 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food Agriculture Nutrition and Development, Vol. 9, No. 3, May, 2009, pp. 814-829 Congenital malformations Among Newborns In Kenya Muga RO1*, Mumah SCJ2. and PA Juma3 1Professor of
Paediatrics, Great Lakes University of Kisumu (GLUK). P.O. Box 2224, Kisumu, Kenya. Code Number: nd09027 ABSTRACT Available literature suggests that congenital malformations are a major cause of prenatal infant deaths and postnatal physical defects [1, 2]. Therefore, a study was conducted to determine the patterns and incidence of congenital malformations at birth in newborns in Kenya and thereby analyze associated predisposing factors in their mothers. This single cross-sectional survey adopted the quasi-experimental study design to investigate a total of 7,355 consecutive births at the maternity unit of Kenyatta National Referral Hospital over a period of uninterrupted 12 months beginning 8th September to 7th September of the following year. Data collection involved clinical examination of the malformed newborns for final diagnosis using a standard proforma. The study included a control group of new born babies selected systematically among babies who were born during the same study period but had no recognizable defects at birth (n=210). These included normal babies delivered immediately after the malformed newborns. The experimental group comprised the malformed babies (n=207). Mothers were also interviewed for demographic information and data on life style and behavioral risk factors. In this paper only the results of the experimental group are described. A total of 207 malformations were documented. Results showed overall incidence of externally discernible malformations of 28.1 per 1000 total births (28.1/1000). The incidence of major malformations was 15/1000 births. Malformations of musculoskeletal system were the most frequently observed, accounting for 33.9% of all the major malformations, followed by malformations of the central nervous system (28.6%). Polydactyl was the most common single malformation with an incidence of 10/1000 total births. Neural tube defects (with an overall incidence of 4.6/1000 births) and chromosomal disorders were also common. On the overall, congenital malformations occurred in proportions that were comparable to other findings in Africa and other parts of the world. These findings highlight the need for stepping up nutritional prevention efforts, for instance, folic acid supplements; strengthening surveillance to monitor trends; and the establishment of a genetic centre in Kenya in order to strengthen local capacity for chromosomal studies, prenatal diagnosis, and genetic counseling on these complex issues. Key words: Congenital malformations, polydactyl, birth defects. INTRODUCTION Congenital malformation (a birth defect or a congenital anomaly) is a physical defect present in a baby at birth, irrespective of whether the defect is caused by a genetic factor or by events occurring/existing before or at birth. In a malformation, the development of a structure is arrested, delayed, or misdirected early in embryonic life and the effect is permanent. Congenital malformations can involve many different organs including the brain, heart, lungs, liver, bones, and intestinal tract. These defects can occur for many reasons including inherited genetic conditions, poor diet, toxic exposure of the fetus for example, to alcohol, birth injury and, in many other cases, for unknown reasons.[1] All parents are at risk of having a baby with a birth defect, regardless of age, race, income or residential status.[2] This paper describes a study carried out to determine the pattern of congenital malformations at birth in newborns, thereby analysing the associated predisposing factors in their mothers with a keen focus to nutritional related variables. The study was carried out at Kenya National Hospital (KNH) in Kenya. Available literature shows that congenital malformations contribute highly to prenatal mortality and postnatal physical defects [3, 4,5]. In the US for instance, 2-3% of babies are born with a major congenital malformation.[1]; these include heart defects, cleft lip or palate, Downs syndrome, spinal bifida, and limbdefects [6]. Sixteen% of all neonatal deaths in Queensland were due to congenital malformations [4]. Additionally, 20 percent of late infant deaths were attributable to major congenital malformations in Queensland (ibid). [4]. Literature further indicates that congenital malformations are present in one of every three babies that die in the world [ 7 ] and their effects on a child vary depending greatly on the severity of the defect and whether or not other medical problems are present. Thus, it was interesting to determine the pattern of congenital malformations at birth in newborns and analyse associated predisposing factors in their mothers. METHODOLOGY The study was a prospective survey conducted at the maternity unit of Kenyatta National Hospital (KNH), which is Kenya’s leading referral hospital in Nairobi. The study covered an interrupted period of 12 months from (8th September 1983) to (7th September 1984). Data on 7,355 consecutive births were collected during the study period. A total of 207 birth defects were identified. Malformed babies (n=207) were clinically examined for final diagnosis using a standard proforma (with demographic indicators of the newborn, information on clinical examination of the ears, eyes, mouth, neck, chest, CVS, abdomen, genitalia, extremities, CNS and clinical gestation). Major congenital malformations included defects present at birth which may be fatal and/or handicap the patient throughout life. Minor congenital malformations were classified as those defects with no handicap, for example, skin tag and birth mark. If a newborn had two or more malformations, the system with the most obvious or major malformation was adopted. For instance, a baby with a meningomyeloceole and talipes was classified under Central nervous system malformation and counted only once. In cases where a group of malformations constituted a known syndrome or chromosomal disorder, then the syndrome was taken as the diagnosis. Further, only those cardiac malformations which were either confirmed by a pediatric cardiologist or discovered at autopsy were included in the analysis. Mothers were interviewed with the help of a questionnaire. Information gathered included demographic profile, data on lifestyle and behavioral risk factors including smoking during pregnancy, alcohol consumption and use of contraceptives. Other relevant information included medical history of illness, treatment history, past occurrence of similar birth defects, birth order of index baby and father’s age, and social habits. In addition, photographs of the malformed baby were taken for detailed documentation (after obtaining informed consent from the mother). Babies with major congenital malformations were followed up, with daily reviews in the hospital for the first 28 days post-delivery, to determine neonatal outcomes. At discharge, the babies were booked at the paediatric demonstration clinic for follow- up review at the end of the first month of life. Any baby requiring surgical or other specialist attention at this stage was referred to the respective clinic for follow up. Death of a baby from the study population while still in the hospital resulted in a postmortem examination to establish immediate cause. Descriptive analysis was performed to determine distribution pattern, incidence of malformations and neonatal outcomes. Malformations were classified into major and minor ones. RESULTS During the study period (September 1983 and September 1984), there were 7,230 deliveries resulting in 7,355 newborns (Table 1). Newborns numbering 207 were malformed with an overall incidence of 2.8% of all live births. Stillbirths were 304 (4.1%) out of which 17 (5.6%) were malformed while 1.5% of the malformations were major. Peak reproductive age group was 20-24 years (range 16-44 years) and mean age of mothers with malformed babies was 26 years (Table 2). Table 1: Outcome of deliveries by sex.
Table 2: Mothers’ age.
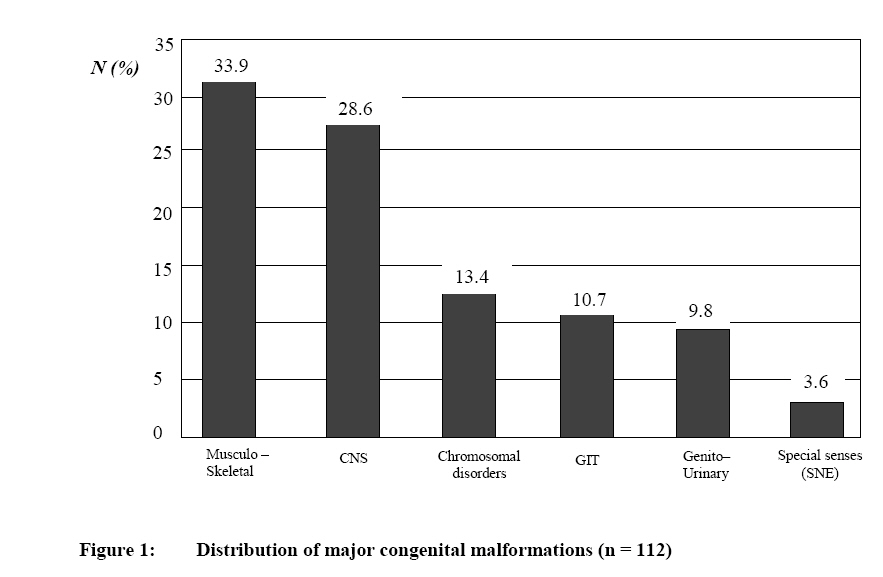
Nearly 8% of the babies with major congenital malformations were of low birth weight (<2500gm). Musculoskeletal system was the commonest of the malformations, contributing 33.9 % (38) of all major malformations followed by the CNS 28.6% (32) (Figure 1). Malformations of special senses (skin, nose and ear) were the least common. The overall incidence of Musculo-skeletal (MSS) malformations was 17.3/1000 total births, the commonest malformation being polydactyl (59.1% with an incidence of 10.2/1000 births, twice as common in males as females (α=0.05, p<0.001) (Table 3). Additionally, 40.4% of the babies who had Musculo-skeletal malformations were low-birth weight as opposed to the 11.9% of their controls (α=0.05, p<0.001). An analysis into the relationship between mother’s age and babies born with MSS malformations (polydactyly excluded) revealed that a greater majority of MSS malformations (69%) occurred in mothers aged between 20-29 year. Table 3: Distribution of musculo-skeletal malformations.
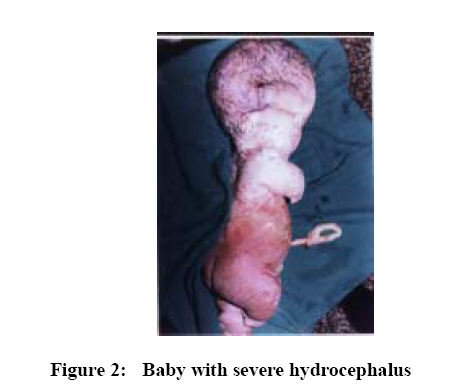
There were 75 cases of polydactyly (44% of which involved both upper and lower limbs attached on the ulnar border of the 5th finger, 34% unilateral left ulnar border) with an incidence of 10.2/1000 births. Of all these cases, 62.7% had positive family history of polydactyly. Some 8% of the babies with polydactyly had other associated major malformations, the commonest being hydrocephalus followed by chromosomal disorders. There were, however, no statistical differences in the birth order of babies born with polydactyly. Further, polydactyly occurred in all maternal age ranges (with slight increase in cases born to mothers aged 20-24, corresponding with the peak reproductive age range). Overall incidence of CNS malformations was 4.6/1000 total births with hydrocephalus being the most common CNS anomaly, contributing 32.4% (with an incidence of 1.5/1000 births) (Table 4). About 53% of all the CNS malformations occurred in association with the other system involvement (Figure 2). Table 4: Malformations of the CNS.
Seventy six percent of all CNS malformations occurred in mothers below age 30 years, with an increment in age, especially from 35 years. Findings regarding the birth order of babies with CNS malformations showed that birth order “Four” (4) contributed 55.2% of the cases. Down’s syndrome was the leading chromosomal defect contributing to 6 out of the 15 cases with an incidence of 0.82/1000 total births (Table 5). Overall male-female ratio was 2:3, far above the expected 1:1, indicating female preponderance in chromosomal disorders. One hundred and twelve babies had major congenital malformations and 15.1% (17) of the major congenital malformations were among stillborn babies. Two babies had cardio-respiratory problems; one had TGA and the other diaphragmatic hernia. A baby in the special senses category had bilateral choanal atresia and two babies had ear malformations associated with internal abnormalities. Some malformations found at autopsy were associated with external presenting malformations (Table 7). Table 5: Chromosomal defects.
Fifty deaths occurred among the 95 live born babies with major malformations giving a fatality rate of 44.6% (Table 6). Fifty percent (25/50) had CNS malformations of whom 17 were stillborn. CNS defects contributed to most deaths followed by chromosomal (16%) and musculo-skeletal (14%) defects. Based on 7355 births recorded during the study period, the mortality rate due to congenital malformations was 0.7% of all births. Table 6: Distribution of deaths according to system involvement.
Table 7: Malformations found at autopsy in association with external presenting malformations.
Table 8: Frequency of congenital malformations found in some prospective studies in different populations.
DISCUSSIONS The incidence of major malformations in this study was 1.5% of total births. This is comparable to findings of other studies [ 8, 9, 10, 11]. However, other studies have reported higher rates. MacKeon and Record [14] reported two times as many malformations. In another study, McIntosh, et al, could only diagnose 43.2% of all malformations at birth yet at the end of one year follow-up, the figure had risen to 97%.[3]. Similar findings were reported by Neel showing that the incidence of congenital malformations in live births in a given population tend to increase with follow-up duration (age) [9]. The incidence found in the present study and those of the prospective studies in different populations were comparable.(Table 8). There were more malformed male than female infants; however, the difference was not statistically significant.[3, 12,13]. The number of malformed babies appeared to increase with increasing maternal age especially from 35 years and above, who accounted for 13.4% of all malformed babies. Musculoskeletal malformations were commonest. Polydactyly accounted for 59.1% of all musculoskeletal malformations, and 10.2 per 1000 births. It has been recorded since ancient times in the Bible, 11 Samuel 21:20, “And there was a man of great stature who had six fingers and six toes on every hand and foot—“. Drew et al. [17], in Melbourne found polydactyly among newborns at a rate of 0.6 per 1000 births. This was nearly sixteen times lower than the rate in the current series. It is known to be inherited by simple dominant gene mechanism although the condition may be present in all people heterozygous for the gene and the manifestation is very variable. Family history is positive in many cases [18]. Among the CNS malformations, findings showed a combined incidence of anencephaly and myeloceole of 1.9 per 1000 total births. This is consistent with findings of Mati[ 15] in a study in Nairobi which found a combined incidence of 1.1 per 1000 total births. It suffices to say that neural tube defects do occur among Africans contrary to the previous suggestions of Simpkiss and Lowe [16]. CONCLUSION Major newborn malformations are often fatal, as illustrated in this study. Prevention, therefore, should be prioritized to the extent possible. There is evidence that improvement of nutrition during conception and during the first trimester can reduce the risk of fatal birth defects [6, 7, 19, 20, 21 ]. Appropriate nutritional supplementations are recommended to reduce the risk of congenital malformations; establishment of a genetic centre in order to facilitate chromosomal studies, prenatal diagnosis of congenital malformation [22, 23, 24, 25 ] and genetic counseling in Kenya. There is also need for improved surveillance system for congenital malformations in hospital births to monitor trends in view of increasing environmental pollution due to rapid industrialization in Kenya and in the rest of the developing world. ACKNOWLEDGEMENTS We take this opportunity to acknowledge our indebtedness to those who assisted us in this research. To the staff who worked in the study areas, especially nursery and labour wards, we thank you very much for your support. To mothers whose newborns were the subjects of this study, we are proud of you because without you, this study could not have been done. REFERENCES
© Copyright 2009 - Rural Outreach Program The following images related to this document are available:Photo images[nd09027f1.jpg] [nd09027f2.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}