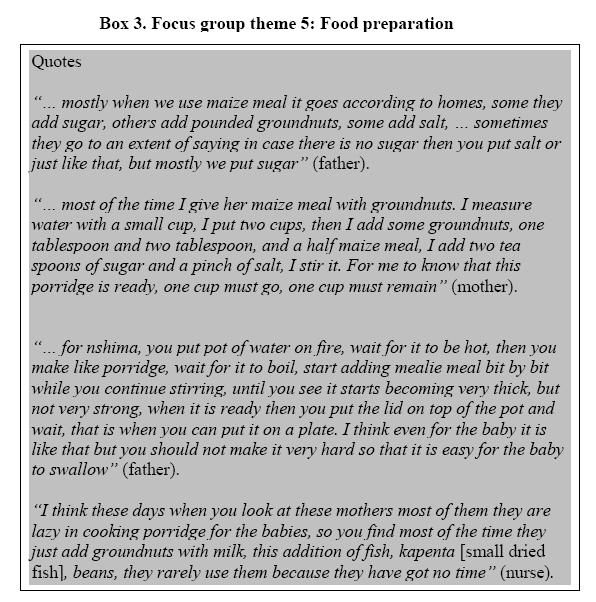
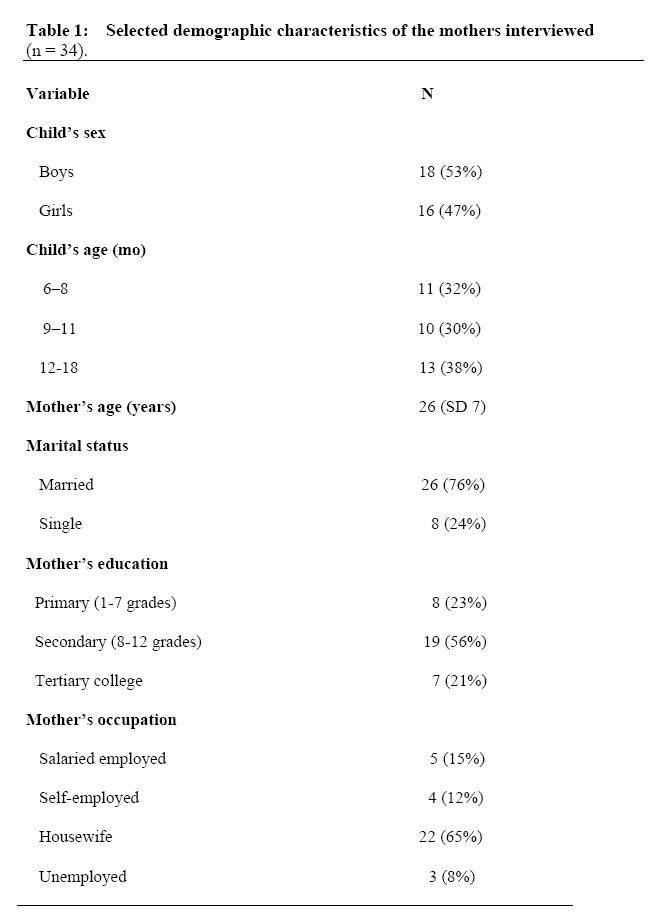
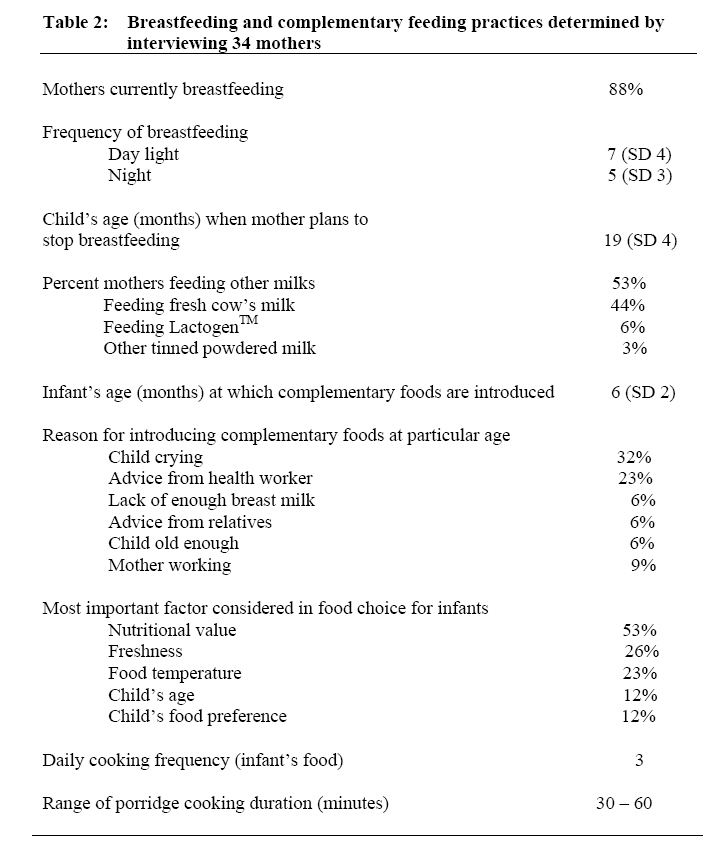
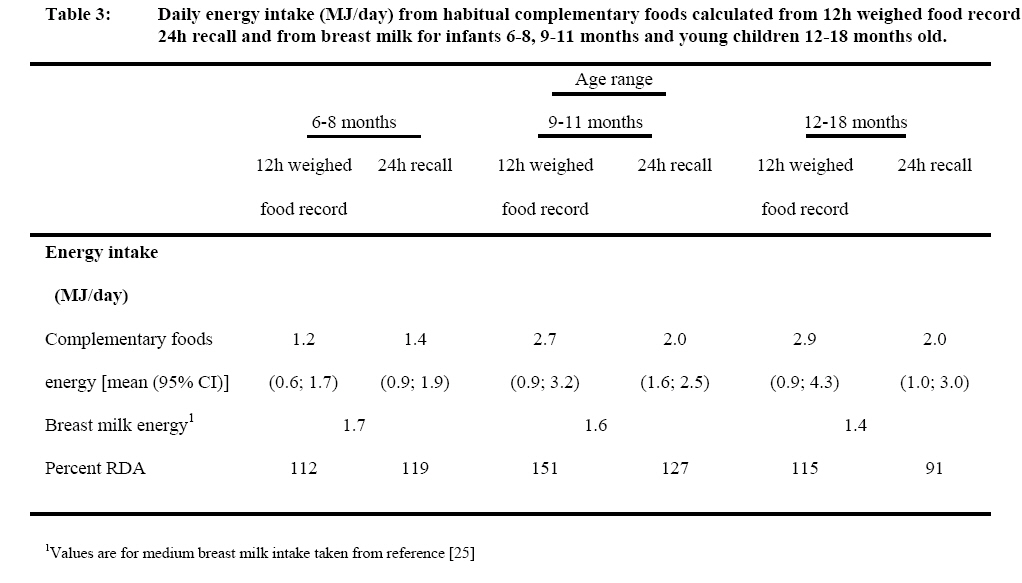
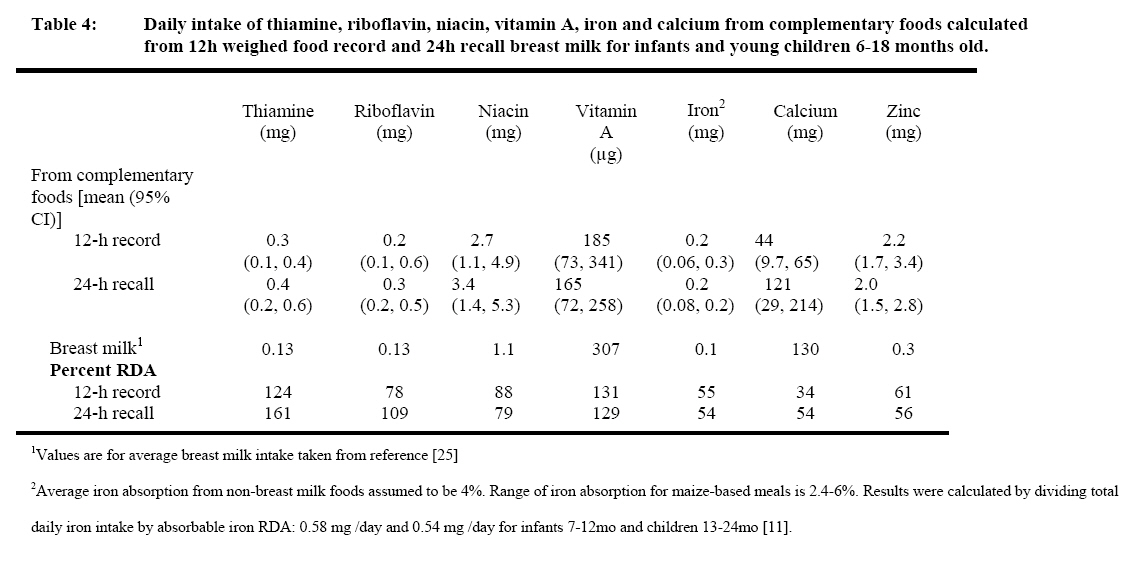
Email: vowino@hotmail.com Code Number: nd08005 ABSTRACT Poor quality complementary foods with low nutrient density and inappropriate feeding practices have been identified among the major causes of malnutrition in young children. In many developing countries, complementary foods are introduced too early or too late and the quality and quantity of the foods are insufficient, leading to a great risk of nutritional deficiencies during the second half of infancy. Most of the habitually used complementary foods in developing countries are unfortified cerealbased gruels characterised by low energy and nutrient density and are often inadequate in iron, zinc and pyridoxine and in some populations may be deficient in riboflavin, niacin, calcium, thiamine, folate, ascorbic acid and vitamin A. The aim of this study was to establish current complementary feeding practices of mothers/caretakers living in a medium income urban community in Lusaka, Zambia. The study was the first phase of a larger study designed to develop improved complementary foods based on already-in-use cereals and legumes for the improvement of infant health in urban settings characterised by high HIV prevalence. Complementary feeding practices and nutrient intakes of children 6-18 months old in Lusaka were assessed by qualitative and quantitative methods. Themes generated from three focus group discussions (9 health workers, 7 mothers and 8 fathers) were used to design a semi-structured questionnaire to interview 34 mothers, 20 of whom were observed for 12 hours at home and their infant’s dietary intake measured by 12-h weighed food record and 24-h recall, (assuming medium breast milk intake). The results showed that although mothers had wide knowledge of optimal infant feeding, actual practices were constrained by food cost, maternal HIV status and time availability. Compared with the recommended daily allowance (RDA) at 6-8, 9-11 and 12-18 months of age, the daily nutrient intakes were 88%, 121% and 94% for energy; 33%, 52% and 59% for iron and 30%, 33% and 38% for calcium, respectively. Fortification of complementary foods is necessary to meet infants’ needs for iron and calcium. Keywords: Complementary feeding, infants, iron, Zambia. INTRODUCTION Poor quality complementary foods with low nutrient density and inappropriate feeding practices have been identified as among the major causes of malnutrition in young children [1]. In many developing countries, complementary foods are introduced too early or too late and the quality and quantity of the foods are insufficient, leading to a great risk of nutritional deficiencies during the second half of infancy [2]. Most of the habitually used complementary foods in developing countries are unfortified cereal-based gruels characterised by low energy and nutrient density and are often inadequate in iron, zinc and pyridoxine and in some populations may be deficient in riboflavin, niacin, calcium, thiamine, folate, ascorbic acid and vitamin A [3, 4]. Food selection and preparation practices which affect food safety, nutrient density and feeding practices and maternal characteristics such as education, and socio-economic status have been identified as integral components of care-giving in relation to nutrition of young children [2]. The dearth of data on mother-infant interaction during feeding has been highlighted [2]. Such data may be used as the basis for education to cause change in feeding practices. Secondly, information on feeding practices may be used as the basis for complementary food design and promotion for the improvement of the nutritional status of infants and young children in resource poor settings. The main aim of this study was to assess the complementary feeding practices and nutrient intakes of children aged 6 – 18 months old in urban Lusaka as a prelude to the development and evaluation of the acceptability of a multi-micronutrient fortified maize-bean complementary food. METHODS The study was based at Chilenje clinic in Lusaka, Zambia, a medium income urban area where most households have running water and flush toilets. Chilenje clinic was chosen since the study was the initial phase of a larger study that aimed to assess the benefits of improved complementary foods among an urban population that could afford such foods. Ethical approval was obtained from the University of Zambia Ethics Committee and Great Ormond Street Hospital, UK. Qualitative data were obtained, based on convenience sampling, using three main techniques, namely, focus group discussions, interviews and home observations in order to allow for the triangulation of findings as described previously [5]. A qualitative approach was chosen to obtain information on knowledge, attitude and complementary feeding practices that could not be measured by standard quantitative methods [5]. Secondly, findings obtained by qualitative methods were used as the basis for the subsequent stage of complementary food development. Quantitative data were obtained by 24-hr dietary recall and 12-hr weighed food record. All participants gave written consent to attend the focus group discussions and had the ability to speak English. The requirement that participants be able to speak English was not a major source of bias as English is the official language in Zambia and schooling is in English. Focus group discussions Three focus group discussion sessions were held at Chilenje clinic with the help of two trained assistants (nutritionist and nurse) to assess current complementary feeding practices, attitudes and beliefs that would influence any nutritional intervention based on the provision of improved complementary foods. The three groups attending the discussions were: 1) 9 health workers from Chilenje clinic; 2) 7 mothers from Chilenje who had children aged 6-18 months 3) 8 fathers from Chilenje who had children aged 6-18 months. These three groups were chosen because they had direct involvement in child care and complementary feeding decision making process. Individual mothers, nurses and fathers were invited by one of the assistants who had good rapport with the Chilenje community based on her involvement in a previous project by our group. Focus group themes were explored using the same question guide for all the three focus groups discussion sessions. Proceedings of each discussion were recorded in note books by the first author and one assistant and on audio cassette which was later transcribed. Generated themes were used to design the semi-structured questionnaire for formal interviews. Interviews A total of 34 mothers of infants 6-18 months old were interviewed by the first author and two assistants using a semi-structured questionnaire that had been pre-tested at Chilenje clinic with three mothers of infants of the same age group (6-18 months). Participants were invited by the two trained assistants as they brought their children for growth monitoring at the clinic. The main inclusion criteria were that the mother was able to speak English and gave informed consent. The purpose of the interviews was to assess the availability and factors affecting the use of cereals and legumes and commercial complementary foods in addition to complementary feeding practices, knowledge, beliefs and attitudes. The questionnaire was divided into three main sections concerning household characteristics, food availability, and infant feeding and care practices. The third section was divided into four subsections namely, breastfeeding practices, infant care and time availability, complementary feeding practices, and food preparation and handling. All mothers were asked after the interviews if they would give consent for home visits after two weeks; 20 mothers gave written consent: 7 with infants 6-8 months, 6 with infants 9-11 months and 7 with children 12-18 months. Home observations The 20 mothers were observed at home for 12 hours during daylight by the first author accompanied by a female nurse. Although this approach provides first hand information, it is intrusive and the results may be biased due to change of behaviour by the subject in the presence of an observer [6, 7, 8]. Mothers were asked to continue with their normal routines while the researchers determined their actual food preparation and handling behaviour and how they fed their children. Dietary intake was determined by 12-h weighed food record for the day of the visit and 24 h-recall for the day preceding the observation. Weighed food record data were used to calculate the daily intake of energy, iron, and calcium based on a Zambian food composition table [9]. Medium breast milk intake was assumed based on the latest World Health Organization (WHO) estimates for children 6-23 months old [10]. Data for iron absorption from complementary foods and breast milk and the recommended dietary allowance (RDA) for absorbable iron were taken from the current WHO estimates [11]. Low iron absorption (2.4 – 6%) from maize-based diets was assumed. Daily amounts of absorbable iron obtained from breast milk were assumed to be 0.11mg/day and 0.09 mg/day for children 6-12 months and 13-18 months, respectively [11]. The daily intake of calcium from breast milk was assumed to be 130 mg, the estimate for children 6-23 months old and calcium retention from breast milk and solid foods was assumed to be 50% and 20-25%, respectively [10]. Energy and absorbable iron obtained from 12 h weighed food record and 24 h recall of the day preceding the observation were compared. A total of 10 and 9 porridge recipes obtained by 12 h weighed food record and 24 h recall, respectively were compared. Data analysis Data analysis was performed by the first author based on previous guidelines [6, 12]. Tape records of the three focus group discussions were transcribed verbatim and combined with a review of notes that were taken by the researcher and an assistant. The transcripts were coded into major themes that were generated manually. Internal validity was ensured by combining focus group discussions with interview and home observation data. In addition, peer examination of the transcripts was done by an African nurse with experience in nutrition who was not directly connected with the study. Quantitative data from home observation were double entered using Epi Info (version 3.2, Center for Disease Control and Prevention, WHO, 2002). Frequencies, means and median values were calculated using SPSS software (version 11.6). RESULTS Focus Group Discussion Themes Five major focus group discussion themes were generated: 1) breastfeeding and timing of weaning; 2) food availability and affordability (see Box 1); 3) food beliefs and attitudes; 4) food choice and avoidance (see Box 2); and 5) food preparation (see Box 3). Breastfeeding and timing of weaning There was wide knowledge of the benefits of breastfeeding for the first two years of life. The need to feed on demand was also supported, especially for younger infants and in cases where mothers were not working outside the home. Even though there was understanding of the benefit of breastfeeding, there were doubts as to the nutritional adequacy of breast milk. Complementary foods were introduced mostly when the child attained 4 – 6 months; however, the age of introducing these foods ranged from 1 – 9 months. Factors determining the timing of complementary foods included baby crying, and baby not being satisfied. The other factors were advice from the health clinics and the necessity for some mothers to return to work. Knowledge of maternal HIV status was also mentioned as one of the factors that may lead to early introduction of complementary foods. Food availability and affordability The main foods available for feeding infants included maize meal, rice, groundnuts, beans, fish, milk and fruits (bananas, oranges, pawpaw) and vegetables (carrots, pumpkins, green vegetables). The child’s food was determined by what was available in the household, the cost of food and seasonality. Even though commercially processed complementary foods were also available in the market, their use for feeding infants was restricted by the high prices. Food beliefs and attitudes There was preference for foods prepared at home as mothers felt that they were fresher and that they contained all the nutrients. However, there was also acknowledgement that some of the foods (such as okra prepared using sodium bicarbonate and cold foods) prepared at home may cause stomach problems in the child. The use of traditional foods as opposed to commercially prepared foods was thought to be more common among poorer households. There was acknowledgement that commercially processed complementary foods were easy to prepare and some participants felt they were better than what they prepared at home. However, the use of these foods was hampered by mistrust of their freshness and nutritional completeness. Food choice and avoidance Food choice was affected mainly by the food’s nutritional value, availability, child’s age and cost. Other factors included expiry date and temperature. There was emphasis among focus group participants on the provision of a varied diet. With additional income, households buy foods they consider more nutritious. Foods were considered bad if they were carbonated, spiced, acidic or too sweet. Food preparation The main food for infants was porridge that was prepared in different ways depending on ingredient availability. Cooking of porridge lasted 20 – 45 minutes. The other major food for infants is nshima (a stiff porridge from maize meal) and is prepared such that the child can easily swallow it. Mother’s availability had a major effect on what food the babies were fed, how these foods were prepared and meal frequency. Interviews Table 1 shows the selected demographic characteristics of the 34 interview subjects. Most (62%) of the households had 2-3 children and 32% of the households had another child aged below 5 years. Table 2 presents breastfeeding and complementary feeding practices of interviewed mothers. A majority of the mothers (88%) were still breastfeeding. Foods other than breast milk were introduced into the infant’s diet at an average age of 6 (SD 2) months of age, indicating that mothers were complying with breastfeeding guidance. Cessation of breastfeeding was at the age of 19 (SD 4) months. The choice of which solid food the infant was fed on was based on mother’s perceived nutritional value of the food. Use of legumes, cereals and pre-packed complementary foods, and food preparation For preparation of infant foods, all mothers used maize, beans and groundnuts, while a third of mothers used bambara nuts and pre-cooked soya flour. Maize-meal-based porridge was the main form of food for infants. Porridge was prepared with the addition of any or more of the following ingredients to maize meal: pounded groundnuts, cooking oil, sugar, fresh milk, salt, eggs and custard powder. The main pre-packed multi-micronutrient fortified cereal-based complementary foods available in Lusaka were high energy protein supplement (HEPS, a maize-soya food mainly used as food aid in relief operations), Speciality VitasoTM, Speciality NutrexTM and CerelacTM. These foods are mainly targeted to children from 6 months to 4 years of age. The average price per kilogram for these foods was found to be US$ 4.6 (SD 2.4) and most mothers in Chilenje could afford them. Cash expenditure on food and fuel The mother’s ability to purchase food for their child was determined mainly by educational attainment, which may have affected salary levels, and marital status. Mothers who had attained primary, secondary and tertiary level of education made spending decisions in 25%, 32% and 83% of the cases, respectively. While married mothers made spending decisions in only 27% of cases, single mothers decided in 75% of cases. Eighty two percent of mothers used electric hot plates for cooking, while 18% used charcoal. The mean monthly electricity cost was USD 12. Lack of electricity occurred mostly twice a week, but this became worse during rains and 59% of mothers recalled having experienced electricity failure in the month prior to the interview. HOME OBSERVATIONS Dietary intake Table 3 presents the daily intake of energy from habitual complementary foods measured by 12h weighed food records, and 24h recall, and from breast milk for infants 6-8 months, 9-11 months, and young children aged 12 – 18 months old. Energy intakes obtained by 12 h weighed food record and 24 h recall were comparable. However, the food solids intake values obtained by 12 h weighed food record were higher than those obtained by 24 h recall. The mean energy density based on recipes from 12h food record and 24h recall of home porridges was 3.8 (SD 1.1) kJ/ml and 3.5 (SD 1.1) kJ/ml, respectively for recipes obtained by 12 h weighed food record and 24 h recall. The average daily complementary food intake was 127 g (95% CI, 82.7, 171.3) for the three age groups. The average daily intake of protein and fat were 10.6 g (95% CI, 5.2, 16.0) and 11.6 g (95% CI, 6.3, 16.8), respectively, representing 107% and 179% of RDA for protein and fat, respectively, for children aged 6 – 18 months. Table 4 shows the daily intake of thiamine, riboflavin, niacin, vitamin A, iron and calcium from complementary foods calculated from 12h weighed food record and 24h recall and breast milk for infants and young children 6-18 months old. While most of the micronutrient intake results were comparable for the two methods, values for thiamine, riboflavin and calcium were lower when 12h weighed food record was used. The mean absorbable iron density of the porridges was 3.0 (SD1.6) µg/ml (95% CI, 2.0, 4.0) and 4.5 (SD 3.1) µg/ml (95% CI, 2.5, 6.5), respectively for recipes obtained by 12 h weighed food record and 24 h recall. Infant feeding and care In most cases (70%), the mother fed the child. The rest of the time the child was fed by the grandmother, sibling or house-help. The feeding location was predominantly (75%) in the sitting area of the family house with the child held on the mother/caretaker’s lap. Verbal encouragement was observed in 74% of the cases, and in most cases was occasioned by the child’s refusal to eat. Predominant silence with occasional encouragement or coaxing was observed in 26% of the cases. Feeding utensils comprised plastic cups and spoons for porridge. Other foods were served on plastic plates and fed by hand. Most mothers (68%) did not store leftover food, which in most cases was eaten by an older member of the family (mother, sibling or any other member of the household). DISCUSSION The dietary data show that energy and macronutrient intakes of infants and young children in this population were generally adequate, but that intakes of certain minerals, particularly iron, calcium and zinc, were inadequate. The strong support for breastfeeding by mothers, fathers and health workers contributed to the adequate intakes of many nutrients. However, in order to improve infant nutrition in Lusaka, it may be necessary to develop and promote fortified complementary foods which are acceptable to and affordable by families since they are produced based on locally grown cereals and legumes. The focus group discussion results show that even though some mothers use commercially processed complementary foods to feed their children, most mothers, including well educated people, regard these foods with suspicion. This is mainly with regard to how long the foods have been on the shelf. Most of the existing commercially processed foods in Lusaka cost on average US$ 4 per kilogram pack since they are largely based on imported ingredients based on milk powder. Most mothers in Chilenje could not afford these foods. Engagement in work outside the home was a constraint on the length of time the mother spent on child feeding and care. Food that is considered good on the basis of its nutritional value and freshness and that which can be readily prepared had potential market among Chilenje mothers. The wide support for breastfeeding is supported by the observation that only 2 of the mothers introduced complementary foods due to reported perception of lack of enough breast milk. The median age for the introduction of complementary foods was 6 months as recommended [13], but some mothers introduced these foods too early at 2 months and some too late at 12 months. The acknowledgement of maternal HIV status as a determining factor for the early introduction of complementary foods supports previous observations that knowledge that HIV can be transmitted through breastfeeding results in decreased levels of breastfeeding [14]. This may reflect a response to current recommendations for abrupt cessation of breastfeeding for HIVinfected mothers in cases where affordable, feasible, acceptable, sustainable and safe replacement feeding is available [13]. Other work from our group [15] showed that HIV-infected primiparous women stop exclusive breastfeeding earlier than other women in Chilenje, suggesting that there is confusion about what is the best feeding practice for HIV-infected women in resource poor settings where the strict criteria for replacement feeding may not be easily met. Fear of disclosure of HIV status and stigma may lead to too early introduction of fluids and other foods as reported from South Africa [16]. Further, emerging evidence indicates that some mothers who know that they are HIV-infected still continue to breastfeed even in cases where there is counselling on infant feeding options [17]. This has been attributed to lack of openness among partners, fear of stigma in the community lack of knowledge and lack of money to buy replacement formulas [16-19]. A recent review further highlighted difficulties in constructing a nutritionally adequate diet for the nonbreastfed child in low income settings [20]. The observation that mothers/caretakers encouraged the child to eat only when the child was not eating well is contrary to the currently recommended responsive feeding [21] that entails feeding with positive verbal encouragement, without physical or verbal coercion [2]. The fact that most feeding sessions took place in the living room could result in interruption of feeding by visitors and entertainment media such as television. The significance of a feeding environment free of distraction for adequate nutrient intake has been underscored [2] The observed daily intake of food solids is within the range of 25 g to 250 g reported earlier for developing countries [10]. The observed total intake of absorbable iron and calcium fell short of recommended values [10, 11]. The observed intake of iron in the current study is consistent with recent observations from Tanzania [22] that complementary foods provided 15%, 20% and 27% of iron requirements for infants 68, 9-11 months and young children 12-23 months, respectively. The current results also support recent findings from South Africa [23] that complementary foods were inadequate in iron, zinc and calcium. The observed high intakes of vitamin A can be attributed to the fact that in Zambia sugar is fortified with vitamin A at a minimum rate of 10 mg/kg [24]. From 24h-recall data, sugar formed 20% of porridge dry recipe. It is estimated that vitamin A intake from sugar in the three groups accounted for 63% of the total vitamin A intake from complementary foods. This finding is consistent with the results of evaluation studies on the effect of sugar fortification on vitamin A status in Zambia [24]. Since vitamin A is classified as one of the problem micronutrients in developing countries, the Zambian model of fortifying sugar with vitamin A may be used in other countries [25]. However, sugar may not be affordable to most households in poor settings and may thus not be the best vehicle for vitamin A. Micronutrient capsules or sprinkles may be more appropriate for poor settings [25]. Inadequate intakes of iron, calcium and zinc augment previous observations that these three micronutrients are among ‘problem nutrients’ in developing countries [25] even in cases where strategies to improve their bioavailability are employed [26]. A recent double-blind, randomized placebo-controlled study from Tanzania [22] showed that improved iron solubility and energy density of a complementary food processed using germinated and autoclaved finger millet-kidney beans, roasted peanuts and mango puree had no effect on growth, haemoglobin and iron status of children 6-12 months old. The workers concluded that the slight improvement in iron solubility as a result of processing was not sufficient to offset the low iron content of the complementary food. A study from Bangladesh reported inadequate intake of vitamins and minerals among breast-fed infants 6-12 months old and attributed this to low micronutrient density of complementary foods [27]. The findings of the current study strongly support previous recommendations that multi-micronutrient fortification of complementary foods is required if the needs for ‘problem nutrients’ like iron, calcium and zinc are to be met, especially for nonbreastfed infants after the first 6 months of life. ACKNOWLEDGEMENTS We acknowledge the support of the entire staff of the Breast Feeding and Postpartum Health Project throughout the study. We are grateful for the assistance in data collection by Molly Chisenga, Lungowe Nyaywa, Mutinta Muzyamba and Tamara Kavimba and in analysing qualitative data by Rachel Rori. We also acknowledge the contribution of Rhoda Zulu, National Institute for Scientific and Industrial Research, Lusaka for her critique of this manuscript. We are grateful to Score Africa for the financial support. REFERENCES
© Copyright 2008 -Rural Outreach Program The following images related to this document are available:Photo images[nd08005t3.jpg] [nd08005b2.jpg] [nd08005b1.jpg] [nd08005b3.jpg] [nd08005t2.jpg] [nd08005t1.jpg] [nd08005t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}