 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Food, Agriculture, Nutrition and Development, Vol. 11, No. 1, 2011 pp. 4582-4594 DIET AND HYPERTENSION: A COMPARATIVE ANALYSIS OF FOUR DIET GROUPS IN SOUTH-WESTERN NIGERIA Makinde YO*1 and DA Babalola1 1Department of Agriculture and Industrial Technology, Babcock University, Ilishan, Ogun State, Nigeria *Corresponding author email: yetundemakinde@gmail.com Code Number: nd11010 ABSTRACT
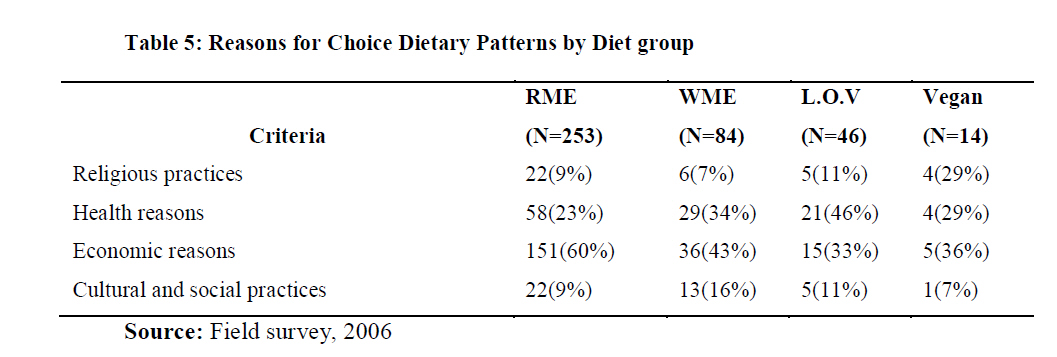
Rising burden of hypertension in sub-Saharan Africa has been well documented. This study examines the relationship between diet pattern, anthropometry and hypertension in south western Nigeria. Three hundred and ninety seven adults (108 men and 289 women), aged 21 years or older formed the sample size used for this study. The respondents were grouped into four diet classes or groups based upon their dietary habits. These dietary habits include red meat eaters (RME), white meat eaters (WME), lacto-ovo-vegetarians (L-O-V) and vegans (V). A lifestyle questionnaire was administered to respondents to collect their socio-economic characteristics (age, gender, marital status, level of education and income level), their reasons for choosing particular dietary habits, their physical activity levels, and blood pressure status awareness. Anthropometric measurements (body mass index, waist circumference, hip circumference, waist- hip ratio and waist- height ratio) and actual blood pressure status (diastolic blood pressure and systolic blood pressure) status were also obtained from each respondent. Diagnosis of hypertension was based on blood pressure of >160/95mmHg. Results showed that the average body mass index (BMI) was highest among the red meat eaters (mean= 25kg/m2) and lowest among the vegans (mean = 21.19kg/m2). There was significant correlation between BMI and blood pressure (BP) levels (diastolic and systolic) in both male and female RME (p<0.01). No significant correlation was observed between the anthropometric measurements and blood pressure in the vegans. The majority of the respondents were not aware of their blood pressure status (RME= 89%, WME= 92%, L-O-V= 85% and V= 93%). However, some of the participants were found to be hypertensive: 13% of males and 9% of females. Based on the reasons given for the choice of dietary habit, economic reasons ranked highest for choice of dietary habit especially among RME (60%). But health and religious reasons were also important factors for dietary pattern among L-O-V and V. Promotion of nutrition education and relevant public health action which focuses on the environmental and nutritional changes was recommended. Key words: Hypertension, Anthropometric measurements, diet, vegetarian INTRODUCTION
There has been a general rise in life expectancy in the past century in both the developing and developed world [1]. This increase has been attributed primarily to improved preventive practices, not to advances in clinical medicine. It has been estimated that the increase in life expectancy has been largely due to disease prevention [1]. The second half of the twentieth century witnessed major health transitions in the world, propelled by socio-economic and technological changes that profoundly altered life expectancy and ways of living, while creating an unprecedented human capacity to use science to prolong and enhance life. The most globally pervasive change among these health transitions has been the rising burden of noncommunicable diseases such as cardiovascular diseases (CVD) [2]. By 2001, CVD became the number one cause of death worldwide with eight per cent of the burden occuring in developing countries. Considering that many developing countries are still contending with infectious diseases and malnutrition problems [3], the emergence of non-communicable diseases [4], and various types of cancer, contributes to an even greater morbidity and mortality [5]. Many studies on the epidemiological transition have shown that over the last two centuries, the industrial and technological revolutions and the economic and social transformations associated with them have resulted in a dramatic shift in the cause of death from infectious diseases and malnutrition before 1900, to non- communicable disease (NCD) such as hypertension and cancer today [3, 4]. A global NCD epidemic is rapidly emerging. Twice as many deaths due to CVD can be attributed to risk factors such as hypertension and obesity. Even in sub-Saharan Africa, high blood pressure, high cholesterol, tobacco and alcohol use, and low vegetable and fruit consumption are already among the top risk factors for cardiovascular disease [4, 5]. The non-communicable disease (NCD) epidemic bears direct implications on the quality and quantity of household labour supply and life expectancy especially in an agrarian economy such as Nigeria. It has been estimated that by 2020, between 55 and 80 percent of the total burden of disease in Asia and many parts of sub-Saharan Africa will be attributable to noncommunicable diseases [2]. Hypertension, the most common treatable risk factor for CVD [6] is responsible for 12.4 million deaths annually, most of which (9.6 million) occur in developing countries [7]. The prevalence of hypertension in Nigeria, the largest black nation on earth, ranges from 8-10% in the rural area to 10-12% in the urban population baseline of 160/95mmHg [4,5]. Three percent of the population dies from hypertension every year and about 7% are at risk [8]. Hypertension is a disease most commonly found among middle-aged and elderly Nigerians [9,10]. Hypertension is said to occur when the blood pressure is above normal (such as when systolic is above 140mmHg and diastolic is above 90mmHg). High blood pressure is an emerging health problem in semi-urban areas in sub-Saharan Africa. Among the several factors found to contribute to this emerging trend, poor diet has been reported to contribute 87%, while environmental and other factors share 13% [4, 11, 12]. Rapid movement to urban areas has led to increased consumption of processed food which has increased the risk of CVDs [4, 13]. Unfortunately, like HIV/AIDS, hypertension is a silent killer and many do not consider themselves at risk from consuming poor diets consisting of food and snacks with high salt, saturated fat content and refined carbohydrate content, as well as cigarette smoking and alcohol consumption. Possible interaction between early childhood nutrition and risk of CVDs later in life has been reported by Barker [14]. Though not conclusively proven, the “Barker hypothesis” raises serious considerations for most developing countries where child malnutrion is entrenched. Obesity, a diet-related risk factor for hypertension, usually defined as BMI of > 30kg/m2 is responsible for substantial morbidity and early mortality [12, 15, 16]. Relationship between obesity and hypertension among black Africans is not completely understood because of paucity of data. Studies have shown differences in BMI and nutrient intakes between meat-eaters and vegetarians [7, 17]. Findings have also severally focused on BMI and other anthropometric variables and socio-economic factors on high blood pressure among Nigerian and other black African populations [7, 18]. There is evidence to demonstrate that many hypertensive individuals in Nigeria are blissfully ignorant of the occurrence of this disease and few are knowledgeable of associated risks or needed therapy to minimize such risks. Even when detected, less than half of victims have access to proper treatment to control the silent killer disease [6]. The south western part of Nigeria records higher incidence of poverty [19]. The poor will become progressively vulnerable to the ravages of CVD risk factors such as high blood pressure, and will have little access to the expensive and technology-intensive management that clinical care demands. Also, the diversion of scarce societal resources to the treatment of these disorders dangerously compromises the ‘unfinished agenda’ of infectious and nutritional disorders that almost exclusively afflict the poor. It is against this backdrop that this paper examines prevalence of hypertension, a major cause of morbidity and mortality, in relation to anthropometric measurements (BMI and upper-body adiposity-WC, WHR, and WHtR) and socio-demographic factors among four selected diet groups in the south western part of Nigeria. METHODOLOGY
The study was carried out in the south western part of Nigeria. Ogun State was chosen based upon proximity to the centre where anthropometric measurements were recorded on all the respondents. Three hundred and ninety seven (397) adults were selected using multi-stage random sampling method. Respondents were sampled from four local government areas from existing 15 local government areas as follows: 100 from Abeokuta North, 100 from Abeokuta south, 99 from Sagamu and 98 from Ikenne. The respondents’ food intake over the previous year was collected using the food frequency questions (FFQ) section of the structured lifestyle questionnaire. The responses to the questions were used to classify the population into 4- four diet groups: red meat eaters (RME), white meat eaters (eat fish and chicken but no red meat) (WME), lacto-ovo-vegetarians (consume, milk products and eggs but no red or white meat) (L-O-V) and vegans (exclude all animal flesh and products) (V). Other variables collected from the respondents include socio-economic characteristics such as age, gender and income level. Anthropometric measurements, reasons for choosing a particular dietary habit, physical activity levels (such as brisk walking, jogging, running, cycling, swimming and dancing), high blood pressure status awareness and actual blood pressure status were obtained. Diagnosis of hypertension was based on blood pressure of >140/90mmHg. Data were coded and subjected to descriptive statistics and correlation using the Statistical Package for Social Sciences (SPSS 11.0; SPSS Inc). RESEARCH FINDINGS Socio- Demographic characteristics
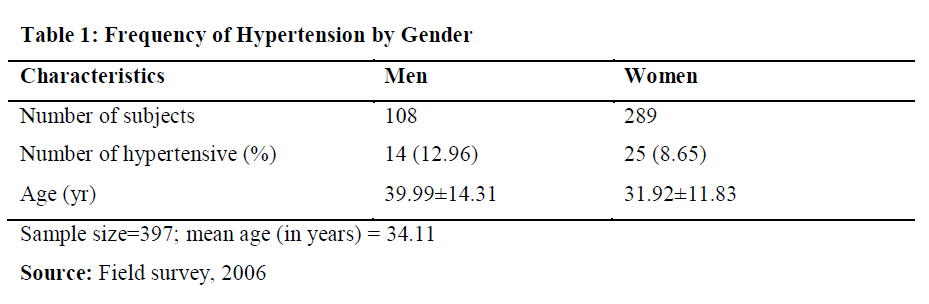
Table 1 shows that more females than males were sampled (108 men and 289 women). The mean age for the sampled respondents was 34 years, 40 years for men and 32 years for women. Results showed that majority of the respondents had at least secondary education (Table 2). Diet
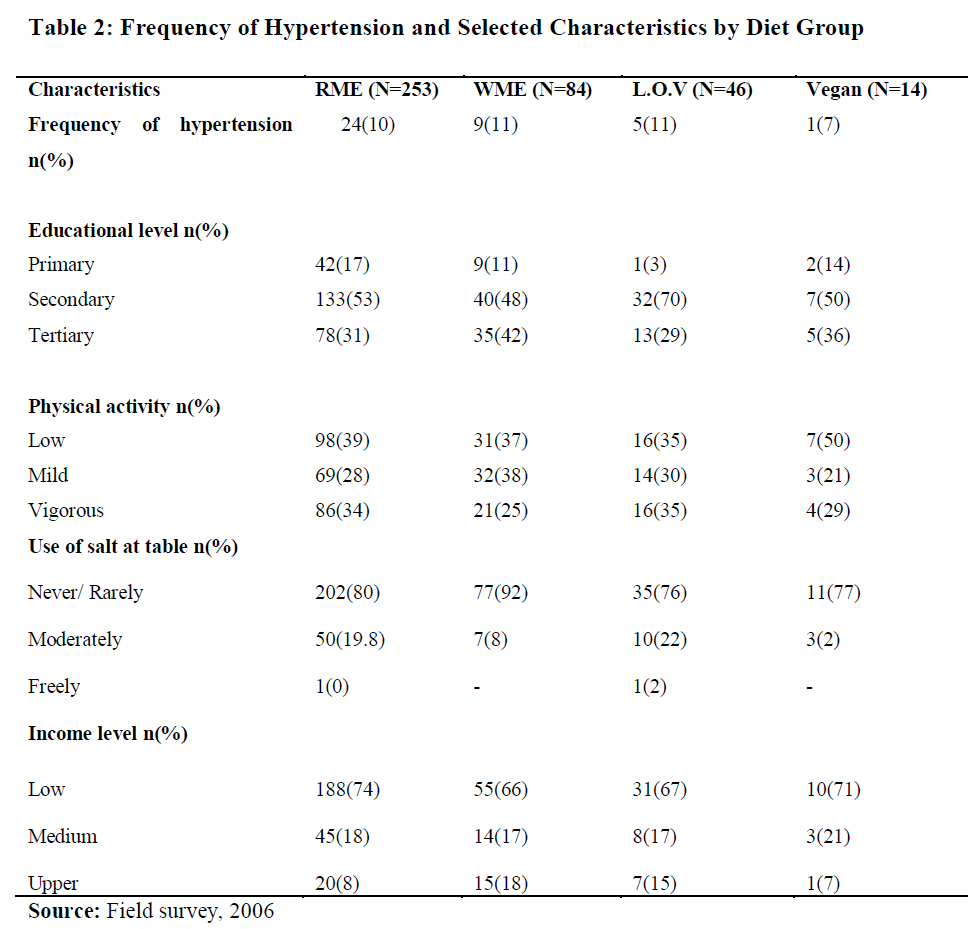
Out of the 397 respondents interviewed, 253 were red meat eaters, 84 were white meat eaters, 46 were lacto- ovo- vegetarians and 14 were vegans (see Table 2). Physical Activity
Table 2 shows that 34% of RME, 25% of WME, 35% of LOV 29% of V engaged in vigorous daily activities. Furthermore, 39% of RME, 37% of WME, 35% of LOV 50% of V engaged in low physical exerting activities daily. Educational Level
Table 2 shows that the majority of the respondents, across the diet groups have secondary education and above (84%, 90%, 98% and 86%) for RME, WME, LOV and V, respectively. Income Level
Low income level is defined as earning less than Blood Pressure and Anthropometric measurements
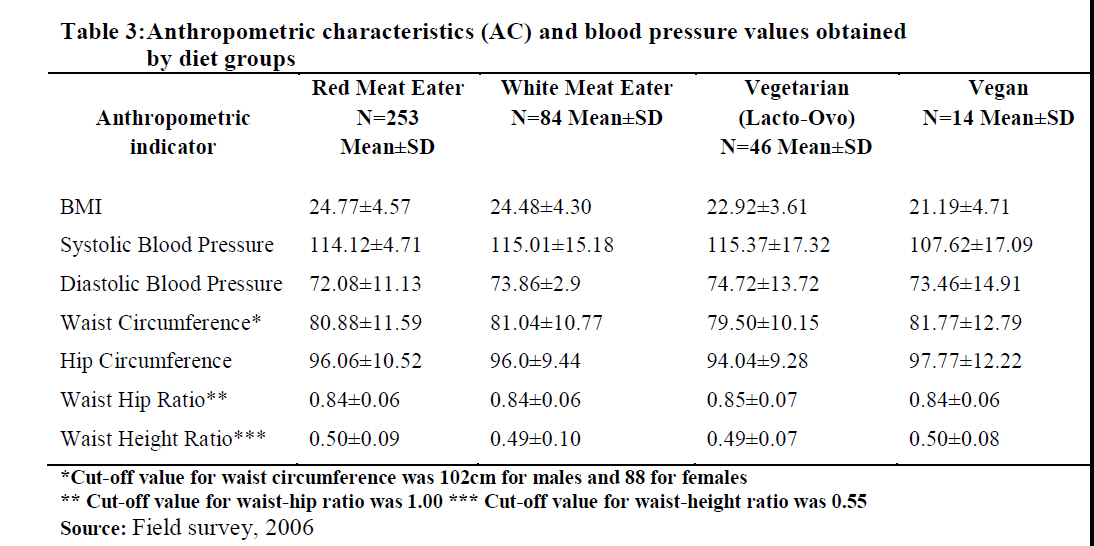
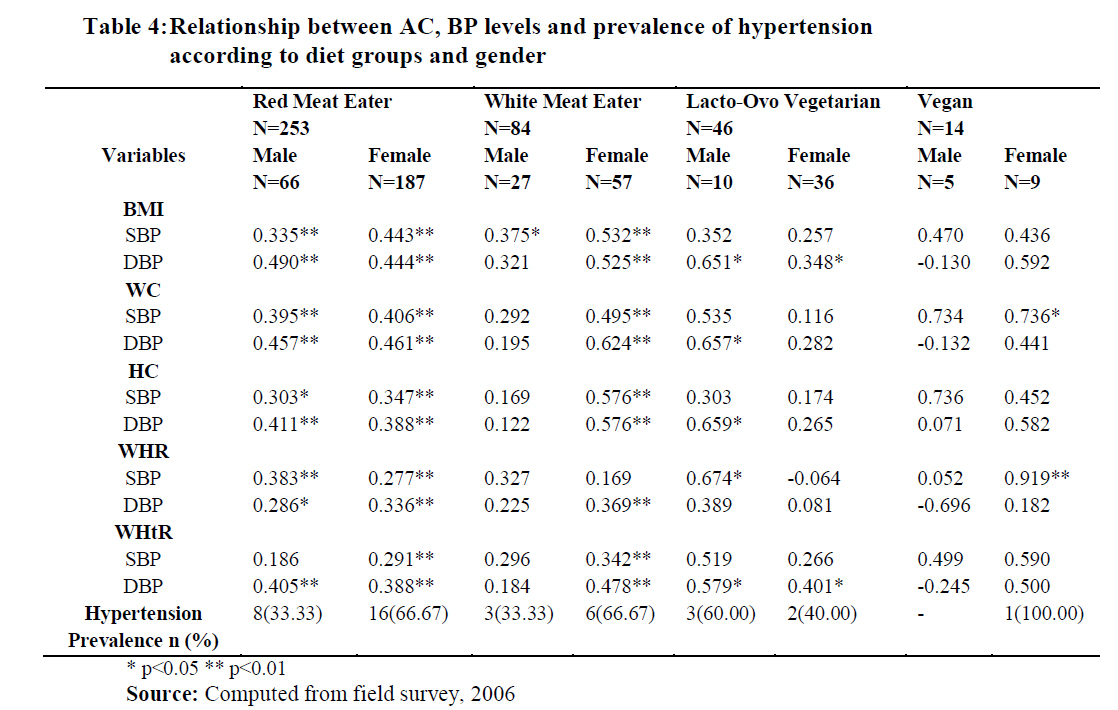
Thirteen percent (13%) of the male respondents were hypertensive while 9% of the female were hypertensive (Table 1). The percentage of those that are hypertensive among the men is slightly higher than in women. This result is consistent with past literature [20, 21]. Table 3 shows that the BMI for the majority of the respondents was less than 30 kg/m2. The BMI, however, is lowest among the Vegans (mean = 21.19kg/m2) and highest among the Read Meat Eaters (mean= 25kg/m2). Table 4 shows that significant positive correlations were observed between all the anthropometric measurements and blood pressure levels among RME and WME; however, positive correlations existed between BP levels and waist circumference (WC), hip circumference (HC), waist- hip ratio (WHR), waist height ratio (WHtR) (especially among female respondents) and BMI for both male and female respondents. Among L-O-V, positive correlations were observed between BP levels and WC, HC, WHR and WHtR among male respondents and positive correlation with BMI for both male and female respondents. In vegans, a positive correlation was observed between BP levels and WC and WHR among female respondents only. Reasons for Choice of Dietary Pattern:
Economic status, which determines ability to pay for a chosen basket of food items, and health reasons rank highest for the choice of dietary habits among the study groups (Table 5). The reason given by most RMEs for consuming that diet pattern was economic reasons; the highest percentage of L-O-V gave health reasons for their choice of diet. Blood Pressure status awareness
Many respondents were not aware of their hypertension status (Table 4). However, when assessed across the diet groups, L-O-V had highest awareness level (15%) and vegans were the least aware (7%) of BP status. Food intake by diet group
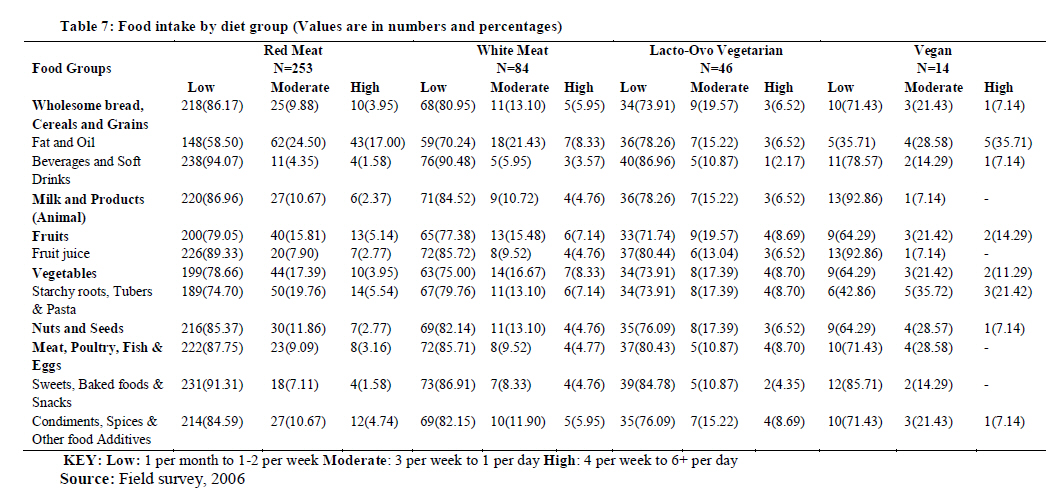
Analysis across the diet groups (using the high consumption values in Table 7) showed that whole grain were consumed more by vegans (71% consumed) and least by RME (4% consumed); animal milk and milk products were consumed more by L-O-V (78% consumed) and least by RME (2% consumed). The L-O-V were the highest consumers of fruits and vegetables (72% and 74%, respectively). The vegans were the next in rank. Meat, fish and poultry products were consumed more by RME (88% consumed). DISCUSSION
The study recorded higher ratio of women in the sample as a result of the occurrence of more women in the target population. Considering the age distribution, the majority of the respondents were part of the active labour force in the study area and anything that impairs their work output will affect Nigeria’s GDP. The study shows fair literacy level among respondents which, expectedly, should increase adoption level for innovations, reception to awareness programs and change. Respondents in the entire sample did low to mild physical activities which may be a risk factor for high BMI [4]. This, however, is not consistent with the fact that the majority of the respondents belonged to the low income category and were expected to live a vigorous lifestyle. Further studies into the occupational distribution, impact of urbanization and analysis of distance of home to work place may be relevant to shed light on this discrepancy. Economic reasons ranked highest for choice of dietary habit especially among RME, which implies that the level of disposable income played an important role in the choice of food consumed among this group. A rise in real income (expected result of development) may lead to increase in NCDs associated with diet. In this study, the higher relationship that existed between anthropometric measurements and BP levels in meat eaters (especially female) than non-meat eaters indicates that prevalence of hypertension varies with dietary pattern. Vegans comprised only a small population in this study. This observation is similar to what is obtained around the world [12]. More epidemiological studies should be carried out among Africans to assess the magnitude of hypertension prevalence in various populations. CONCLUSION AND RECOMMENDATIONS
This study has demonstrated that there is a correlation between diet pattern and CVD risk factors. Lifestyle factors, food consumption patterns and socioeconomic status were also observed to play an important role in the development of hypertension. The study also showed that a stronger relationship existed between anthropometric measurements and blood pressure levels in meat eaters (especially female) than nonmeat eaters. Thus, there is an interaction between dietary pattern and established anthropometric risk factors on blood pressure outcomes. Non-meat eaters, especially the vegans, have a lower prevalence of hypertension and lower systolic blood pressure than meat eaters (RME and WME). It was also observed that the consumption of diet rich in whole grains, fruits and vegetables (typical of the vegans’ diet) may be capable of reducing blood pressure, the major risk for CVD, even with the presence of higher BMI. This study strengthens the Dietary Approach to Stop Hypertension (DASH) (diet rich in vegetables, fruits and the use of low-fat dairy foods) as a recommended tool for lowering blood pressure in both normotensive and hypertensive individuals. The low blood pressure observed in this study may be due to increased consumption of Nigerian local fruits and vegetables which are rich in dietary fiber, potassium, magnesium and other anti-hypertensive and hypocholesterolemic effects. This, however, requires further studies. Promotion of good nutrition messages and relevant public health action, which focuses on the environmental and nutritional changes that trigger the expression of susceptibility to high blood pressure and other CVDs is strongly recommended. REFERENCES
Copyright 2011 - African Journal of Food Agriculture, Nutrition and Development The following images related to this document are available:Photo images[nd11010t3.jpg] [nd11010t1.jpg] [nd11010t4.jpg] [nd11010t7.jpg] [nd11010t6.jpg] [nd11010t5.jpg] [nd11010t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}