 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food Agriculture Nutrition and Development, Vol. 9, No. 9, Jan, 2009, pp. 1845-1858 Urinary Schistosomiasis And Iron Deficiency Anemia Among Malian School Children Ayoya MA*1, Koné KM2 and AK Traoré2 1 UNICEF Country Office, 73 Lodi Estate, New
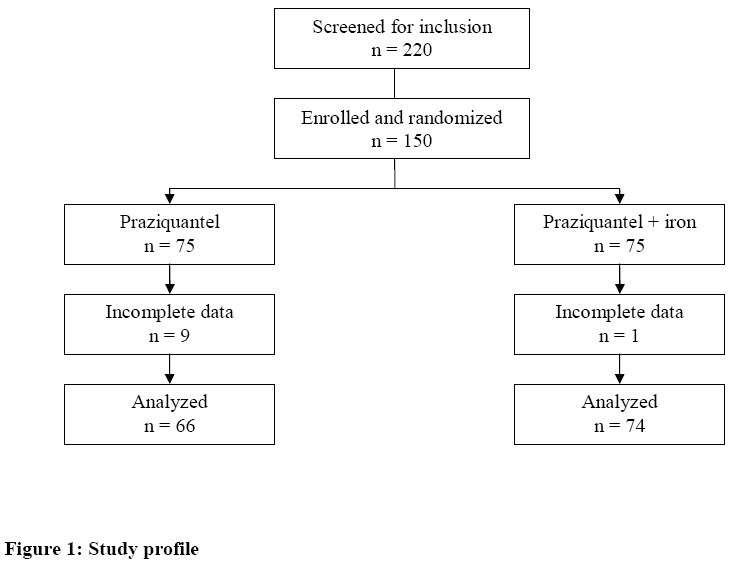
Delhi 110003, India. Code Number: nd09108 ABSTRACT Anemia continues to be a major public health problem in many countries. The prevalence and intensity of urinary schistosomiasis, which contributes to anemia, often peak at school age adding to that age group’s nutrition and disease burdens. However, unlike malaria and hookworm infections, little is known on the role of urinary schistosomiasis in iron deficiency anemia. The objective of this study was to assess the prevalence of iron deficiency anemia and the effect of iron supplementation on hemoglobin (Hb) and serum ferritin (SF) levels among school children infected with Schistosoma haematobium in Bamako, the capital city of Mali. A total of 150 anemic school children between 7 and 12 years were randomly assigned to receive either 40mg/kg of praziquantel or 40mg/kg of praziquantel (P) + daily 66 mg of iron (Fe), five days a week for three months. Hb and SF were measured at baseline and at 6 and 12 weeks of the intervention. Only children who had complete Hb and SF data at each stage of the trial were included in the statistical analyses (n = 74 in the P+Fe group; n = 66 in the P group). At baseline, mean Hb (g/dl) was 10.53±0.93 in the P group and 10.47±1.17 in the Fe+P group; mean SF (µg/l) was 34.39±37.58 in the P group and 29.82±23.34 in the Fe+P group, and the prevalence of iron deficiency was 17.2%. At 6 and 12 weeks of the intervention, there was an important reduction in anemia and in iron deficiency in both treatment groups. Mean Hb (g/dl) was higher in the Fe+P group (11.63±0.88 and 11.55±0.94) than in the P group (11.14±0.98 and 10.84±0.86) at 6 and 12 weeks, respectively. Mean SF (µg/l) was also higher in the P+Fe group (74.26±40 and 100.29±53.92) than in the P group (40.65±35.63 and 40.70±29.57) at 6 and 12 weeks, respectively. In these Schistosoma haematobium infected children, iron deficiency was prevalent and treatments with P alone or in combination with Fe supplementation were able to increase hemoglobin and iron stores. Neither P nor P+Fe by alone completely reversed anemia in this sample population. Key words: Urinary schistosomiasis, anemia, children, Mali INTRODUCTION Anemia continues to be a major public health problem in many countries. The World Health Organization (WHO) estimates that globally anemia affects 1.62 billion people with the highest prevalence (47.4%) found among school children [1]. In Africa, 41% of individuals are affected and the proportion of anemic pre-school children (68%) is the highest in the world [1]. In Mali, the prevalence of anemia among school-age children is estimated to be 56% [2]. In this age group, anemia reduces physical activity, increases absenteeism and decreases school performance [3]. In sub-Saharan Africa, the major causes of anemia include micronutrient deficiencies (particularly iron), infectious diseases (particularly malaria and helminthes) and hemoglobinopathies [4]. The contribution of malaria and hookworm to iron deficiency anemia has been documented extensively [5, 6]. However, little is still known on the association between Schistosoma haematobium infection and iron deficiency anemia. The most recent estimates suggest that approximately 200 million people are affected by schistosomiasis [7]. Of these, 85% live in sub-Saharan Africa where Schistosoma haematobium accounts for 67% of schistosome infections and 70% are school age children [8, 9]. Besides anemia, the disease causes serious consequences, such as impaired physical and mental development, and lower school attendance and performance [10]. In this study, we examined the prevalence of iron deficiency anemia and assessed the effect of iron supplementation on hemoglobin (Hb) and serum ferritin (SF) levels among schoolchildren infected with Schistosoma haematobium in Mali. METHODS Study site and subjects The study, a randomized controlled trial, was conducted in an economically poor neighborhood of Bamako, the capital city of Mali. The study population consisted of primary school children from a single school. Only boys and girls ranging in age from 7-12 years who were anemic (Hb < 120 g/L) and had documented infection with Schistosoma haematobium were eligible. School children in grades 1 to 6 and their parents or guardians were informed about the study and invited to participate. Participants (n = 220) gave their consent, have not been on any oral iron or anthelminthic preparation and have not had a blood transfusion 3 months prior to the study. Of the 220 children screened, 150 who met the inclusion criteria were enrolled in this study. This sample size calculation was based on the primary outcome of Hb concentrations. A two-sided estimation yield a minimum of 130 children (65 per group) needed for analyses. This level of enrolment also allows for an exclusion of 25% non anemic children, a drop-out rate of 10% and an exclusion rate of 5%, expecting that one twentieth of the sample will be excluded and treated for severe anemia. This group size was estimated to be sufficient to detect a 5g/L difference in Hb response among the groups, which is presumed to be clinically significant. These calculations assume an SD of 12 g/L, α = 0.05 and β = 0.20. We enrolled 15% children more in each group to ensure that the sample size at the end of the study remains large enough. Trained health personnel collected venous blood samples (5 mL) for a complete blood count (including hemoglobin) as the first step of enrollment assessment. Mildly or moderately anemic children, as determined from the complete blood count and hemoglobin level, were requested to provide clean voided urine samples in leak resistant and sterile tubes with screw on lids for schistosomiasis determination. Children diagnosed with schistosomiasis were asked to provide additional blood (5 mL) for serum ferritin (SF) measurements. Schistosomiasis infection was diagnosed at baseline by the presence of schistosome eggs in a single sample of urine. Urine samples were shaken well to ensure the adequate dispersal of eggs and 10 mL were processed by the nuclepore filtration technique [11]. Schistosomeeggs were detected microscopically after adding Lugol’s solution. Venous blood was collected at baseline, and at 6 and 12 weeks of the intervention. Aliquots were placed in trace elementfree and K3EDTA vacutainer tubes(Becton Dickinson, Franklin Lakes, New Jersey, USA) chilled and taken immediately to the laboratory for processing. Serum was collected after centrifugation (1800 x g, 10 min at room temperature). Hemoglobin concentration determinations were included in complete blood counts obtained from a Diana-5 hematology analyzer (Hycel diagnostics, Massy, France). Serum ferritin determinations were done in duplicate and analyzed by an automated enzyme linked fluorescent assay using the VIDAS system (BioMérieux, Marcy l’Étoile, France). SF values less than 12 µg/L were interpreted as consistent with iron deficiency. All measurements were made in the same laboratory. The instruments used were calibrated every day. Coefficients of variation of all assays were < 10%. In addition the laboratory personnel who assessed the hematological and biochemical outcomes were not aware of treatment group assignments. Iron deficiency anemia was defined as low Hb concentration (< 120 g/L) + low SF concentration (< 12 µg/L). Two severely anemic children (Hb < 70 g/L) were omitted and referred to a health clinic for evaluation and treatment. Selected children were then assigned randomly to one of two treatment groups: praziquantel alone (P group) or praziquantel + iron (P+Fe group). Praziquantel (40 mg/kg) was administered at enrollment and 4 weeks thereafter. This dosing schedule was expected to avoid re- and persistent Schistosoma haematobium infection. Fe was administered once a day 5 times a week during school days under surveillance by the principal investigator and other field team members. Supplementation was initiated at enrollment and continued for 12 weeks (60 days of supplementation).Supplemental ferrous sulfate tablets (Eupharma Laboratories Limited, India) contained 60 mg of elemental iron. Ethical considerations Recently numerous debates regarding the ethical nature of research in the developing world have centered on issues of exploitation, informed consent and beneficence/non-maleficience. This study took these ethical issues into consideration at every step of the planning process, implementation, analyses and dissemination phases. The research protocol was approved by the Ethics Committee of the Malian National Institute of Public Health Research of the Ministry of Health, the neighborhood school system authorities in Bamako, and by the University Committee on Human Subjects at Cornell University. The purpose and details of the study and its voluntary nature were explained carefully to school children and to their parents and teachers in an appropriate and understandable dialect. Signed assents and consents were obtained from children and their parents before screening and enrollment. Participants were allowed to terminate their participation at any time with no prejudice to them. They were informed individually about results of tests done on them and the meaning of all results. Confidentiality was assured at every step. All information that potentially could lead to identification of individual subjects was excluded from reports. Information regarding children’s participation in the study was not shared with any other individual, except parents, without each child’s consent. Statistical analysis All statistical analyses were done using SPSS version 13.0 for Windows (SPPS Inc., Chicago, Illinois, USA) and STATA version 9 (StataCorp, College Station, Texas, USA) statistical packages. Statistical significance of differences in treatment effects, that is changes in mean hemoglobin and serum ferritin levels between diverse treatment groups at 6 and 12 weeks were assessed by Student’s two-tailed t tests. Chi-square test was used to assess differences in categorical outcomes. Data for SF were log transformed to account for positive skewness in the distribution. P values of 0.05 or less were judged to reflect statistical significance. RESULTS Characteristics of children Children’s mean age was 8.61 ± 1.53 years; there were slightly more boys than girls (52% male). Mean age and sex distributions were not different between the 2 groups. The study profile is shown in fig. 1. Prevalence of anemia At baseline all children were anemic as this was an inclusion criterion. After 6 weeks of the trial, the prevalence of anemia in both groups dropped to 70%, a reduction of 30 percentage points. After 12 weeks, 76% of the children in both groups were still anemic, a reduction of 24 percentage points compared to baseline but an increase of 6 percentage points compared to week 6. The reduction in prevalence of anemia was significantly higher (P < 0.05) in the Fe treated group (30%) than in the P only group (18%) at 12 weeks of the trial. Mean hemoglobin At baseline, there was no difference in mean Hb concentrations between the two treatment groups (Table 1). Following treatments, mean Hb concentrations increased in both groups. After 6 weeks, mean Hb of children who received iron in addition to praziquantel was significantly higher than the mean Hb of children who were treated with praziquantel only (t test = -3.07, p = 0.003). After 12 weeks, the same trend was observed; the group treated with iron had significantly higher mean Hb (t test = -5.50, p = 0.000). Table 1: Mean hemoglobin concentrations before and during the trial1
P,
praziquantel; Fe, iron; Hb, hemoglobin. Prevalence of iron deficiency anemia At baseline, iron deficiency (SF < 12 µg/l) was diagnosed in 17.2% of children. At 12 weeks of the trial, iron deficiency prevalence (children who had an SF less than 12 µg/l) decreased in both groups to 3.5% (60% reduction in the P only group and 72% reduction in the P + Fe group). The comparison between the two groups showed a significantly (p < 0.05) higher reduction in the Fe treated group than in the P group both at 6 and 12 weeks. Mean serum ferritin At baseline, there was no difference in mean SF concentrations between the two treatment groups (Table 2). Following treatments mean SF concentrations increased in both groups. After 6 weeks, mean SF of children who received iron in addition to praziquantel was significantly higher than the mean SF of children who were treated with praziquantel only (t test = -5.16, p = 0.000). After 12 weeks, the same trend was observed; the group treated with iron had significantly higher mean SF (t test = -7.78, p = 0.000). Table 2: Mean serum ferritin concentrations in before and during the trial1
P, praziquantel; Fe, iron; SF, serum ferritin. DISCUSSION In this study the prevalence of iron deficiency anemia and the effect of iron supplementation were assessed among school children infected with Schistosoma haematobium. At baseline more than 15% of anemic children had low iron stores (SF < 12 µg/l). At 6 and 12 weeks of the trial, P and P + Fe treatments increased SF and Hb. Children who received iron in addition to praziquantel had significantly higher means of Hb and SF concentrations than those treated with praziquantel only throughout the study period. The positive effects of P on Hb and SF suggest that the treatment may have reversed a likely sequestration of Fe and limitations of its absorption associated with urinary schistosomiasis by suppressing possible inflammatory processes and by reducing pro-inflammatory cytokines linked to low Hb and SF levels. Similarly, P + Fe treatment may have redressed simultaneously potential inadequate dietary iron and the adverse effects of schistosomiasis infection on erythropoiesis. The relationship between Schistosoma haematobium and anemia has been documented extensively [12, 13, 14]. However, many of the studies have treated concurrently schistosomiasis and geohelminth infections making it difficult to determine the exact benefit of treatment for schistosomiasis. Most of those studies used antischistosomal drugs other than praziquantel. The only randomized controlled study comparing praziquantel to placebo was conducted by Stephenson et al. in a Schistosoma haematobium endemic area of Kenya [12]. In that trial, Schistosoma haematobium was found to be a significant predictor of anemia at baseline, but praziquantel had no significant effect on hemoglobin. A similar conclusion was reached by Befidi-Mengue et al. studying school children in Cameroon [13]. Those authors provided only a single dose of praziquantel and re-assessed hemoglobin after 6 months, a period long enough for re-infections to occur or for other factors (better nutrition, malaria, food shortage or other infections) to ameliorate or reverse effects of the previous treatment. Conflicting results were reported by others. For example, in a randomized controlled trial in which subjects were allocated to placebo, placebo plus praziquantel, placebo plus albendazole, and praziquantel plus albendazole; investigators found that the praziquantel group demonstrated a statistically significant increase in hemoglobin as compared with a placebo group [15, 16]. The results of this study are consistent with this body of literature reporting that treatment of Schistosoma haematobium infection improves hemoglobin levels. Few authors have estimated the losses of blood or iron through urine that occur during Schistosoma haematobium infection. Gerritsen et al. [17] estimated that between 1.3 and 6.1 ml of blood are lost daily as a consequence of this infection. Farid et al. [18] estimated that these daily iron losses are between 0.6 to 37.3 mg. This study’s results are compatible with P treatment reducing blood and iron losses. The results are also compatible with P treatment suppressing proinflamatory cytokine response, which would improve iron absorption as a consequence of expected reductions in pro-inflammatory cytokines enabled by the elimination of the Schistosoma haematobium infection and the prevention of re-infection within the study’s follow-up period [19]. Praziquantel alone had a lower effect on anemia and iron deficiency than P + Fe. However, P + Fe treatment was not enough to reverse anemia in the whole sample. This suggests strongly that other causes such as hemoglobinopathies, malaria and other single or multiple micronutrient deficiencies, likely contribute to anemia in this population. Previous studies have shown, indeed, that malaria and hemoglobinopathies are prevalent among school children in the neighborhood where the study was conducted and that the diets of many Malian families are characterized by low animal food consumption [20, 21]. Therefore, addressing anemia effectively in this population would require an integrated approach in which nutrition, hygiene and health services are provided together. The data presented here are in line with the WHO recommendation to use praziquantel at least once a year in school children living in endemic areas of schistosomiasis [22]. However, greater effect on hematologic status of infected or at risk individuals may require more frequent administration of the drug. For example, the administration of praziquantel twice within a few weeks was shown to offer more advantages over the single-dose treatment in terms of reduction in infection intensity and micro-haematuria, which in turn may reduce the incidence of anemia and iron deficiency [23, 24]. This is especially true and important in areas of high parasite endemicity such as Mali where high risks of new or quick re-infection are persistent. The major limitation of this study is the lack of a control group; that is a group non-infected with Schistosoma haematobium which could have been used to quantify the contribution of the infection to anemia and iron deficiency. Therefore, a study designed to address specifically the question of how Schistosoma haematobium contributes to iron deficiency anemia in similar or other population groups and settings is strongly warranted. CONCLUSION Iron deficiency was highly prevalent among Malian school children infected with Schistosoma haematobium. Treatments with praziquantel alone or in combination with iron supplementation were able to increase hemoglobin and serum ferritin concentrations of those children. The effect of iron added to praziquantel on hemoglobin and serum ferritin, although insufficient to reverse anemia and restore iron stores in the total sample, was significantly higher than the effect of praziquantel treatment alone at both 6 and 12 weeks of the intervention. Consequently, deworming programmes against urinary schistosomiasis for school children in Mali should also integrate other anemia control measures as per the country’s epidemiological profile. REFERENCES
© Copyright 2009 - Rural Outreach Program The following images related to this document are available:Photo images[nd09108f1.jpg] | ||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}