 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food Agriculture Nutrition and Development, Vol. 10, No. 1, Feb, 2010, pp. 2024-2039 Growth performance and iron status of rural beninese school-age children in post- and pre-harvest season Mitchikpe CES*1,2, Dossa RAM1, Ategbo EAD2, van Raaij JMA3 and FJ Kok3 * Corresponding
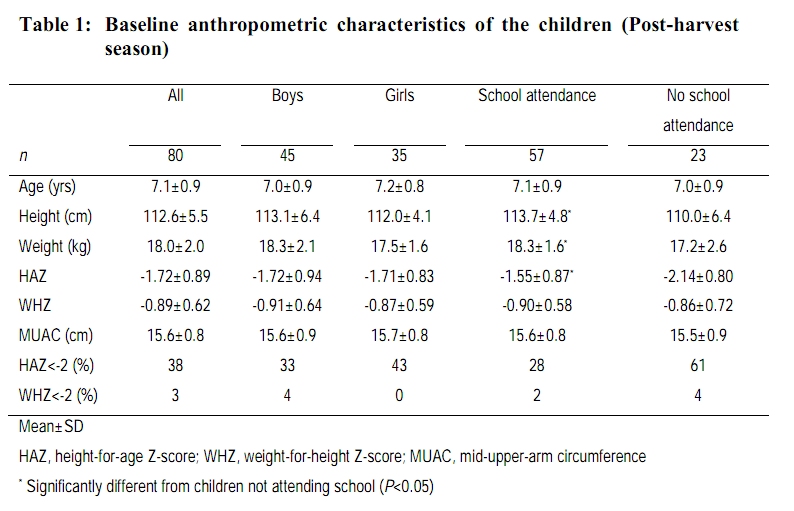
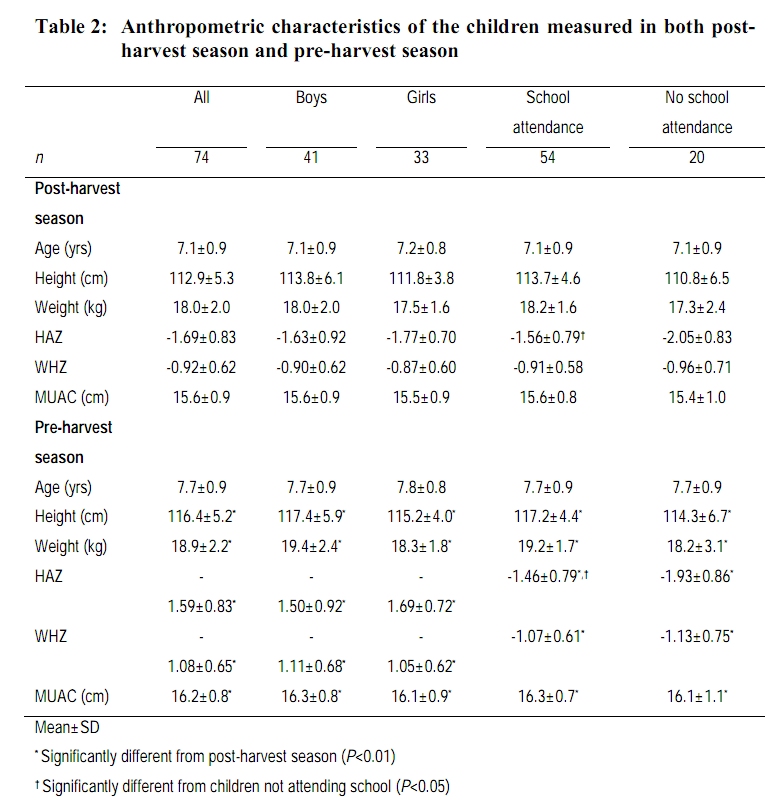
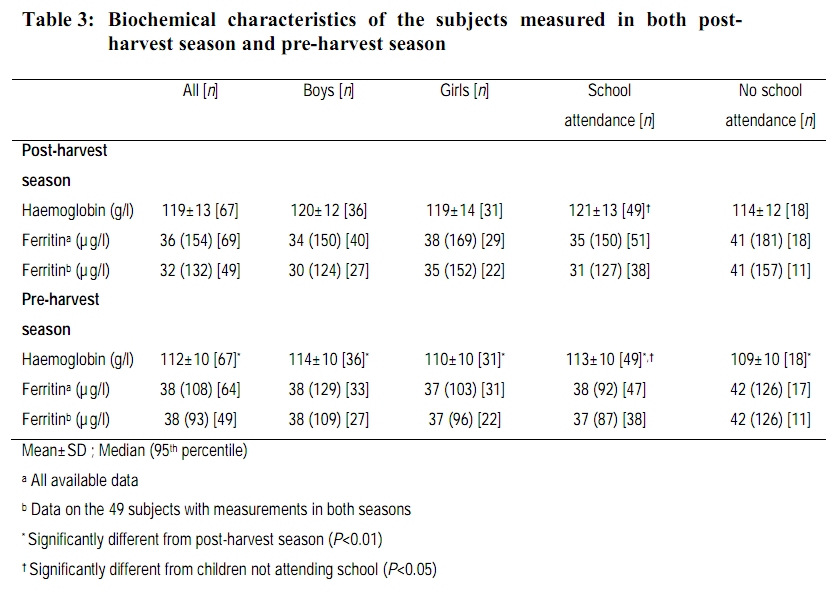
author email: evamitchs@yahoo.fr Code Number: nd10007 ABSTRACT Malnutrition and micronutrient deficiencies are major public health problems in developing countries. Most affected groups are children, adolescents, women of reproductive age and pregnant women. School-age children also represent an important vulnerable age category because they are still in the middle of their growth process which implies that their diets should supply appropriate macro- and micronutrients for an adequate growth and development. A better nutrition in school-age children is associated with increased school performances and a better school achievement. School-age children are dependent on their parents for access to adequate foods and nutrition but, in areas characterised by a unimodal climate with only one rainy season and one dry season, seasonal variation in food availability may also influence their nutritional status. The present study was undertaken to analyse the growth performance and iron status of school-age children in rural Benin, not only in relation to season but also to school attendance. The study was carried out in three villages in the Atacora province in northern Benin. Eighty children aged 6 to 8 years were randomly selected. Anthropometric parameters, haemoglobin level, serum ferritin and C-reactive protein were measured in the same children in the post-harvest season and the next pre-harvest season. Complete anthropometric data sets were available for 74 children while for blood analysis 69 children completed the study. In the post-harvest season, mean Z-scores for height-for-age and for weight-for-height were -1.72 ± 0.89 and -0.89 ± 0.62, respectively. The Z-score for height-for-age of children attending school (-1.55 ± 0.87) was significantly different from that of children not attending school (-2.14 ± 0.80) (P<0.05). In the post-harvest season, haemoglobin level was 119 ± 13 g/l and median serum ferritin level was 36µg/l. The haemoglobin level of children attending school (121 ± 13 g/l) was significantly different from that of children not attending school (114 ± 12 g/l) (P<0.05). The school-age children have poor growth performance and poor iron status that did not differ between seasons. The reasons behind the difference in nutritional status in relation to school attendance need further investigation. Key words: Growth, iron status, school-age, seasonality INTRODUCTION Iron and zinc deficiencies are common in populations dependent on cereal-based diets because of the poor bioavailability of these minerals from such diets [1]. Inadequate absorption of dietary iron is one of the explanations for the high prevalence rate of anaemia in developing countries in addition to the anaemia also caused by parasitic diseases such as malaria or hookworm infection [2]. An inadequate absorption may also apply to dietary zinc, as iron and zinc bioavailability is both susceptible to the same potential inhibitors in plant-based foods. The most cited inhibitors of iron and zinc bioavailability are phytate and polyphenols [3, 4]. Iron deficiency is the result of long-term negative iron balance. It is not the only cause of anaemia. However, when anaemia is prevalent in populations, iron deficiency usually is the most common cause [5]. The World Health Organisation estimated that about 40 % of the world population suffers from anaemia. Current estimates in developing countries suggest that 53 % of school children and 42 % of preschool children are anaemic [2]. Previous studies in Benin suggest a prevalence of more than 70 % among children of 6 to 59 months [6]. In Benin, no such information is available on school children. Growth retardation or stunting in children in developing countries occurs primarily as a result of chronic under-nutrition and infectious diseases and affects 30 % of children under five years of age [7]. A previous study performed in northern Benin reported prevalence of stunting of 28 – 36 % among children under five [8]. In that area, diets were predominantly plant-based and consumption of animal foods was fairly small. Such conditions are probably associated with a high prevalence of iron deficiency and also deficiency of other micronutrients such as zinc and vitamin A. In addition, a seasonal pattern in growth performance of the children was reported [8]. This was probably mainly due to seasonal variation in food availability [9, 10]. Comparable information for school-age children in Benin is scarce. Most nutritional status studies on school-age children focused on children attending school and only few concentrated on children not attending school. In sub-Saharan Africa, this latter category represents as much as 35-40 % of the whole age group [11]. In rural areas of Benin, the proportion of children 6 to 11 years not attending school can reach 52 %. Therefore, the objective of the present study was to analyse the growth performance and the iron status of school-age children in rural Benin, not only in relation to season but also in relation to school attendance. SUBJECTS AND METHODS Study area The study was carried out in three villages in the Atacora province in northern Benin [Figure 1]. This province is characterised by a unimodal climate pattern with the rain season lasting from May to October and one dry season lasting from November to April. Average annual rainfall is about 1300 mm. It is savannah open grassland. The population density is low (21 inhabitants/km²) and the main economic activity is farming. Cultivated food crops are maize, sorghum, millet, yam, cassava, bambara nuts, peanuts and beans. Early crops such as yam, sweet potato, and early varieties of beans, maize and millet are harvested two to three months before the staple cereals are harvested in November and December [9]. Cash crops like cotton, tobacco and cashew nuts are also cultivated. Small livestock and poultry are raised in some households but animals are slaughtered when there is a ceremony or sold when there is an urgent need for money. Clean water sources are limited and a lot of households are still using water from rivers and ditches for drinking and cooking. There is no latrine and domestic wastes are disposed around the house. Study design The nutritional status of 6-8 year olds was assessed by anthropometry and blood analysis during November and December, at the end of the harvest season and six months later in June and July, at the end of the pre-harvest season. Two anthropometric measurement sessions with a time interval of five weeks were organised in each season. Blood samples were collected at the second anthropometric session and were analysed for haemoglobin, serum ferritin and C-reactive protein (CRP). The anthropometric sessions and the blood sampling took place at a hospital annex in one of the villages. Subjects The objectives and contents of this study were discussed with the staff of the hospital of the department in Natitingou, prior to data collection. From the local register of birth, a list with names of 302 children between the ages of 6 to 8 years was obtained. Out of the 302 children, 143 could be traced and served as the sampling population. Only 143 children could be traced mainly because of complicated naming practices and changing of names. Eighty children were randomly selected and this random selection resulted in a sample of 45 boys and 35 girls. This random selection resulted also in a sample of 57 children attending primary school (35 boys and 22 girls) and 23 children not attending primary school (10 boys and 13 girls). Informed consent was obtained from the parents of the children. Complete anthropometric data set became available for 74 children while for blood analysis 69 children completed the study. The slightly lower numbers were caused by moving to other places and by refusing follow-up blood sampling. The baseline anthropometric characteristics including prevalence rate of stunting and wasting of the randomly selected subjects are presented in Table 1. Anthropometric results are based on the mean values from the two measurement sessions in the post-harvest season. METHODOLOGY Anthropometry Anthropometric measurements were performed according to standard procedures [12]. Body weight was measured early in the morning using a SECA platform spring weighing scale (Seca, type 725; Vogel und Halke Mess-Und-Wiege Techniek, Hamburg, Germany). The scale was placed on a horizontal surface and calibrated before each measurement session using a standard weight of 20 kg. Children were measured wearing a minimum of clothing. Readings were done to the nearest 0.5 kg. Height was measured using a microtoise. Measurement was performed with the subject standing without shoes on a horizontal surface against a wall with heels together, chin tucked in and body stretched upwards to full extent and head in the Frankfurt plane. Heels, buttocks and shoulders were in contact with the wall to which the microtoise was attached. Height was read to the nearest 0.1 cm. Mid-upper arm circumference (MUAC) was measured using a flexible non-extensible tape on the left side of the body halfway between the tip of the shoulder and the elbow with the subject's arm hanging freely along the body. Readings were done to the nearest 0.1 cm. Age, height and weight were used to derive anthropometric indexes height-for-age and weight-for-height. Z-scores for height-for-age (HAZ-score) and weight-for-height (WHZ-score) were calculated using the National Centre for Health Statistics (NCHS) reference data and Epi info software (version 2002). Blood sample collection and handling Fasting venous blood samples were collected by medically qualified technicians. Subjects were sitting stretching the arm in a straight line from the shoulder to the wrist and were asked to make a fist. The puncture site was cleaned with antiseptic and an elastic band was placed around the upper arm. A stainless steel needle was inserted within one minute after applying tourniquet and about 10 ml of blood was collected in the evacuated tube. During the procedure, the tourniquet was released to restore circulation. Haemoglobin concentration was determined immediately after sample collection. The remainder of the blood sample was let to clot for 30 minutes at room temperature while tubes were covered with foil. The clotted blood samples were packed in an isotherm container with ice and transferred to the departmental hospital in Natitingou at about 30 km from the hospital annex. Subsequently the samples were centrifuged the same day at 1200 rpm for 15 minutes. Serum was transferred to freezer-proof labelled tubes of 1.5 ml, closed firmly and frozen at -20 °C until analyses. Blood analysesBlood analyses included haemoglobin, serum ferritin and C-reactive protein (CRP) determinations. Haemoglobin concentration (g/l) was determined from whole blood just after collection using a photometry analysis method: the HemoCue device [13]. The accuracy of the HemoCue was checked every day with a control cuvette provided by the manufacturer. Serum ferritin and CRP were determined using kits provided by Randox Laboratories Ltd. Serum ferritin was measured by immunoturbidimetric assay using FN 2464 kit. C-reactive protein was also measured by immunoturbidimetric assay using CRP – CP 7950 kit. These serum analyses were performed in the laboratory of biochemistry of the national university hospital in Cotonou using the automatic biochem-analyser RAXT TECHNICON. To define iron deficiency, serum ferritin < 12 µg/l is generally accepted in absence of infection. Serum ferritin < 30 µg/l is suggested in populations in which prevalence of infection or inflammation is high [5, 14, 15]. Therefore, in the current study, serum ferritin < 30 µg/l is used to define iron deficiency. Iron deficiency anaemia (IDA) is defined as iron deficiency simultaneously with anaemia. This latter is defined as haemoglobin concentration below 115 g/L [16]. C-reactive protein > 10 mg/l is used to indicate presence of infection or inflammatory conditions. Statistical analysesBefore statistical analysis, data were checked for validity. Anthropometric data of the two measurement sessions in each harvest season were averaged after verification by paired t-test of no session difference. Effects of gender, school attendance and seasonality on anthropometric and blood parameters measured at baseline and six months later were studied using factorial ANOVA. Data sets obtained in the post- and pre-harvest seasons were compared using paired-samples t-test or Wilcoxon signed-rank test. Subgroups of children, based on gender and school attendance (attending or not attending school), were also compared using independent samples t-test or Mann-Whitney test. All statistical tests were two tailed and p values less than 0.05 were considered statistically significant. Analyses were performed using SPSS statistical package for Windows (version 11.0). RESULTS The anthropometric results of the children in the post- and pre-harvest season are summarised in Table 2. Height, weight and MUAC in the pre-harvest season were significantly higher than in the post-harvest season (P<0.01). The pre-harvest Z-score for height-for-age was significantly higher than the post-harvest score (P<0.01) and the pre-harvest Z-score for weight-for-height was significantly lower than the post-harvest score (P<0.05). For the total group, prevalence of stunting was high in both seasons (34 % in post-harvest and 27 % in pre-harvest season), but prevalence of wasting was quite low (three percent in post-harvest and seven percent in pre-harvest season). The height-for-age and weight-for-height Z-scores of boys were not significantly different from those obtained on girls. The height-for-age Z-score of school attending children was significantly higher than that of children not attending school, in post-harvest as well as in pre-harvest season (P<0.05). The nutritional status of the children was also assessed by biochemical parameters (Table 3). The pre-harvest haemoglobin level was significantly lower than the level measured in the post-harvest season (P<0.01). Using the cut-off point of 115 g/l, prevalence of anaemia has doubled from 33 % in post-harvest season to 70 % in pre-harvest season. For both seasons, haemoglobin level of school attending children was significantly higher than that of children not attending schools (P<0.05). All other comparisons between and within seasons did not reveal significant differences (see Table 3). For the whole group of children, prevalence of iron deficiency defined as ferritin value < 30 µg/l was 49 % and 33 % in the post- and pre-harvest season, respectively. Prevalence of iron deficiency anaemia defined as presence of iron deficiency simultaneously with anaemia was ten percent in the post-harvest season and 16 % in the pre-harvest season. Elevated CRP values were observed in both seasons suggesting an increased level of infection and inflammatory conditions. C-reactive proteinvalues higher than 10 mg/l were observed in 20 % of the children during the post-harvest season and in 30 % of them during the pre-harvest season. DISCUSSION The objective of the present study was to analyse the growth performance and the iron status of school-age children in rural Benin, not only in relation to season but also in relation to school attendance. Growth performance The mean height and weight of the children were 112.6 ± 5.5 cm and 18.0 ± 2.0 kg, respectively (Table 1). In this study, children were clearly stunted (38 %) but not wasted (three percent). Comparable levels of stunting were reported in preschool children and in school-age children in Benin and in Ghana [8, 17]. From post-harvest to pre-harvest season, the HAZ-score was significantly increased whereas the WHZ-score was significantly decreased (Table 2). However, the absolute differences between the post- and pre-harvest seasons for the HAZ- and WHZ-scores were only 0.10 and 0.16 units, respectively. Such small differences are probably not relevant. Similar results were suggested by Wright et al. [18]. The absence of seasonality was consistent for boys and girls and for children attending and not attending school. The high prevalence of stunting in the school-age children suggests a poor nutrition that started in the past. Study of food intake of the school-age children during the post- and pre-harvest seasons did not show seasonal variation in energy and nutrient intakes; however, the nutritional quality of their diet was inadequate [19]. The diet was based on cereals and was not well balanced (inadequate protein and lipid content), showing that intake of limiting amino-acids from cereals and absorption of fat, fat-soluble vitamins and carotenoids might be low. According to a recent study, the prevalence rate of chronic energy deficiency among women of reproductive age is 13.6 % and there is a high prevalence of stunting in children 24 to 59 months (35 - 52 %) [20]. Therefore, the currently observed high prevalence of stunting might be the expression of a cumulative effect of inadequate food and nutrient intake starting at a young age maybe even before birth. Special attention should be given to infant and young child feeding practices and to the nutritional status of women of reproductive age in the study area in order to assess the problems and design interventions to prevent such high prevalence of chronic malnutrition [21]. The poor growth as reported in this study may have a negative impact on the school performance of the children and may result in poor psychological functioning in late adolescence [22, 23]. This implies that urgent actions should be taken in order to reduce the negative impact of the chronic malnutrition on school achievement and the late psychological functioning of the adults. Actions may involve school feeding targeted at the children but at a global level, strategies such as increasing household food and nutrition security, adding of nutrient to foods, increasing bioavailability of minerals and vitamins, reducing nutrient requirements and supplementation should be implemented. As expected for children of 6 to 8 years, there were no significant differences between boys and girls with respect to anthropometric parameters. However, children attending school have significantly higher heights and weights compared to children not attending school. As a consequence, children attending school have a significantly higher HAZ-score than children not attending school. Similar results were reported among school-age children in Ghana and Tanzania [17, 24]. It is generally assumed that differences in nutritional status between children attending school and children not attending school are due to differences in socio-economic background. However, nearly all children not attending school have a sister or a brother attending school. In addition, in the same area, no socio-economic differences between households have been reported [9]. It is conceivable that parents cannot financially allow all their children to attend school, and that the children attending school might be the privileged of their parents’ choice for those already nutritionally better-off. Iron status Haemoglobin level in the post-harvest season is similar or higher than values reported for schoolchildren in other African countries [24, 25, 26]. It is similar to values reported in Thai school children [27]. Serum ferritin level is also comparable to that reported in Thai school children but is slightly lower than the value reported for Kenyan children [26]. From post-harvest to pre-harvest season, haemoglobin level was significantly decreased by 7 g/l. This resulted in an increased prevalence of anaemia from 33 to 70 %. A comparable high prevalence rate of anaemia has been reported for Beninese preschool children [6]. Serum ferritin levels were not significantly different between seasons. The commonly used cut-off value of serum ferritin < 12 µg/l as an indicator of iron status might underestimate the prevalence of iron deficiency if infections or inflammations are present [28]. In such situations, serum ferritin < 30 µg/l is suggested [5, 14, 15]. Using this cut-off point of serum ferritin < 30 µg/l, the prevalence of iron deficiency is estimated to 49 % and 33 % in post- and pre-harvest season, respectively. These high prevalence rates are in line with those obtained in school children in Côte d’Ivoire [15]. The prevalence of iron deficiency anaemia defined as presence of anaemia simultaneously with iron deficiency was ten percent and 16 % in the post- and pre-harvest season, respectively. The high prevalence of iron deficiency in the post- and pre-harvest seasons strongly suggests poor iron nutrition in the children. The diet of the children contains only small amounts of animal products and is low in protein, fat and vitamin C, and high in fiber. Anti-nutritional factors such as phytate and polyphenols in the diet were also high [29]. This means that in addition to the reduced absorption of fats, fat-soluble vitamins and carotenoids, iron and zinc bioavailability might be fairly low. The increased level of anaemia with unchanged iron status from the post-harvest to the pre-harvest season might be explained by the increased prevalence of infections and malaria [30]. The C-reactive protein (CRP) data indeed suggest an increased prevalence of infections in the pre-harvest season (30 %) when compared to the post-harvest season (20 %). The poor hygiene and sanitation as observed in the villages also might explain these high prevalence rates. A similar prevalence rate of infections was reported in school children in Côte d’Ivoire [15]. Determinants of iron status of the school-age children are in line with determinants of their growth performance as measured by anthropometry. A global approach for improving the nutritional quality of the diet and reducing nutrient requirements (by improving sanitation, controlling malaria, vaccination, controlling birth and deworming) might provide a sustainable solution for the nutrition problem in the study area. As expected for children of 6 to 8 years, there was no difference between boys and girls with respect to haemoglobin and serum ferritin levels. However, children attending school have significantly higher haemoglobin levels compared to children not attending school. Similar findings were reported by Fentiman et al. [17]. The difference in haemoglobin levels between children attending and not attending school might be due to the interaction between nutritional status and morbidity as children not attending school have a significantly lower HAZ-score than children attending school. In conclusion, school-age children in northern Benin have a poor growth performance that did not differ between seasons. Iron status should also be considered as poor, and also did not differ between seasons. Prevalence rate of anaemia was high but significantly higher in pre-harvest season probably because of infections. Reasons behind the difference in nutritional status of children attending school and those not attending school need to be further explored. Inadequate dietary intakes on a long-term, and poor hygiene and sanitation to a lesser extent might be the major determinants of the nutritional status of school-age children in northern Benin. Government, non-governmental organizations and private sectors should work together in order to increase school attendance, and nutrition and health of children in northern Benin. For further actions, infants and young children feeding practices and the nutritional status of women of reproductive age need to be documented. ACKNOWLEDGEMENT This study was financially supported by the North-South Interdisciplinary Research and Education Fund (INREF) of Wageningen University. REFERENCES
Copyright © 2010 - Rural Outreach Program The following images related to this document are available:Photo images[nd10007t3.jpg] [nd10007t2.jpg] [nd10007f1.jpg] [nd10007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}