 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
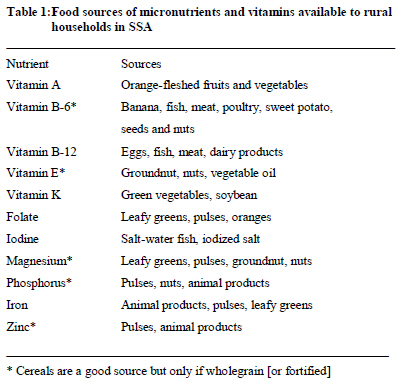
African Journal of Food, Agriculture, Nutrition and Development, Vol. 11, No. 2, 2011 pp. 4688-4707 Farming For Balanced Nutrition: An Agricultural Approach To Addressing Micronutrient Deficiency Among The Vulnerable Poor In Africa Hillocks RJ*1 1Natural Resources Institute, University of Greenwich, Chatham Maritime, Kent ME4 4TB, UK *Corresponding author email: r.j.hillocks@gre.ac.uk Code Number: nd11020 ABSTRACT Concepts on malnutrition have evolved from an emphasis on protein deficiency through energy deficit, to the realization that food quality in general and an adequate supply of micronutrients in particular, is often more of a problem than food quantity. Throughout the developing world, micronutrient deficiency is one of the most important factors influencing human health, being directly responsible for conditions such as xeropthalmia, associated with vitamin A deficiency and anaemia, due to iron deficiency. In addition, micronutrient deficiency predisposes children to infection and retards recovery from common infections such as malaria, measles and diarrhoea. The groups most at risk from micronutrient deficiency are usually children and those for whom labour for food production is limited by ill health (HIV sufferers), advanced age or intense social commitments (single mothers, for example). There have been numerous health projects in sub-Saharan Africa and elsewhere in the developing world, to address micronutrient deficiency through the distribution of vitamin and mineral supplements, which usually have to be imported. An alternative (or complementary) approach is to promote the inclusion of high quality food crops in the farming system to enrich the diet with essential vitamins and minerals. This agricultural approach to the problem of micronutrient deficiency can provide sustainable solutions, which improve diet quality. An increase in the cultivation of high quality foods such as legumes, fruits and green vegetables, may be able to deliver a balanced diet to households, without necessarily requiring additional land and labour. Agricultural approaches to enhance dietary intake of vitamins and minerals have the additional advantage that they foster community self-reliance, they are sustainable in the absence of external funding, and, offer the opportunity for enhanced income by marketing surplus production. Diet diversification through better use of existing biodiversity offers an immediate means to address poor diet quality and can also include the use of presently available nutritionally enhanced crops, such as orange-fleshed sweet potato. Key words: micronutrients, deficiency, agriculture, diet diversity INTRODUCTION Human under-nutrition may be caused by insufficient calorie intake to supply the energy required to meet daily work and social demands, insufficient protein to build body mass and/or an inadequate supply of micronutrients [1]. In some cases, where basic energy and protein requirements are met, diet quality may remain poor due to deficiencies of vitamins and minerals [2]. Diet-related health problems have become common in developed countries due to over-consumption of meat and fats and this is now being seen in urban populations in developing countries [3,4], as well as among the rural poor [5]. However, consumption of meat and dairy products is limited among the rural poor, who depend heavily on starchy staples. The linking factor between all three groups (rural poor and middle class in developing countries and urban populations in developed countries) is that they do not have a sufficiently high proportion of fruits and non-starchy vegetables in their diet. These foods are high in trace elements and vitamins and insufficient dietary intake of these, leads to symptoms of micronutrient deficiency, such as slow growth in children, anaemia and poor eyesight. Over-reliance on cereal crops low in iron, zinc and vitamin A, is the cause of widespread deficiency of these micronutrients in rural populations in developing countries. High levels of micronutrient deficiency were found in the general population in Malawi; vitamin B12 (84% of population surveyed), vitamin A (65%), zinc (53%), iron (46%), folate (37%), vitamin C (33%) and riboflavin (32%). However, the high prevalence of micronutrient deficiency in Malawi is not necessarily associated with poverty, where it was found that the consumption of fruit and vegetables declines as income increases, while consumption of meat and starchy foods increases [6]. There have been numerous health projects in sub-Saharan Africa (SSA) and elsewhere in the developing world, to address micronutrient deficiency from a medical perspective [7]. These programmes involve the prescription and distribution of vitamin and mineral supplements, which usually have to be imported. An alternative (or complementary) approach is to promote the inclusion of high quality food crops in the farming system to enrich the diet with essential vitamins and minerals [8, 9]. Agricultural solutions to the problem of micronutrient deficiencies have the additional advantage that they foster community self-reliance, they are sustainable in the absence of external funding, and, offer the opportunity for enhanced income by marketing surplus production. The Consultative Group for International Agricultural Research (CGIAR) addresses micronutrient deficiency primarily through crop fortification by breeding and genetic transformation [10]. While this approach is making an important contribution to tackling micronutrient deficiencies [11], diet diversification through better use of existing biodiversity offers an immediate means to address poor diet quality and can also include the use of presently available nutritionally enhanced crops, such as orange-fleshed sweet potato [12]. MICRONUTRIENT DEFICIENCY AND INFANT HEALTH In July 2004 Kofi Annan said: ‘Africa is the only continent where child malnutrition is getting worse, rather than better’, and that ‘halving hunger in Africa by 2015, under global anti-poverty goals seems a far-off fantasy’ [13]. More than 840 million people in the world have insufficient food to meet their daily energy requirements [14]. However, it is estimated that 2 billion people suffer micronutrient malnutrition [15], due to the poor food quality of their farm produce or, lack of money to buy high quality foods, such as fresh meat, vegetables and fruit. Globally, the most widespread micronutrient deficiencies are vitamin A, iron, zinc and iodine. Vitamin A deficiency affects an estimated 127 million children [16]. Women and children in sub-Saharan Africa (SSA) are particularly at risk of disease, premature death and impaired cognitive ability. Malnutrition is a significant factor in 50% of deaths of young children in SSA [17-19]. Diets poor in crucial nutrients result in a weakened immune system and impaired capacity to recover from the effects of diseases, which are not normally life-threatening for well nourished children; these diseases include diarrhoea, measles, respiratory infections and malaria [20,21]. Diarrhoea kills more children around the world [1.9 million] than malaria, HIV and TB combined and is the second leading cause of death in children under five, after pneumonia. High incidences of diarrhoea occur in populations that are usually also malnourished. Children suffering from malnutrition are unable to recover from the debilitating effects of diarrhoea and other diseases [22-24]. Deficiencies in iron, vitamin A and zinc, rank among the top ten leading causes of death through disease in developing countries [4]. Malnutrition contributes to mortality through its interaction with disease. Diseases such as cholera, typhoid and malaria are aggravated by, or even precipitated by, deficiencies in key micronutrients [25, 26]. A lack of vitamin A, in addition to its contribution to impaired eye sight, has been linked to measles mortality [27] and micronutrient deficiency is the underlying cause of a substantial proportion of deaths due to malaria around the world [28]. The United Nations Children’s Fund (UNICEF) estimates that eradication of Vitamin A deficiency alone would decrease child deaths from malaria by 50% in non-crisis situations [26]. Zinc deficiency affects 5.8 billion people worldwide and has been shown to increase the risk of diarrhoea in young children by 33%, pneumonia by 69% and malaria by 56% [29]. Iron deficiency anaemia is responsible for 20% of neonatal mortality and 10% of maternal mortality, or about 800,000 deaths, representing 2.4% of annual global deaths from disease [17]. The importance of dietary zinc is being increasingly recognised and it is estimated that 1.9% of the global death-toll from disease, is due to zinc deficiency. Trials with zinc supplements have shown improvements in child growth, and lower rates of diarrhoea, malaria and pneumonia [17]. A survey in Malawi revealed that 34% of all deaths of children under five are associated with malnutrition [30]. Forty-eight percent of children between birth and 59 months were chronically malnourished, manifested as below expected height for age. This is the second highest of twenty sub-Saharan African countries included in the survey. Stunting is a good indicator of the nutritional status of a population because it is not affected by short-term factors such as epidemic illness and periodic acute food shortage. Only 6% of mothers screened in the Malawian survey reported experiencing night-blindness during pregnancy and this low figure probably reflects the fact that more than 40% of the recently pregnant mothers received vitamin A supplements. However, the same survey found that 74% of children aged 6 – 59 months and 42% of mothers were anaemic, even though 80% of mothers had taken iron supplements during part or all of their pregnancy. DIET AND HIV/AIDS HIV/AIDS is a recognised threat to community food and nutrition security. HIV increases the severity of food insecurity and creates food insecurity among previously food secure households [4]. Food consumption may drop as a result of illness and falling labour productivity of household members. In Tanzania food consumption was found to decrease by an average of 15%, following the death of an adult in the poorest households [31]. With fewer people to work the land, households farm smaller plots and resort to less labour-intensive crops, such as cassava, which often have a lower nutritional value [32]. A study in Zimbabwe found that after the death from AIDS of a working-age adult in the household, crop production fell by 37 – 61%, depending on the crop [33]. In Ethiopia, the number of hours worked on farming activities per household, fell from 34 to 11 – 16 hours per week, when the household was affected by HIV/AIDS [34]. Several studies have shown that HIV damages farming systems, causing significant decreases in land use, a decline in livestock keeping, resulting in declining crop yields and a reduction in the range of crops grown which in turn, can result in poor diet, lower income, and loss of soil fertility. Support from agricultural extension and introduction of new technologies, can help to maintain agricultural productivity in the face of declining labour [32]. HIGH QUALITY FOODS Allen [35] described the evolution of concepts on malnutrition, from an emphasis on protein deficiency through energy deficit, to the realization that food quality in general and adequate supply of micronutrients in particular, is more of a problem than food quantity. Cultivation of high quality food crops can improve the diet, as well as offering new livelihood opportunities for all households in rural communities in Africa. It is particularly beneficial for expectant and nursing mothers, infants and HIV patients, who are most at risk for micronutrient deficiency [8]. High quality food crops are so named because they contain higher amounts of essential vitamins and minerals than the same weight of common starch staples, such as maize, rice, sorghum and cassava. Diet quality can be much improved by the consumption of foods derived from these crops, so that the total daily intake (weight) of food per person can be decreased. This in turn, means that less land and labour is required to provide an adequate and balanced diet for an individual or household, than would be required if they were relying only on common staples. Cultivation of high quality food crops, therefore, offers a strategy for disadvantaged groups such as HIV sufferers [36], the elderly and female-headed households to obtain a balanced diet, with less expenditure of time and energy in labour related to food production. It must be recognised that fruit and vegetables contain a lot of water and, therefore, horticultural crops require more land per food-energy calorie, than do the starch staple crops. However, diets of the poor in sub-Saharan Africa (SSA) are not always short of calories but are often deficient in key micronutrients and vitamins. This has several effects [7]:
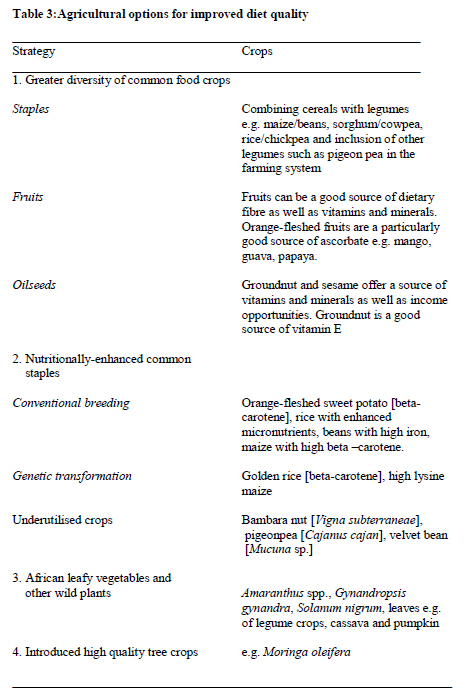
Despite acceptance by the international community that diet quality is as important as diet quantity, micronutrient deficiency is becoming an increasing problem. Little attention has been given to agricultural solutions through diet diversification, due partly, to the different ministries responsible for the work of agriculturalists and that of human health and nutrition professionals, with the consequent difficulty of co-ordination [37]. With reference to Malawi, a study by the International Food Policy Research Institute (IFPRI) [6] concluded that policies, which reduce maize prices, can decrease calorie and mineral deficiency but tend to increase vitamin deficiency by increasing the proportion of diet derived from maize. Therefore, policies which decrease food prices must be accompanied by programmes that encourage diet diversity. Current programmes aimed at preventing or treating malnutrition, depend on expensive imported foods and diet supplements, which would be out of the reach of poor beneficiaries if offered commercially. Two important international meetings in 1992 (International Conference on Nutrition and the colloquium ‘Frontiers of Nutrition and Food Security ’ organised by the Smithsonian Institute and the International Life Sciences Institute of North America) outlined a new approach to addressing malnutrition, which places more emphasis on food quality and addressing micronutrient deficiency, rather than addressing only energy and protein deficiency. More than 15 years after those meetings, there are few programmes that link health and agricultural research to provide the technical support required to address micronutrient deficiency through farm (and/or home-garden) diversification. DIET DIVERSITY Diet diversity is defined as the number of different food groups or food items consumed over a given period and this correlates well, in developed countries, with nutrient adequacy [39]. A study by IFPRI highlights the influence of low diet diversity in micronutrient malnutrition and found that out of 12 countries in sub-Saharan Africa [SSA] which were surveyed, diet diversity was worst in Mozambique (65% of households were assessed as having low diet diversity), followed by Uganda, Malawi and Rwanda (all around 50%), whereas the mean figure for Tanzania was less than 10%. Furthermore, the report noted that female-headed households are likely to be particularly vulnerable to poor quality diet [12]. While vitamin and mineral supplementation programmes can have an immediate impact on micronutrient deficiencies [6], they need to be complemented by a more sustainable approach of improving diet quality. The provision of adequate quantities of zinc and other important micronutrients and vitamins can be addressed by teaching households how to include crops in their farming systems and home gardens, that will improve the quality of their diets. Previous experience has shown, however, that nutrition education alone is insufficient to significantly improve the diets of pregnant and nursing mothers [40], without giving them the means to effect change. The message about improved diet, therefore, needs to be backed-up by improved access to seed of high quality foods and technical support on how to diversify their farming systems. AGRICULTURAL SOLUTIONS TO IMPROVE DIET DIVERSITY The ‘World Declaration’ and the ‘Plan of Action on Nutrition’, adopted by 59 countries during an International Conference held in Rome in 1992, recognised the urgent need to find sustainable solutions to micronutrient malnutrition. The conference called for sustainable food-based strategies to be given first priority in agricultural policies and that meeting the challenge of micronutrient deficiencies, required additional investment in agricultural research [41]. The declaration also states that strategies to combat micronutrient malnutrition should ensure that priority is given to locally available foods, taking into account, local food habits. At the ‘Frontiers of Nutrition and Food Security ’ colloquium, it was noted that: ‘Food, nutrition and health programmes should not exist as vertical programmes within the Health Ministry, nor should agricultural programmes be solely production-oriented. Health, nutrition and food security are inextricably interrelated and must become explicit objectives of development policy, particularly agricultural policy’ [42]. In the year 2000, the Food and Nutrition Bulletin published a special issue containing papers presented at an international conference organised by the Consultative Group for International Agricultural Research (CGIAR) on: Improving Human Nutrition through Agricultural Research. In the opening paper, the Director General of IFPRI wrote: ‘There has been little dialogue between agricultural scientists and human nutritionists to explore ways to solve the problem of malnutrition in developing countries. Little attention has been paid by human nutritionists to agriculture as a complementary means of solving the dietary quality problem’ [38]. At the same conference, Underwood [9] said: ‘Increased investment in agriculture for quantitative and qualitative improvement of the nutrition of populations is crucial to accelerating global economic growth and national development. The spin-off for the health and quality of life for millions of individuals and communities now trapped in poverty and deprivation is obvious. It is fundamental to achieving the increasingly recognised human right to adequate food and nutrition’. Welch and Graham [41] spoke of a ‘new paradigm for agriculture – the food systems paradigm; an agriculture that aims not only for productivity and sustainability but also for better nutrition’. The Asian Vegetable Research & Development Centre (AVRDC) also supports the view that the dietary approach, rather than the medicinal [supplement pills] approach, is the most economical and sustainable way to correct micronutrient deficiency [43]. Enhanced agrobiodiversity has also been advocated as a sustainable approach to improved nutrition for those suffering from HIV [44]. Although diet diversification has been recommended as the best strategy to combat micronutrient deficiency [45], there are few examples in the developing world where this has been backed by changes in agricultural policy, resulting in practical research and development programmes. Agro-biodiversity could be more effectively utilized to improve diets and nutrition, according to IFPRI [15]. Agrobiodiversity used and conserved in a livelihood context can directly contribute to nutrition, health and income generation. At the Nutrition Stakeholders Workshop held at the International Policy Research Institute (now Bioversity International) in Rome in 2006, current activities and future requirements were summarised and methods outlined for mainstreaming biodiversity and nutrition in agricultural research and development programmes and in agricultural development policy [46]. Nevertheless, agrobiodiversity remains an under-explored avenue for improving nutrition. A considerable international effort is being made to use conventional breeding and biotechnology to develop varieties of staple crops with enhanced nutrient status (biofortification) [10, 47]. Vitamin A enhanced sweet potato has been one of the more successful bio-fortified crops developed through conventional breeding [12] and has been shown to improve the vitamin A status of children in South Africa [48]. The CGIAR developed the ‘HarvestPlus’ initiative to use biofortification to reduce the effects of micronutrient malnutrition by breeding staple crops (beans, cassava, maize, rice, sweet potato and wheat) with enhanced micronutrients (especially vitamin A, iron and zinc) [49]. ‘Golden rice’ has been genetically modified for enhanced beta-carotene [50] and may become commercially available in some Asian countries in the near future [51,52]. Beans (Phaseolus vulgaris) and pearl millet have been fortified with iron and wheat and rice with zinc [11]. Cassava varieties have been selected for higher content of zinc in the roots [53]. Quantitative trait loci associated with improved bio-availability of iron have been identified for use in marker-assisted selection in maize [11]. A strong case has been made for agricultural approaches to address micronutrient malnutrition through biofortification [11, 54]. There is adequate variability in the germplasm of most staple crops to allow selection for higher nutrient content by conventional breeding and the traits tend to be stable across environments [10]. Fortified varieties of common staples produced by conventional breeding would provide an inexpensive and accessible approach to improve diet quality [55]. The impact of biofortified varieties on the micronutrient health of populations depends on their widespread utilization. Fortification achieved through genetic modification meets the additional obstacles of public and market acceptance of genetically modified foods and the requirement for proper risk assessment and biosafety regulation [56]. However, there are problems associated with the distribution and adoption of introduced varieties, especially if there is no immediate commercial advantage to the farmer. Combinations of food crops already available can provide the required vitamins and minerals (Table 1), when consumed in combination with the starch staples. Leafy greens [14, 57, 58] for instance, provide fibre, minerals and vitamins and are an excellent supplement to the starch staples which are low in micronutrients (Table 2). Underutilised indigenous crops such as bambara nut [59] and introduced crops such as the Moringa tree [60] can also contribute to a balanced diet. Encouraging more widespread cultivation of nutrient-rich indigenous and introduced crops does, however, meet similar obstacles to adoption, as does the introduction of new varieties from international and national biofortification breeding programmes. Home gardens can make a significant contribution to diet diversity and alleviation of micronutrient deficiency. The homestead food production (HFP) programme was introduced in Bangladesh by the Helen Keller International, over 20 years ago, with the original objective of combating vitamin A deficiency through a programme of education and vegetable gardening. It has expanded into a nation-wide programme which increases the availability of nutrient-rich foods for millions of households, while also contributing to household income and community development [1]. The HFP programme has been highly successful at improving diet quality and the model has been adopted in other parts of the world, including some African countries but on a much smaller scale. Impact studies showed that the HFP programme led to an increase in the number of mothers and children consuming adequate amounts of leafy greens and animal products to meet their micronutrient needs but no comparison was made of the incidences of deficiency in target communities, before and after the programme. The emphasis in this review is on the contribution to diet diversity of increased crop biodiversity but the importance of food products of animal origin, should not be overlooked [61,62]. In addition to the contribution they make to household nutrition, livestock also provide manure for sustainable approaches to soil fertility. In SSA, the inclusion of animals in the farming system may not always be possible, whereas crop production is universal in all but the driest areas. Disease, small land holdings and the economics of providing feedstuffs and access to veterinary services, are the main factors that prevent smallholders from keeping animals. Goat keeping is often more accessible to poorer households than cattle-keeping and much more could be done to develop markets for goat meat, which would provide the incentive for smallholders to invest in improved breeds and animal husbandry [63]. Most rural households in Africa keep chickens, so that eggs and poultry meat can also make a valuable contribution to a balanced diet [64]. OPTIONS FOR INCREASING DIET DIVERSITY There are four crop-based options available to improve the diversity and food-quality of homestead produce (Table 3), which can be integrated into a single strategy:
Successful outcomes from a programme based on diet diversity would depend on establishing good working relationships between the National Agricultural Research Systems (NARS), health and nutrition services, education services and local communities. Horticultural R & D agencies should link to community-based health programmes to develop and promote accessible vegetables and fruit trees, which can increase the diversity of foods produced from household gardens. Capacity-building of research and extension organizations is necessary to ensure the sustainability of interventions, once project support is removed. The necessary awareness of diet-related health issues would be developed through linking the programme to the education of children at schools and to adults through community groups. The challenge is in bringing together and coordinating stakeholders in at least three Ministries; Agriculture, Health and Education. Advocates of the biofortification approach to improved nutrition, suggest that diet diversification is a more expensive approach and difficult to sustain on a large scale because of the need to integrate agricultural interventions with health and education [65]. However, this can be done if the right institutional linkages are established from the outset. For instance, a home-gardening programme in South Africa was integrated with primary health care to successfully increase serum retinol concentrations in children through increased consumption of yellow and dark green leafy vegetables [58]. The sustainability of diet-diversity as a solution to micronutrient deficiency requires that seed of ‘new’ crops are made available and national agricultural and horticultural services need to be engaged to provide the starting materials and technical support. Then, future seed availability will depend upon community seed exchange which will require the support of community leaders, NGOs and the organisation of regular ‘seed fairs’ instigated by village extension officers and community leaders. In order to make recommendations which do not involve additional labour and which are accessible to the disadvantaged, interventions should be focused on making the farm and/or household garden, more productive in terms of food quality, not necessarily in the quantity of food produced [1]. If the crop combinations being promoted to expand diet diversity include those with commercial potential, market opportunities for surplus production, provide the incentive for adoption of high quality crops by the wider community. REFERENCES
The following images related to this document are available:Photo images[nd11020t1.jpg] [nd11020t3.jpg] [nd11020t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}