 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
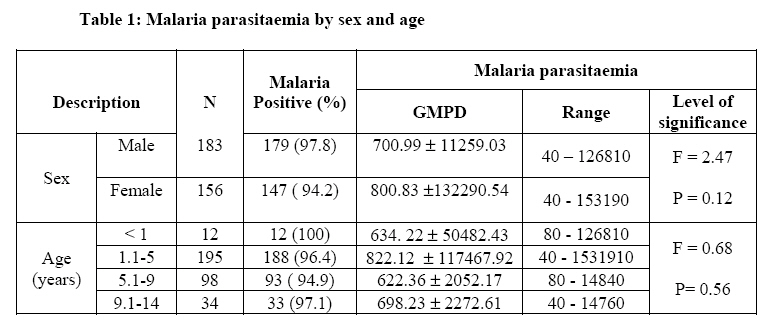
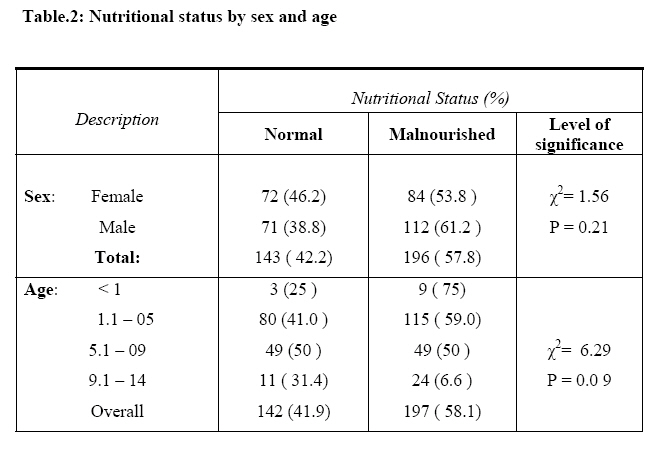
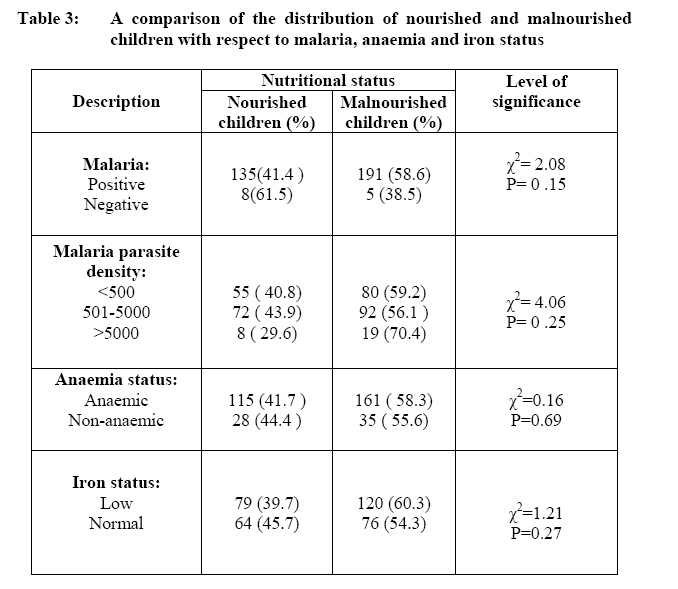
African Journal of Food Agriculture Nutrition and Development, Vol. 8, No. 3, Sept, 2008, pp. 252-264 The Burden Of Malaria And Malnutrition Among Children Less Than 14 Years Of Age In A Rural Village Of Cameroon Theresa K. Nkuo- Akenji1, I. Sumbele2, E.N Mankah1, A.L. Njunda3, M. Samje1 and L. Kamga3 *Corresponding author Email: wifon@yahoo.com Code Number: nd08024 ABSTRACT Malaria and malnutrition are a major health burden in developing countries with infants and children being the most vulnerable groups. The extent of the burden of malaria and malnutrition was investigated in 339 children ≤14years residing in the village of Muea located in the South West Province of Cameroon. Malaria parasitaemia was determined microscopically from Giemsa stained thick blood films. Nutritional status was determined using age and the anthropometric parameters of weight and height. Height-for-age (HAZ), weight-for-age (WAZ) and weight-forheight (WHZ) Z scores were computed based on the National Centre for Health Statistics (NCHS)/World Health Organisation growth reference curves. Anaemia was assessed by measuring haemoglobin (Hb) concentration while plasma iron levels were determined by spectrophotometric assays. The prevalence of malaria in the study population was 96.2% (326/339) with a majority (68.4%) having asymptomatic disease. The geometric mean parasite density (GMPD) was 744.37 ± 89396.11 (parasitaemia range 40-153190 parasites/µL blood). The mean Hb concentration was 9.29 ± 1.8g/dL (range 4-14.1g/dL) and anaemia (Hb<11g/dL) was diagnosed in 81.4% of the children, a majority of whom had microcytic anaemia. A negative correlation was observed between parasite density and haemoglobin concentration (r = -0.14). The mean plasma iron level was 53.64 ± 32.87µL/dl (range 1.8-159) with 58.7% (199/339) of the children diagnosed as iron deficient (plasma iron concentrations <50µg/dL). A negative correlation was observed between plasma iron values and malaria parasitaemia (r = -0.031). The prevalence of malnutrition was 58.1% (197/339). Of the 197 malnourished children, 23.6% were wasted (< -2 SD weight-for-height Z- score), 26.5% underweight (< - 2 SD weight-for-age Z score) and 49.9% stunted (< - 2 SD height-for-age Z score). There was a negative correlation between nutritional status and malaria parasitaemia (r =-0.034). The findings from this study are strongly suggestive that falciparum malaria and malnutrition exist in children residing in Muea and constitute a major health problem which needs to be immediately addressed to reduce morbidity and mortality. Key words: Malaria, Malnutrition, Anaemia, Iron, Children. INTRODUCTION Malaria and malnutrition remain major causes of child morbidity and mortality [1] yet, their precise interaction remains unknown. Malnutrition commonly affects all groups in a community, but infants and young children are the most vulnerable because of their high nutritional requirements for growth and development. The etiology of mild to moderate malnutrition in most tropical countries is probably multifactorial, not only involving an inadequate or inappropriate diet but also intercurrent infections [2]. The diagnosis and management of malnutrition in Third World countries have to be mostly a public health operation as many malnourished individuals live in slums, shanty-towns or remote rural areas and do not visit hospitals [3]. Malaria is still the world's most important parasitic disease and is responsible for the death of more people than any other communicable disease except tuberculosis [4]. It has been and still is an important cause of human morbidity and mortality. Assessing the burden of malaria accurately is difficult because most deaths from malaria occur at home with the clinical features of malaria being very similar to those of many other infectious diseases and good quality microscopy is available in only a few health centres [5]. The relation between malaria and malnutrition is important; if malaria is a major cause of malnutrition, it may be responsible for considerable indirect mortality that could potentially be reversed by effective malaria control [6]. Synergism between malnutrition and infection is responsible for much of the excess mortality among infants and preschool children in less developed regions. Infections are likely to have more serious consequences among persons with clinical and sub- clinical malnutrition and infectious diseases have the capacity to turn borderline nutritional deficiencies into severe malnutrition. Thus, malnutrition and infection can be mutually aggravating and can produce more serious consequences for the patient than would be expected from the summation of the independent effects of the two [7]. Nutritional anaemia is a priority of the World Health Organisation (WHO), and one of the most common causes of iron deficiency. Although malaria causes a large proportion of anaemia, the contribution of underlying micronutrient malnutrition to the overall burden of anaemia is often overlooked. Areas endemic for malaria often have a high prevalence of micronutrient malnutrition, creating a complex web of interactions with serious health repercussions. Several of these micronutrients such as vitamin A, vitamin E, zinc and iron play an essential role in immune functioning and have been implicated in resistance to many infectious diseases [8]. Iron deficiency is probably the most common of all nutritional deficiencies in the world [9]. In Cameroon, malaria remains the main cause of consultation in health facilities nationwide. There are no up-to-date epidemiological data available on malaria in many parts of the country and this is a serious handicap towards attempting to control the disease. The major factor that favours malaria parasite growth and transmission in Muea, the site of the study described herein, is poor environmental sanitation with pools of standing water and large numbers of dirt dumps and bushy areas around homes which all serve as breeding sites for the mosquito vector. Most of the inhabitants of Muea are subsistence farmers with carbohydrates and plant proteins being the most consumed diets. Inhabitants of Muea grow fruits and vegetables abundantly which are good sources of iron but these are rather sold than consumed by the local population thus contributing to the poor nutritive value of their foods. Muea with its heterogeneous and multiethnic population is, therefore, an ideal site to investigate the burden of malaria and malnutrition. The results from the study would provide necessary information to be used in developing effective strategies for the control of malaria and prevention of malnutrition. METHODS Study site Muea village is a semi-rural setting with a heterogeneous and multi-ethnic population of approximately 9,000 inhabitants. There are over 55 different ethnic groups residing in this area. Of the 9,000 inhabitants, 3500 are children <14 years old. About 80% of the inhabitants are farmers who have no steady source of income and live from hand to mouth. The principal food crops include cocoyam, cassava, maize, yams and vegetables. Fruits and vegetables are used as cash crops and are sold mainly to individuals that come from neighbouring cities and towns. The village is divided into ten quarters, each with a quarter head [10]. Study subjects The population was sensitized on the importance of the study after which children were recruited from 300 randomly selected homes in the ten quarters. To be included in the study, children had to be ≤14years old with or without signs of malaria and sickle test negative. Children who presented with fever, joint pains, malaise, abdominal pain, nausea and vomiting were considered to be symptomatic. Children weighing <5kg and those with severe malaria and other diseases requiring hospital admission were excluded from the study. Ethical clearance was obtained from the Provincial Delegate of Health, South West Province. Informed consent was obtained directly from the parents/guardian of the children. A questionnaire was administered to parents to obtain information on knowledge of malaria, kind of treatment given to their children and types of food generally consumed. This study was carried out from January to November 2006, to include the rainy season (April-September) which has been reported as the peak malaria transmission period in the locality [11]. Measurement of clinical parameters Body temperature was measured using a digital thermometer. A child was considered febrile when he/she had a body temperature ≥ 37.5 °C. Weight and height were measured using a Terraillon weighing scale (Terraillon, Paris) and a measuring tape, respectively. Ages of the children were obtained from their mothers and verified from their birth certificates. HAZ, WAZ and WHZ Z scores were computed based on the National Centre for Health Statistics (NCHS)/WHO growth reference curves using the nutrition module (Epi Nut) of the Epi Info 2000 programme [12]. Heights, weights and ages were related to references as standard deviations (SD). Children were malnourished when values were less than minus two (-2) SD. Children with values less than minus three (-3) SD were considered severely malnourished. Those with values between minus three SD and less than minus two SD were moderately malnourished. Spleen examination was carried out by palpation by the medical officer and the nurse of the health centre. The tip of the spleen was felt by pressing the abdomen under the coastal border. Splenomegaly was graded according to the classification of Hackett [13]. Laboratory investigations Blood collection Blood samples were collected by venipuncture and 5mL of venous blood was dispensed into anticoagulant (EDTA) tubes. Labelled samples were transported on ice in a cool box to the University of Buea malaria research laboratory for further analyses. Malaria parasite density The Giemsa-stained thin and thick blood films were examined microscopically under the 100x objective. Malaria parasites were counted against 200 leukocytes in thick films to obtain the parasite density. This was expressed as the number of parasites per microlitre (µL) of blood assuming an average leukocyte count of 8000 cells per µL of blood [14]. Slides were considered positive when asexual forms and/or gametocytes of any Plasmodium species were observed on the blood film. A slide was declared negative only after having examined at least 100 high power fields [15]. Parasitaemia was classified as low (< 500 parasite /µl of blood), moderate (501-5000 parasites/µl of blood) and high (>5000 parasites/µl of blood) [16]. Subjects found positive with a history of fever were treated with Amodiaquine/Artesunate combination therapy and paracetamol as recommended by the national policy for malaria treatment. Haemoglobin (Hb) concentration This was measured in the field using a Stanbio STAT-Site R Test Kit following the manufacturer's instructions (STAT-site MHgb Meter, Stanbio Laboratory, Texas, USA). Hb levels <11g/dl were classified as anaemic while those ≥11g/dl were considered non-anaemic. Further classification was done with mild, moderate and severe anaemia having values between 6.1-8g/dl, 8.1-10.9g/dl and <6g/dl respectively [17]. Packed cell volume (PCV) This was obtained by spinning blood in well-labelled capillary tubes filled to three quarters the length in a micro-haematocrit centrifuge (Hettich, Zentrifugen, Germany). The PCV values were read from the scale of the microhaematocrit reader and results were expressed as percentages [15]. Red blood cell count Red blood cells were counted using the method of Dacie and Lewis [18]. The mean cell haemoglobin concentration (MCHC), mean cell volume (MCV) and mean cell haemoglobin (MCH) were calculated using Hb, RBC and PCV [11] values. Classification of the type of anaemia (normocytic, microcytic and macrocytic) was based on the red cell indices. Determination of plasma iron concentrations Plasma iron concentrations were determined by spectrophotometry using the Iron Ferrozine reagent following manufacturer's instruction (FerrozineR, Elitech, France). Iron status was classified as low (<50µg/dl) and normal (50-168µg/dl). Statistical Analysis Statistical analysis was done using the SPSS TM (Statistical package for the Social Sciences, SPSS Inc., Chicago, IL, USA) package. Chi square (χ2) test was used to compare the prevalence of malnutrition and malaria infections as affected by sex and age. The analysis of variance (ANOVA) was used where appropriate to compare means. The Epi Info package (Epi Nut module) was used to analyze WAZ, WHZ, and HAZ Z-scores. Spearman's rank correlation was used to predict the relationship between plasma iron levels and malaria parasitaemia. All results were considered to be significant at 95% probability level (P <0.05). RESULTS A total of 339 children aged 0-14 were enrolled in the study, of which 183 were males (54%) and 156 (46%) females with an overall mean age in years of 4.98 + 2.87. Children were stratified into age groups with 12 (3.5%), 195 (57.5%), 98 (28.9%) and 34 (10%) being less than one, 1.1- 5 years, 5.1-9 years and 9.1-14 years, respectively. Malaria parasitaemia Of the 339 children examined, 326 were positive for malaria giving an overall prevalence of 96.2%. The mean parasite density was higher for females than males and also highest in the 1.1-5 year age group when compared with the other age groupings (Table 1). However, this difference in mean parasite densities was not statistically significant (P>0.05). Of the 326 malaria infected individuals, 135 (41.4%), 164 (50.3%) and 27 (8.3%) had parasite loads of ≤500, 501-5000 and >5000 parasites per µl of blood, respectively. Again children between 1.1-5 years carried higher parasite loads when compared with those in the other age groups although this difference was not statistically significant (P>0.05). More males carried higher parasite loads than females. Overall, children less than five years of age had a GMPD of 822 ±117467 when compared with 622 ± 2052 for those older. The prevalence of splenomegaly was 23.3% (79/339). As expected, more children (78) less than or equal to nine years had enlarged spleens compared with only one in the greater than nine years age group. The difference was statistically significant (P = 0.001). Marked splenomegaly (Hackett score greater than or equal to two) was very frequent in younger children (20%). Malaria and Hb concentration The mean Hb concentration was 9.29±1.8g/dL (range 4-14.1g/dL). It was observed that 276 (81.4%) children had anaemia compared with only 63 (18.6%) who were non-anaemic. Of the anaemic cases 54 (19.6%) 199 (72.1%) and 23 (8.3%) were classified as mild, moderate and severe anaemia, respectively. The mean Hb concentration for anaemic children was 8.77g/dl compared with 11.56g/dl for nonanaemic children and this difference was highly significant (P<0.005). The GMPD for anaemic cases (751 ± 9853; range 40-153190) was higher than for normal cases (710 ± 3148; range 80-21280) but this difference was, however, not statistically significant (P>0.05). There was a negative correlation between parasite density and Hb concentration (r = -0.14). Malaria and red blood cell indices The majority of anaemic children 231 (83.7%) had microcytic anaemia. The GMPD for children with microcytic anaemia was generally higher (725.99 ± 29175.89) than that for individuals with normocytic anaemia (660.96±1754.29). Microcytosis decreased with increased age with children less than five years having the highest prevalence of microcytosis. Iron status and malaria There were 199 children (58.7%) with iron deficiency and 140 (41.3%) with normal iron concentrations. The mean iron concentration was 53.64 + 32.97µg/dl. Most of those who were iron deficient were children between 1.1 - 5 years. Of the 199 iron deficient children, 192 (96.5%) had malaria. More children (38.6%) with high parasite densities were iron deficient compared with 20.1% with low parasite densities. There was a negative correlation between malaria parasite density and the iron status of individuals (r =-0.037). Malnutrition, malaria, anaemia and iron levels The overall prevalence of malnutrition was 58.1 % (197/339). Of the 197 malnourished children, 23.6% were wasted (<-2SD weight-for-height Z score), 26.5% underweight (<-2SD weight-for-age Z score) and 49.9% stunted (<-2SD height-forage Z score). The highest prevalence of malnutrition (75%) was recorded in the <1 year age range while the lowest prevalence (6.6 %) was observed in those between the 9.1-14 years age group (Table 2). Although a decrease in prevalence of malnutrition with increase in age was observed in the study population, this was not statistically significant). The prevalence of malaria among malnourished children was 97%. There was no significant difference (P>0.05) in malaria prevalence between malnourished and well-nourished children (Table 3). The malaria positive children however, were 2 times at odds of being malnourished than the malaria negative children (Odds ratio at 95% confidence interval is 2.26; 0.73-7.07). Although not significant (p>0.05), hyperparasitaemia prevalence (high parasite density) was higher in malnourished children when compared with nourished children. There was a negative correlation between nutritional status and parasitaemia (r=-0.034). No significant difference was observed in the frequency distribution of malnourished children in the different iron level classifications (P>0.05). The children with low iron status were 0.7 times more likely to be malnourished than those with normal iron status (odds ratio at 95% confidence interval, 0.78; 0.51-1.21). Of the 191 children who had both malaria and malnutrition 117 (61.3%) had lower than normal iron status. DISCUSSION Malaria and malnutrition are serious health problems in many tropical countries. Our study revealed a malaria prevalence of 96.2% in rural Muea. The prevalence of 23.3% for children with enlarged spleens confirms that malaria is endemic in Muea. Children less than five years were observed to be highly infected with malaria parasites as compared to older children. The finding that 68.4% of children were asymptomatic indicates that children in the study area seem to have acquired the ability to tolerate parasites without having fever. Among those diagnosed with malaria 91.7% carried parasite loads ≤ 5000 parasites/µl of blood. This corroborates findings by Biemba who reported that in highly endemic areas, where there is constant repeated transmission and infection, a low-grade asymptomatic parasite load remains the common phenomenon [19]. The high number of afebrile cases is, however, a cause for concern because many parents/guardians in Muea seek treatment only when the child has persistent high fever after self medication with herbal remedies or drugs from questionable sources. This practice may have serious adverse consequences if, their health/treatment seeking behaviours are not modified through proper child health education. The high prevalence of anaemia in malaria cases suggests that malaria related anaemia is a problem in Muea. Hypochromia and microcytosis were prominent morphologic findings in children with anaemia. The prevalence of microcytosis decreased with an increase in age and this could partially be attributed to a gradual acquisition of immunity. It was observed that while the inhabitants of Muea were aware that malaria existed in the community, they did not realize the importance of prompt treatment. Most parents treated their children at home using mostly traditional herbs or drugs of questionable quality purchased from street vendors. Children were usually brought to the health centre only when home treatment failed. Lack of proper education and poverty are contributing factors to these attitudes and practices. Nutrition plays a major role in maintaining health, and malnutrition appears to generate vulnerability to a wide variety of diseases and general ill health [20]. The high prevalence of malnutrition (58.1%) with stunting more common than underweight and wasting, most likely reflects the low socioeconomic status of the inhabitants. Children in the < 1 age group had a higher prevalence of malnourished children when compared with other age groups. This may be due to the lack of adequate complementary foods, both in nutrient content and amount of intake to supplement breast milk. Iron deficiency is a public health problem in Saharan and Sub-Saharan Africa. The prevalence of iron deficiency in Muea was higher (58.7%) compared to a prevalence of 40% and 50% reported in Tanzania and Nigeria, respectively [21]. Most of the children in Muea with iron deficiency were less than five years of age and iron levels were observed to increase with age. Iron deficiency is common in African children particularly in their second year of life. This has been related to prolonged breast-feeding. The low iron content of breast milk, the lack of other iron rich foods, and the age-related increase in iron requirements predisposes children to the depletion of iron stores [22]. The majority of the population of Muea feeds on carbohydrates and plant proteins, which are not favourable for iron absorption when compared with vegetables and animal protein. A greater majority of children deficient of iron also had malaria and there was a negative correlation between malaria parasite density and plasma iron concentrations. It has been reported that individuals with malaria have lower plasma concentrations of several micronutrients when compared to controls [23]. This decrease in iron levels during acute malaria has been attributed to immobilization of iron in haemazoin complexes and reduction in intestinal iron absorption [24]. CONCLUSION Malaria and malnutrition are highly endemic in children ≤14 years residing in Muea. Iron deficiency and malaria related anaemia were also found to be prevalent in the study population. There is a strong need to educate the public on the benefits of prompt and proper treatment of malaria. The population should be encouraged to eat vegetables and fruits which are readily available locally so as to augment the nutritive quality of foods consumed and therefore improve on the nutritional status of children in the area. This would be an effective strategy to reduce direct or indirect morbidity and mortality from malaria and malnutrition. ACKNOWLEDGEMENT The authors are grateful to the village chief and entire population of Muea for participating in the study. This work received financial assistance from the University of Buea Research Grant. REFERENCES
The following images related to this document are available:Photo images[nd08024t3.jpg] [nd08024t2.jpg] [nd08024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}