 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food Agriculture Nutrition and Development, Vol. 9, No. 7, Oct, 2009, pp. 1498-1510 Evaluation Of Some Maternal And Socio-Economic Factors Associated With Low Birthweight Among Women In The Upper East Region, Ghana Amagloh FK*1,Williams AA2 and I Angbing3 *Corresponding author email: francisamagloh@yahoo.com Code Number: nd09079 ABSTRACT The birth of a child all over the world often comes with joy. Birthweight is a strong predictor of an individual baby’s survival and a person’s personality. It is one of the key indicators of the health and viability of the newborn infant. It is desired that birthweight should be in the range of 2.5 kg to 4.0 kg. Low birthweight has been defined by the World Health Organization (WHO) as weight at birth less than 2.5 kg. This study seeks to evaluate some of the factors that affect birthweight in the Upper East Region of Ghana. One hundred mothers with singleton live births were sampled and interviewed at birth maternity blocks of Bolgatanga Regional Hospital, Bolgatanga and War Memorial hospital, Navrongo. The factors considered include: gestational age, gestational weight gain, maternal educational level, parity, cigarette smoking habits, type of fuel used for cooking, maternal drinking habits, type of physical exercise undertaken, period of rest during pregnancy, and fundal height. The average birthweight of infants born in the Upper East Region was 2.98±0.53 kg. Correlating the variables, it was observed that most of the above-mentioned factors correlated linearly but insignificantly (p > 0.05) with birthweight. Results of multiple regressions conducted established that maternal educational level significantly determines birthweight (β = 0.34, p = 0.001). Within the limits of this research, maternal educational level contributed significantly in predicting birthweight in the region followed by duration of rest during pregnancy, pre-pregnancy weight, income level, and type of fuel used for cooking. The type of fuel used for cooking in the region contributed to low birthweight infants (β = -0.06, p = 0.567). The estimated weight gain during pregnancy and healthy lifestyle recorded in this study could be responsible for the attainment of appropriate birthweight specified by WHO. It is recommended that education of the girl-child should be taken seriously in the region. Key words: birthweight, pregnancy, maternal, education, fuel BACKGROUND Childbirth all over the world mostly comes with joy not only for the infant’s parents but the whole family at large and also attracts attention from both close relations and community members. In Ghana, to be specific, the family members, especially the women clad themselves in white clothing from headgear to footwear. However, the course of pregnancy is not given such needed attention. The onus lies solely with the woman who is pregnant despite the fact that scientific literature has indicated that the outcome of pregnancy depends on both external and internal factors experienced by the pregnant woman [1-5]. In Ghana, the issue of birthweight and factors influencing it has not received the much needed attention. This should not be the case because birthweight is a strong predictor of an individual baby’s survival and a person’s personality [6,7]. The recommended weight at birth should be in the range of 2.5kg to 4.0kg [8]. The high rate of low birthweight (LBW), defined as weight at birth less than 2.5kg is a major problem in developing countries [9]. From 1998 to 2004, Ghana recorded higher LBW cases of 16% compared to the average of 14% for sub-Saharan Africa [10]. Cases of low birthweight are more common in the developing countries than in the developed countries [9, 11]. Though the major and primary determinant of birthweight is gestational age [12, 13], there are other secondary factors that also bear, either directly or indirectly on determining the weight of a baby at birth. These are maternal weight gain, pre-pregnancy weight, maternal height, parity, age, marital status, cigarette smoking, heredity, gender of baby, working hours and various socio-economic factors [11, 14, 15, 16]. In developing countries, the major determinants of LBW babies are racial origin, nutrition, low pre-pregnancy weight, short maternal stature, and malaria [17]. A WHO Collaborative Study of Maternal Anthropometry and Pregnancy Outcomes reported that weight gained at 5 or 7 lunar months was the most practical screening for LBW and Intrauterine Growth Retardation (IUGR) [18]. The reduction of the incidence of low birthweight also forms an important component of the Millennium Development Goals (MDGs) on child health. Activities towards the achievement of the MDGs will need to ensure a healthy start in life by making certain that women commence pregnancy healthy and well nourished, and go through pregnancy and childbirth safely [9]. Low birthweight is, therefore, an important indicator for monitoring progress towards these internationally agreed-upon goals. Earlier works stated the birthweight of infants in Ghana ranged from 2.00 to 3.00 kg [19, 20]. It is in this light that this research seeks to investigate the effect of some of the factors that affect birthweight in the Upper East Region, one of the poorest regions in Ghana. MATERIALS AND METHODS Study Design and Area This was a cross-sectional survey study. The study was conducted in a district and a municipality, both in the Upper East Region of Ghana; these are the Kassena-Nankana District, which shares boundaries with Burkina Faso to the North, Bongo District and Bolgatanga Municipality to the East, Builsa and Sisala Districts to the West and Mamprusi West District to the South. The Bolgatanga Municipal Assembly which shares boundaries with Bongo District (Zoko) to the North, Kassena-Nankana District (Kandiga) to the East, Talensi-Nandam District to the West and Mamprusi West District (Walewale) to the South. Data were collected from the maternity blocks of War Memorial Hospital (located in Navrongo, the capital of the Kassena-Nankana District) and Bolgatanga Regional Hospital (located in Bolgatanga, the Upper East Regional capital). The former health facility offers secondary clinical and public health services to the people in the District and its environs while the latter doubles as the referral hospital for the Region and a teaching hospital for Bolgatanga and Bawku Nursing Training Schools, Midwifery Training School, Bolgatanga and Navrongo Community Health Centres. Majority of the people in the study area are subsistence farmers while few of them are self- employed or civil servants. Sample Size Determination A sample size of 100 subjects was used for the study on the basis of 6% precision at an expected prevalence (LBW cases) of 10.33%. A population of 73,248 women in the fertility age group (15-49 years) in both the Bolgatanga Municipality and Kassena-Nankana District extrapolated from Ghana Demography and Health Survey (GDHS) 2004 was used in calculating the sample size at 95% confidence level and a margin of error of 5% [21]. In determining the sample size, the formula used was: Where n= sample size N=Total Population =73,248 P= Expected proportion in the population =10.33% Z= Z-value (corresponding to the confidence level of 95%) =1.96 d= Absolute precision =6%
Data Collection and Analysis Using purposive sampling, mothers with singleton deliveries were selected and interviewed at delivery between January and May 2007. Fifty (50) respondents were interviewed at each maternity block. Both primary data (obtained through interviewing of mothers) and secondary data (extracted from mothers’ antenatal records) were collected. The SPSS version 13.0 was used for data entry and analysis [22]. According to GDHS report, the percentage of women in Upper East Region who had no idea of the birthweight of their baby is 85.9% (either child record is missing or weight at birth not recorded) [21]. It would, therefore, be inappropriate to conduct such a study without using mothers who have medical history recorded during the course of their pregnancy. Descriptive statistics (means, modes, standard deviations and percentages), cross tabulations, correlation, and multiple regression were performed to assess relationship of some factors to birthweight. RESULTS Characteristics of the Study Population From Table 1, the mean maternal age for the 100 mothers was 27 yr +5.43. The mean pre-pregnancy weight was 53.55 kg +11.33 with an estimated maternal weight gain of 9.27 kg +3.98 which is comparable with the recommended weight gain of 9.8 kg (recommended lower limit) during pregnancy [2, 23]. The average gestational age was 36 wks +0.56 indicating that most of the respondents did not have full term pregnancy. The mean fundal heights in the first, second and third trimesters were 11.71 cm +0.56, 24.30 cm +2.85 and 35.77 cm +3.73, respectively. Five (5) percent of mothers interviewed were hypertensive. One (1) percent was diabetic. Three (3) percent had heart related diseases. None of them was a sickle cell anaemic patient who needs critical observation during pregnancy. Nineteen (19) percent were treated for malaria during pregnancy. The educational level of the respondents was low. Almost 50.0% of them were illiterate (defined as not having any formal education or was educated up to primary level). Only 5.0% had schooled up to the secondary level or above. The birthweight of 2.98 kg +0.53 is consistent with earlier findings in Ghana [19, 20]. Eighty-seven (87) percent of the infants were normal birth cases (2.5 kg - 4.0 kg), 12.0% of them were low birthweight cases (below 2.5 kg) while 1.0% of the infants was macrosomic (birthweight > 4.0 kg). Table 1: Characteristics of the study population
Effect of type of fuel used for cooking, cigarette smoking and alcohol consumption on birthweight About 91.0% of mothers used the cheapest source of fuel (firewood and charcoal) for cooking when pregnant (Table 2). Only 2.0% of them used Liquefied Petroleum Gas (LPG) for cooking. It can be seen from data in Table 3 that only one of the mothers interviewed smoked cigarette or drank alcohol during pregnancy. Also, 86.0% of the mothers who did not smoke or take alcohol had infants with birthweight in the recommended range of 2.5 kg to 4.0 kg. Table 2: Birthweight compared with type of fuel used for cooking during pregnancy
* Liquefied Petroleum Gas Table 3: Birthweight compared with smoking and drinking habits during pregnancy of respondents
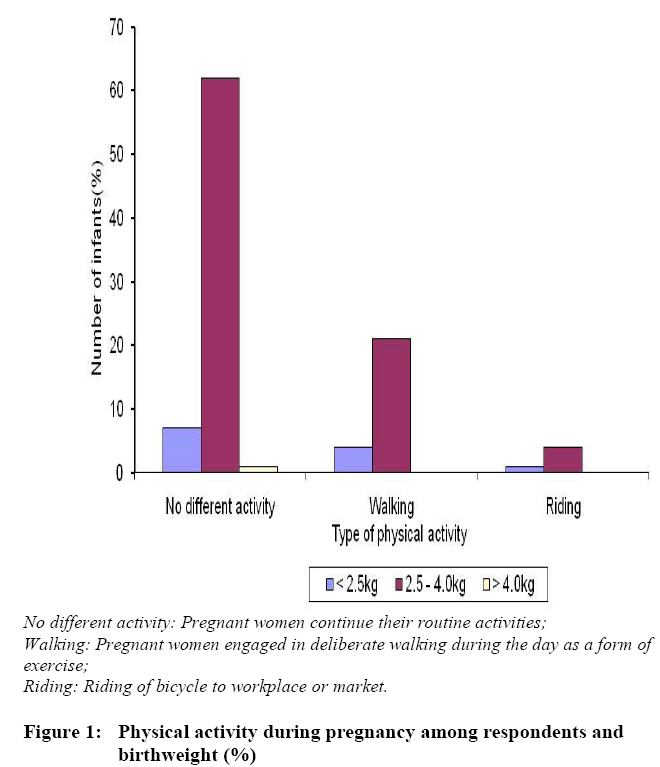
Physical activity of mothers and birthweight Figure 1 highlights the effect of physical activity engaged in during pregnancy and its effect on birthweight. Twenty five (25) percent of the respondents engaged in scheduled walking sessions during the day as a form of exercise in addition to their routine activities while 70% of them did not engage in any planned physical activities. The women who did not embark on any scheduled exercise had the highest number for low birthweight infants; the only macrosomic case was also in this group. Relationship between maternal factors and birthweight Table 4 shows the correlation between birthweight, pre-pregnancy weight, fundal height in three trimesters, maternal age, gestational age and income. The negative sign shows inverse relations and vice versa. All the variables were not strongly correlated. Birthweight, however, significantly correlated with the first and third trimester’s fundal height (p < 0.05). The output in Table 5 shows that all the combinations of the independent variables gave enough evidence (p = 0.008) for their use in predicting birthweight. The effect on birthweight by factors considered were as follows: maternal educational level (ß = 0.339, p = 0.001), duration of rest during pregnancy (ß = 0.144, p = 0.142), pre-pregnancy weight (ß = 0.070, p = 0.469), income level (ß = 0.085, p = 0.395), and type of fuel used for cooking (ß = -0.059, p = 0.567). The type of fuel used for cooking which was mainly firewood was the only one among that factors considered which negatively affected birthweight. Nevertheless, maternal educational level singly contributed to prediction of birthweight (p = 0.001). Table 4: Correlation matrix for some determinants of birthweight
* Correlation is significant at the 0.05 level
(2-tailed) Table 5: Simultaneous multiple regression analysis summary for maternal educational level, duration of rest from work during pregnancy, pre-pregnancy weight, fuel, and income predicting birthweight
Note: Adjusted R2= 0.11; p = 0.008 DISCUSSION The mean pre-pregnancy weight of 53.55 kg ± 11.33 indicates that some of the women in this study were at risk of delivering LBW babies; however, the concomitant weight gained of 9.27 kg ± 3.98 coupled with the healthy lifestyle (only 1% smoked or drunk alcohol frequently during pregnancy) observed in this study could have contributed to the high proportion of normal birthweight babies recorded in this study (12.0% vs. 88.0%, respectively). The progressive increase of fundal height as pregnancy proceeds makes it a good indicator for monitoring its progress. Findings of this research are consistent with use of fundal height to estimate gestational age [9]. Most of the mothers gather the firewood for fuel from farms at no cost, indicating the low socio-economic status of most of the inhabitants of this region. It is worth noting that out of the 12% LBW cases observed in this study, none was associated with the mothers who use Liquefied Petroleum Gas (LPG) which generates virtually no smoke compared to fuel such as firewood and charcoal when used for cooking. The highest (6.0%) incidence of LBW cases was associated with mothers who use firewood for cooking during pregnancy. The firewood when used for cooking generates smoke which the mothers unavoidably inhale. The effect of cigarette smoking on the incidence of LBW deliveries have been reported elsewhere [14]. Moreover, the energy expended by the women in gathering firewood could be implicated in the LBW cases. The type of fuel used for cooking (in terms of the amount of smoke generated) among pregnant women and birth outcomes needs further consideration, since it was observed that fuel used during cooking contributed negatively to birthweight. Most women in this region are engaged in low physical activity like walking to farms and work places. This could have attributed to the inability to clearly use level of exercise to establish effect on birthweight as was observed in other studies [24]. Since maternal educational level contributed significantly to the determination of birthweight, there is the need to give attention to female education in the region since about 50.0% of the respondents were illiterate and only 5.0% had educational training up to secondary level and above. CONCLUSION The estimated weight gain during pregnancy and healthy lifestyle recorded in this study could be responsible for the attainment of the appropriate birthweight specified by the World Health Organisation. The low variability in birthweight that was explained by independent variables used in all the regression models suggests that there were some confounding factors not accounted for. Within the limits of this research, maternal educational level contributed significantly in predicting birthweight in the region. RECOMMENDATION With reference to the research findings, the girl-child education should be encouraged in the region since maternal educational level has significant contribution in predicting birthweight. REFERENCES
© Copyright 2009 - Rural Outreach Program The following images related to this document are available:Photo images[nd09079f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||


{kind=link}