 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food, Agriculture, Nutrition and Development, Vol. 10, No. 7, 2010, pp. 2804-2817 Article DIETARY PATTERNS OF INFANT AND PRESCHOOL CHILDREN IN MWINGI AND MAKUENI DISTRICTS OF UKAMBANI REGION, EASTERN KENYA Ndiku M*1, 2 , Jaceldo-Siegl K1 and J Sabaté 2,3 1Department of Family and Consumer Sciences School of Science and Technology
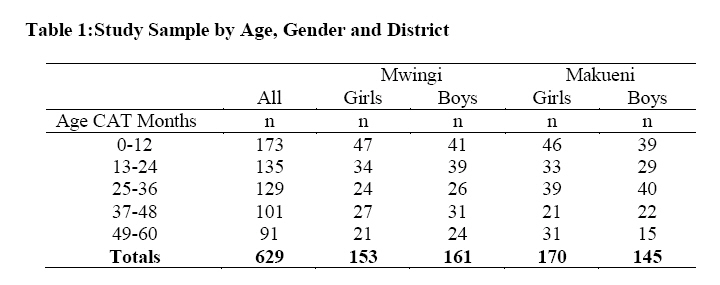
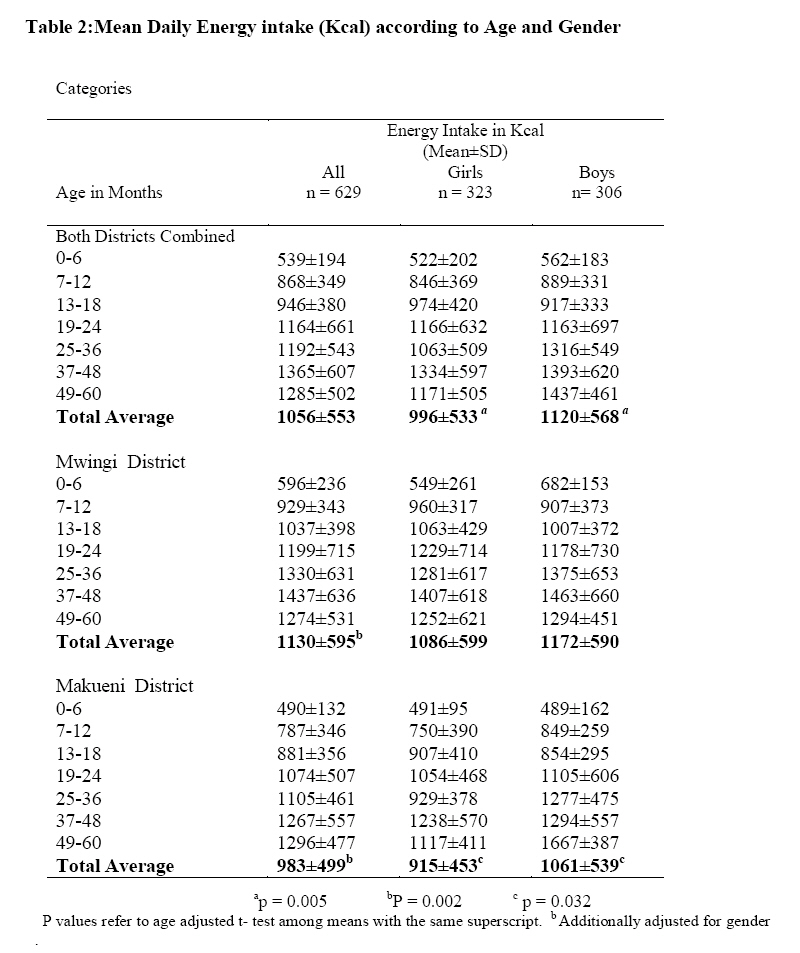
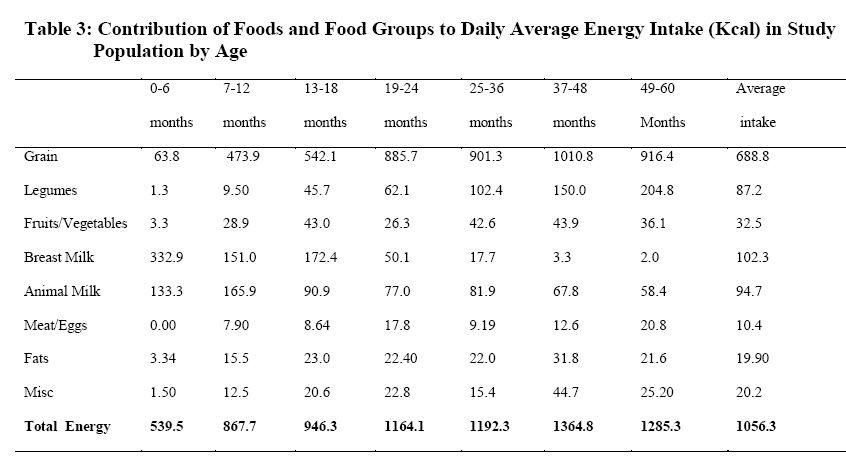
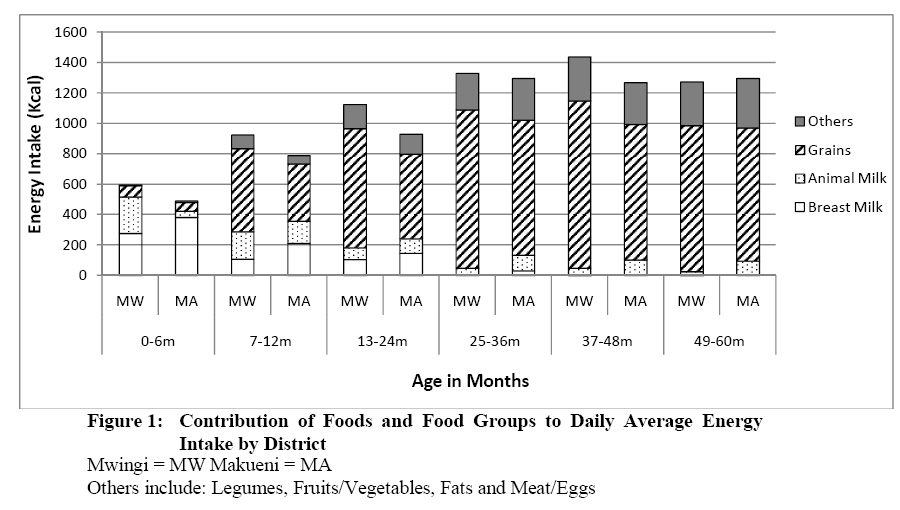
University of Eastern Africa, Baraton. P.O Box 2500 Eldoret, Kenya *Corresponding author email: hellenndiku@yahoo.com Code Number: nd10069 ABSTRACT A cross -sectional study was conducted in the Ukambani region of Eastern Kenya to describe dietary patterns of infants and preschool children. The purpose of the study was to provide region specific data on dietary patterns of children living in Mwingi (MW) a region that mainly grows pearl millet and Makueni (MA), a region that grows maize. A modified rapid, knowledge, practice and coverage (KPC) questionnaire and a 24-hr dietary recall were used to collect the data. A total of 403 households (201 – MW, 202 – MA) were surveyed from four randomly selected divisions of MW and MA districts. This yielded 629 surrogate 24-hr dietary recalls with 314 children from MW district and 315 children from MA district (49% boys and 51% girls). Intake of nutrients and food groups were compared between the two districts using t- test. On average, grains contributed 62-68 percent of total energy intake in both districts. Mean daily energy intake (mean ±SD) for all the children was 1056 ± 553 Kcal. Daily energy intake (1130 ± 595 Kcal) in MW children was 15% higher compared to MA children (983 ± 499 Kcal, p = 0.002). Boys had a 12% higher daily energy intake than girls (p = 0.005). The contribution to total energy from grains was 27% higher in MW children (p = 0.0001) and breast milk contribution to total energy intake was 50% less in MW children (p < 0.001). Consumption of fruits and vegetables was significantly lower in MW children (p<0.0001). Intakes of carbohydrate, protein and iron were higher in MW children and vitamin A intake was lower. Fat intake was the same in both districts for these children. Gender and geographical differences were observed in diets of children in Ukambani region, with the most prominent being the type and amount of cereal intake. Key words: Ukambani, Kenya, under-fives, diets, millet INTRODUCTION Chronic under-nutrition in developing countries continues to be a major cause of morbidity and mortality among children, the most vulnerable segment of the population. One major cause is difficulties in food availability in most developing nations [1, 2]. Assessing food consumption patterns in different areas in developing nations can be helpful in identifying these locations; documenting the type and severity of the food unavailability; describing the causes of malnutrition and understanding practices that might contribute to food unavailability [1]. Dietary assessment surveys can also provide valuable data to guide in policy making, planning at national and regional levels, prioritizing, designing, and evaluation of programs [1]. Although many studies have been undertaken on the nutritional status of infant and preschool children in Kenya, few have described their dietary habits [3-6]. There is a paucity of data on studies describing dietary habits of these children, especially at regional levels. This report describes the dietary patterns of infant and preschool children in two districts in the Ukambani region in Kenya. Mwingi district uses a traditional cereal, pearl millet, as its staple cereal, while Makueni uses maize. This research hypothesized that cultivation and consumption of the traditional grain, pearl millet, in addition to maize, results in improved food availability and better nourishment for children. However, the study did not control for other variables which may differ between the two regions, in particular household income. METHODOLODY AND DESIGN Study area and population This was a descriptive study of the diets of infants and preschool children living in rural districts of Mwingi and Makueni in the Ukambani region. The study population was predominantly of the Akamba ethnic group who live in the semi-arid Eastern province of Kenya [7]. Out of the four districts in Ukambani region, two were selected, which represented maize or pearl millet. Four divisions were then randomly selected, and within the divisions, a total of sixteen villages were selected. These villages were classified as remote, or more remote, based on a 14- item scale assessing a village’s accessibility to the outside world, using infrastructure. All the households in these villages were visited and determined to be eligible for data collection. All households with infants and preschool children were included. Households whose mothers were not present at the homestead at the time of data collection were excluded, since data were only collected from the biological mother of the children. Data were collected from 403 households: 201 and 202 mothers from Mwingi and Makueni, respectively. This represented 629 children with 314 from Mwingi and 315 from Makueni districts. Data collection procedure The research team consisted of a leader (M.N) and four trained research assistants. Data collection proceeded after permission was granted from the district commissioner’s office. At the village level, the team was led by a village elder from house to house during the home visitations. Data were collected in two phases: January to March 2008 (the rainy season), and June to September 2008 (dry/harvest season), from the four randomly selected locations in Mwingi and Makueni. The data collection instruments included a mother and child section that was a modified rapid, knowledge, practice and coverage (KPC) survey questionnaire, and a 24-hr dietary recall of the mother on the child’s food intake. A consent statement was read verbally to the parents in Kikamba (vernacular) and a verbal informed consent was obtained from the biological mother before proceeding with the dietary assessment interview. The age for the children was recorded as reported by the mother, and then verified with the maternal and child health (MCH) cards. Where there was discrepancy, the age on the MCH card prevailed. The 24-hr diet recall data Dietary intake of each child was assessed by a face to face 24- hr dietary recall interview from the mother. A 24-hr dietary record form was used to collect the dietary recalls. The form had a name, location, sub-location and village sections to be completed. An accurate and comprehensive listing of all food/drink the children consumed within the last 24 hours was recorded. A record of how much food was consumed and at what time, was also taken. Preparation methods and how the food was served were recorded as well. Children who were exclusively breastfed and were ≤ 6 months were estimated to take an average of 25 fluid oz (750ml) of breast milk per day. From the 24-hr dietary recall records it was averaged that the babies were fed 6 times per day. Therefore, using this estimate of 6 times within 24 hours, an average of ½ cup of breast milk was estimated for every breast feeding in the 24-hr recall record [8, 9]. After introduction of solid foods, the milk was adjusted accordingly to accommodate the use of solid foods as suggested in the Kenya demographic survey [6]. Thus, as indicated already, the study was done in two phases. During the first phase of the study, the 24-hr diet recalls were done without aid. The mother reported what food, and how much of it, she had fed the child and the researcher estimated the portion sizes. During the second phase, water and a measuring device were used to estimate the portion sizes. The mother was requested to show the interviewers the utensil(s) used to feed the child. The utensil was then filled with water equivalent to the amount of food consumed by the child as shown by the mother. The water was then transferred into a graduated cup and measured for the exact amount. Recipes for foods commonly eaten by the children were created. The mothers provided some of the recipes during the 24-hr diet recall interviews and the rest were generated using one of the author’s (M.N) prior knowledge of having grown and socialized in this region. Porridge recipes were developed and tested with flour imported from Kenya. This was done in the nutrition department kitchen at Loma Linda University in order to obtain exact ratios (by weight) of grain (millet, corn, or sorghum) and water to produce porridge of light, medium, thick or ugali consistency. A random 10% of the 24-hr dietary recall interviews (entries) were selected for quality control. Recipes beyond the range of nutrient tolerance (gram weight >500 and energy >400 per serving) were flagged, checked for accuracy, and then corrected as necessary. Data analysis The 24-hr dietary recall interviews were entered using the NDS-R 2008 (The Nutrition Coordinating Center, Minneapolis, MN, USA). The 24-hr diet recalls were analyzed in terms of nutrients and food groups. For food group analyzes, individual components or ingredients were aggregated into 8 food groups: grain, legumes, fruits/vegetables, breast milk, milk, meat/eggs, fat and miscellaneous. The nutritional data were normalized using log transformations where appropriate, and differences for consumption between age, gender or geographic category were assessed using independent sample t-tests and chi square, with significance assumed at an alpha of 0.05. Descriptive results are reported as mean ±standard deviation (SD), unless otherwise indicated. All statistical analysis was done using SAS version 9.2 (Cary, NC, USA). This research had approval from Kenya Government, Ministry of Higher Education and Loma Linda University Institutional Review Board. RESULTS A total of 629 surrogate 24-hr diet recalls were obtained from 403 mothers. Of the 629 children, 306 (49%) were boys and 323 (51%) were girls. The average age for the interviewed mothers was 30±7 yrs and the mean age for the children was 26.5±17 months. Table 1 presents the distribution of the children by age and gender categories of each district. The distribution was similar, except for the oldest age category of Makueni district where the number of girls was double the boys. There was a progressive decrease of the number of children as age increased in both districts. Table 2 presents mean daily energy intake according to age and gender categories of the two districts. Mean energy intake for these children was 1056±553Kcal. Boys in the two districts had higher total energy intake than girls in almost all age categories and overall. As age increased, daily energy intake for the children increased steadily in both districts except for age category 49-60 months, where there was a major drop. Mwingi children had a 15% higher mean energy intake (1130±595Kcal) than Makueni children (983±499Kcal p = 0.002). Overall, boys had a 12% higher mean energy intake (1120±568 Kcal) than girls (996 ±533 Kcal, p= 0.005). Boys in Makueni had a significantly higher daily energy intake (1061±539) than girls (915±539, p= 0.032). Table 3 presents contribution of food and food groups to daily average intake in the study population. Overall, grains contributed about 62-68 percent of the total energy intake of the children in both districts. Figure 1 shows the contribution of food and food groups to daily average energy intake by district. Grains contribution to daily energy intake was 27% higher (p= 0.0001) in Mwingi children than Makueni children. Breast milk contribution to daily energy intake was 50 % higher in Makueni compared to Mwingi children (p <0.001). Likewise, energy from fruits and vegetables was 178% higher in MA children than MW children (p< 0.0001). The rest of the food groups were not significantly different in both districts. The contribution of breast milk to the daily energy intake of these children tapered off at around 18-24 months in both districts. Mothers of Mwingi district seemed to introduce complementary foods to their children in the first six months. Mothers in Makueni seemed to sustain breastfeeding longer than the mothers in Mwingi. The average total length for breast feeding, as reported by the mothers, was 21.3±8 months for both districts. The same average was 20.4±7.3 months for Mwingi mothers and 22.1±8.6 months for Makueni mothers. (Data not shown). Table 4 presents comparisons of nutrients intake in both districts to recommended daily intake (RDI) in children ≥ 18 months [10]. Children aged 18-36 months had deficits in energy, fat and iron, while those aged 37-60 months had deficits in energy and fat. In the Mwingi district children 18-36 months had higher intakes of carbohydrates (18%), protein (28%) and iron (32%) compared to RDI. Children 37-60 months had higher intakes of energy (6%), protein (6%) and iron (21%), less high, but still above RDI. In Makueni children had higher intakes of vitamin A: 66% for 18-36 months and 24% for 36-60 months. (Data not shown). DISCUSSION This survey found that in infant and preschool children in the Ukambani region of Eastern Kenya, energy consumption increases with age, until the older age category (49-60 months) where there is a major drop; also energy intake in boys is 12 % higher than girls. There are marked differences in breastfeeding practices in the two districts. Mwingi children have higher intake of grains, carbohydrates, protein and iron compared to children from Makueni. The progressive decrease in the numbers of children as age increased resulted in an overall attrition rate of about 42-50%. It is unlikely that the increased mobility of the older children, rendering them unavailable at the time of the research team visit to the households would account for this high attrition rate. The National Kenya Demographic Health Survey (KDHS) for 2003 reports the national under-five mortality rate as 115 deaths per 1,000 live births and infant mortality rate as 77 deaths per 1,000 births. This means that one out of every nine children born in Kenya die before attaining his/her fifth birthday [6]. Daily energy intake consumption increased steadily in all the age categories except for age category 49-60 months where there was a sharp decline. Data were checked for errors, it is unlikely that this was due to computation error, underreporting on the side of the respondent, or due to unstable estimates. The reporting method was the same for all the age categories and the standard deviation for the cell with the smallest sample size was not large. It is probable that these children consumed less energy, or that the children became independent and the mother had no correct record of what they ate. Boys consistently had higher energy intakes than girls. It is likely that the boys were served more than the girls, or mothers over-reported due to expected traditional practices. If it is that the boys were served more, then malnutrition indices (mean Z scores) should be lower in girls and malnutrition prevalence should be higher in girls. This warrants further study. During the first year of life, there is a dramatic drop in breast feeding in the study population. In both districts, breast milk tapered off and ceased to be a major contributor of energy to these children at about 18 months. However, mothers in Makueni district sustained breastfeeding longer than mothers in Mwingi district. Between 18-24 months, most mothers stopped breast feeding completely. This is in support of a study conducted at Kathonzweni in Makueni that reports that most mothers stopped breastfeeding between 12-18 months because they might have conceived [5]. A study in Machakos reports that breast feeding was practiced until 18-24 months [8]. Another study conducted in Western Kenya indicates that breastfeeding was sustained until at least the latter part of the second year for most children in a location in Busia district [11]. In the current study, there is concurrence between the reported length of breastfeeding from the mothers and the actual data collected in the 24-hr recall showing breast milk contribution to daily energy intake. The 2003 KDHS reports at the national level the duration for breastfeeding as 20 months in the rural areas and 19 months in urban areas. At the provincial level, Eastern province had the longest reported breast feeding period, 25 months [6]. Therefore, this study supports the period between 18-24 months as a good cut point for breast feeding in studies looking at nutritional status in infant and preschool children. This is so because breast milk is protective of malnutrition. In both districts, most children were introduced to other foods between the ages of 0-6 months. These other foods, specifically, were milk (cow’s and goat’s milk) and grain porridges of different consistencies. Mwingi district mothers tended to introduce these foods a little earlier than Makueni district mothers. Results from the Kenya Demographic Health Survey indicate that half of all the children between two and three months are given complementary foods [6]. In addition, children under six months receive the following complementary foods: milk other than breast milk (36%), food made from grains (28%), and fruits and vegetables (23%) [6]. In this study population, grains contributed about 62-68% of the total daily energy intake followed by milk (19%) and legumes (8.3%). The higher percentage in grain consumption in Mwingi children could be due to the growing of the traditional grain pearl millet in this district. Pearl millet is indigenous to Ukambani region and was the main staple cereal 50 years ago before the introduction of maize. It is considered more efficient in utilization of soil moisture and has a higher level of heat tolerance than sorghum and maize [12]. Cultivation and consumption of this traditional grain, which has better nutritive value than maize and sorghum, may result in better nourishment of children in arid lands like Ukambani region. The high consumption of cereals by Mwingi district children corresponds to relevant nutrients intake as well. For children ≥ 18 months, Mwingi children had higher intakes of carbohydrates, protein and iron, while Makueni children had higher intakes of vitamin A. Fat intake was the same in both districts. Overall, these children had deficits in energy, fat and iron. Mwingi had no deficit in iron for age category 37-60 months. This could be due to consumption of higher amounts of legumes, which are a good source of iron, as well as pearl millet which is higher in iron than maize, and is comparable to wheat in iron and zinc contents [13]. Children met their recommended daily intake for protein and vitamin A [10]. It is important to note that the protein is mainly derived from grains and legumes. Therefore, it is important for this community to keep a good supply of legumes and grains. The mothers did not report having used many animal products to feed their children during the 24-hr recall. It has been reported that Kenyan children in general have inadequate intakes of energy, fat and micronutrients such as iron, zinc and calcium among many others [14]. A study in Uganda reports energy deficits in children between 12-35 months [15]. Meat and egg consumption was on the low side in this study. The same was observed in a study in Kathonzweni Makueni district [5]. Since most homes had domestic animals, ranging from chicken to cows, parents could be encouraged to incorporate these animal foods in their children’s diet. Animal foods supply high–quality protein and readily digestible protein and energy. They are also a dense and efficient source of readily available micronutrients [16]. CONCLUSION In this population, the boy child consistently seems to consume more energy than the girl child and this may translate into gender differences in malnutrition indices. The major contributor to daily energy in children of this region is grains. In almost all age categories, Mwingi district children have higher energy intakes than Makueni district children. There are marked differences in breastfeeding practices in the two districts in that Makueni mothers seem to sustain breastfeeding longer than Mwingi mothers, while mothers in Mwingi seem to introduce complementary foods earlier in the first six months of children’s life. Further research is needed to establish if the cultivation and consumption of the traditional cereal pearl millet along with the other traditional cereals and maize may result in better nourishment of children in arid lands like Ukambani region. However, a limitation was that this study did not control for other important variables which may have differed in the two regions, particularly household income, ACKNOWLEDGEMENT We wish to thank the Federico Foundation, Switzerland for funding this project and the research team for invaluable assistance during the fieldwork. REFERENCES
Copyright 2010 - African Journal of Food Agriculture, Nutrition and Development The following images related to this document are available:Photo images[nd10069t1.jpg] [nd10069t3.jpg] [nd10069t2.jpg] [nd10069f1.jpg] [nd10069t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}