 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
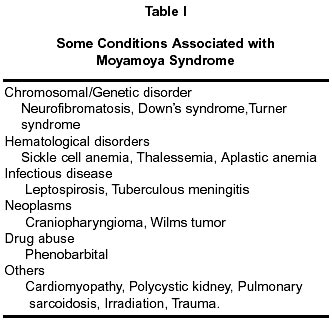
Neurology India, Vol. 50, No. 1, March, 2002, pp. 6-10 REVIEW ARTICLE Moyamoya Disease : A Review J.A. Gosalakkal Department of Pediatric Neurology, NYU School of Medicine, New
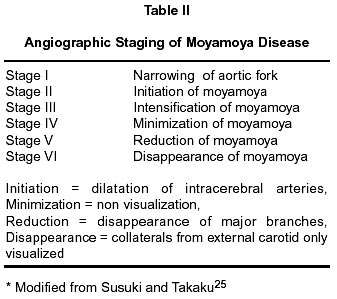
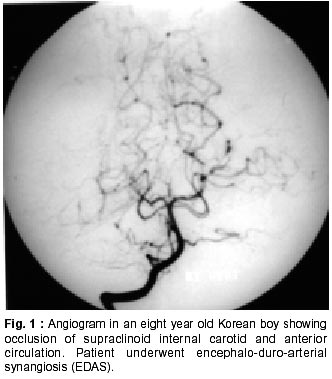
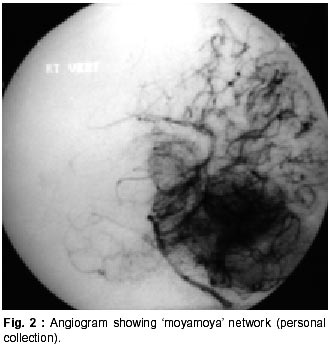
York - 10016, USA. Accepted for publication : 2nd August 2001. Code Number: ni02004 Summary Moyamoya is probably an inherited vasocclusive disease first described in Japan and now reported from all over the world. Genetic linkage studies and study of the factors possibly involved in its pathogenesis have shed new light on this disease. There is some suggestion that the pathogenesis may vary between races. A number of revascularization procedures have been devised. There is still controversy regarding the timing and the type of surgery. Functional MRI and PET scanning may provide more objective criterion on the outcome of these procedures. Neuropsychological studies may also be of use in judging the benefits of surgery. In this review, some of the recent advances in the study of the genetics and pathogenesis of the disease are reviewed and the clinical manifestation and the role of surgery are discussed. Relative lack of literature from outside Japan and the Korean peninsula has hampered the understanding of the disease in other countries. Key words : Vaso-occlusive disease, Moyamoya, Revascularization. Takaku, Suzuki and others described moyamoya disease in Japan in the sixties.1 The term means a 'wavering puff of smoke' and was used to describe the abnormal vasculature at the base of the brain. Moyamoya disease is a cerebrovascular disease that features narrowing or stenosis, starting at the distal internal carotid and proximal portions of the anterior and middle cerebral arteries. Moyamoya syndrome is a phenomenon caused by an olegemic state similar in presentation but caused by various disease entities (Table I). Once believed to be restricted to Japan, there have now been reports from all over the world, especially China and Korea.2-4 Moyamoya is an intriguing disease and little is known about its pathogenesis. Most patients present with the symptoms of cerebral ischemia and a few, especially adults, present with cerebral hemorrhage. Etiology Etiology of the disease is still unknown. A genetic mode of inheritance is considered possible because of the higher incidence of the disease in Japan and Korea and the familial occurrence among the Japanese as well as in Caucasians.5 There have been recent reports of increased familial incidence of the disease. This apparent increase may partly reflect the fact that wide spread use of magnetic resonance imaging (MRI) and magnetic resonance angiography have been detecting the disease in asymptomatic patients. In a recent total genome search, a linkage was found between the disease and markers located at 3p24.2-26.6 Another linkage study using markers on chromosome 6, where the HLA gene is located, showed a possible linkage of the marker D6S441 to the disease.7 DNA typing of HLA also indicates that the disease is probably genetic in origin. There have also been reports of linkage to chromosome 17. Factors involved in pathogenesis A number of factors have been postulated as playing a role in the pathogenesis of moyamoya disease. Fibroblast growth factor has been proposed as a possible mediator of the neovascular response. There is some evidence to show that CSF bFGF may play a role in the pathogenesis of the disease.8 Transforming growth beta factor 1 (TGF beta 1), a factor involved in angiogenesis and expression of connective tissue genes, was also shown to be elevated in the disease. An unknown CSF protein has been detected in some patients with moyamoya. Further analysis of this protein may reveal a clue by which the molecular mechanism of moyamoya disease may be elucidated.9 The role of prostaglandin in the pathogenesis of the disease has been studied. These studies have shown that the arterial smooth muscle cells in moyamoya activate cox2 in response to inflammation, and produce excess PGE.2 This can cause an increase in vascular permeability and decrease the tone, which may promote intimal thickening.10 A possible role for infection in the pathogenesis has been proposed. The evidence is still inconclusive but some studies have suggested a relationship with Epstein-Barr virus infection. This was based on the increased presence of EBV DNA and antibody in patients with moyamoya.11 Moyamoya like changes were histopathologically demonstrated in experimental rats infected with Propionobacterium acnes. The significance of this finding in humans is unknown. Clinical and angiographic criterion for moyamoya disease and syndrome Moyamoya disease has been traditionally described as having the following features. There is stenosis or occlusion observed at the terminal portions of the internal carotid artery and the proximal anterior cerebral artery, middle cerebral artery or both. Abnormal vascular moyamoya networks are observed in the vicinity of the previously mentioned areas in the arterial phase and these findings are present bilaterally. These findings have to be confirmed angiographically. Magnetic resonance angiography is being used more often, especially in children, to confirm the diagnosis. Diseases known to cause similar changes also need to be ruled out. Pathological criteria may be used instead. These are intimal thickening and occlusion or stenosis observed around the intracranial terminal portions of the internal carotid artery. In the main arteries (anterior, middle cerebral and posterior communicating arteries) of the circle of Willis, various degrees of stenosis and occlusions are observed. These vessels show intimal fibrous thickening, widening of the internal elastic lamina and thinning of the media. Many tiny vascular channels are observed around the circle of Willis and small vessels of conglomerated networks are observed in the pia mater. 'Definite moyamoya' fulfils the criteria entirely and the term 'probable moyamoya' is used to describe unilateral cases. The term moyamoya syndrome is used when similar findings are associated with a basic disease (Table II). Recently the terminology has been questioned and it has been proposed that the term moyamoya syndrome should be dropped and be replaced with 'a systemic disease with angiographic moyamoya'. The confusion in terminology is likely to persist till the etiology of idiopathic moyamoya is fully established.12 Cerebral blood flow and metabolism in moyamoya The morbidity of moyamoya is directly related to cerebral blood flow. This was demonstrated in earlier studies using Xenon-133 inhalation. The cerebral blood flow was decreased most in the frontal region with relatively normal flow in the temporal and occipital region. After hyperventilation the blood flow was reduced in all regions. Positron emission tomographic studies have shown an increase in total blood volume, especially in the striatum and increased transit time. The cerebrovascular response to hypercapnia was shown to be impaired. These changes were reversed after reperfusion surgery.13 PET studies have also demonstrated the vasodilatation in normal areas after the termination of hyperventilation. This may cause a steal response increasing hypoperfusion. These studies may help to understand the effects of chronic cerebral occlusive disease. Xenon computed tomography has been used for pre and post surgical evaluation. These studies were found to correlate with angiographic studies and have been claimed to be superior in the study of basal ganglia and posterior circulation.14 Diffusion weighted imaging and perfusion magnetic resonance imagine using contrast have been used in the study of ischemic episodes. Serial studies have also shown the decrease in cerebral blood flow with advancing age.15 Clinical features Moyamoya disease has the highest incidence during the first decade of life. Children present most frequently with transient ischemic attacks or ischemic strokes. Cerebral ischemia may also present as reversible ischemic neurological deficit, sensory attacks or acute infantile hemiplegia. Headaches, involuntary choreiform movements, seizures and other motor disturbances have been described. Motor disturbances are the most common mode of presentation occurring in 80.5% of the population. Convulsions occur in about 9%. Episodic symptoms are often precipitated by hyperventilation or rise in body temperature. Moyamoya and intelligence quotient : There have been a number of reports suggesting a decline in the IQ of children with symptomatic moyamoya. This is one of the reasons often quoted for advocating early surgery. These scores were said to depend on the duration of symptoms and tend to stabilize after ten years. Some studies have shown an improvement in IQ after surgery.16 Endocrine dysfunction : There have been a few case reports of hypothalamic-pituitary dysfunction associated with moyamoya. Patients have presented with evidence of pituitary and thyroid hypofunction. It has been suggested that children with moyamoya be closely monitored for hypothalamic-pituitary dysfunction.17 Hemorrhagic type moyamoya disease : Intracranial hemorrhage is more common in adults with the disease but can manifest in children. Factors, which may contribute to bleeding include hypertension and aneurysms. There seems to be an apparent racial difference with a statistically higher incidence of hemorrhage in Korean children compared to Japanese children. There is also a higher incidence in females. In one study hematoma at the basal ganglia was noted in 40% of cases, intraventricular hemorrhage (IVH) in 30%, thalamic hemorrhage with ventricular rupture in 15% and subcortical hemorrhage in 5%.18 Rebleeding can occur a long time after the first episode. The hemisphere in which it occurs and the type of bleeding is often unpredictable and hence the difficulty in preventing rebleeds. Blood pressure control may help prevent rebleeds. Mortality increases after rebleeds and generally the prognosis is worse after each rebleed. Angiographic features of moyamoya There is narrowing and occlusion of the supraclinoid portions of the internal carotid artery and the proximal portions of the anterior and middle cerebral artery (Fig. 1) The development of the moyamoya network may be seen at different sites (Fig 2). The formation of network of vessels at the frontal base with blood supply from the branches of the ophthalmic artery is known as ethmoidal moyamoya. Dilatation of the basilar artery and formation of moyamoya network by perforating branches of the posterior cerebral artery is known as posterior basal moyamoya. Vault moyamoya is due to development of extra and intracranial transdural leptomeningeal collaterals between pial vessel and branches of the external carotid artery. A well-developed posterior callosal artery is seen. The large and proliferating irregular vessels and transdiploic collaterals of the external carotid artery that supplies the ischemic regions of the brain essentially cause the moyamoya network. Angiographic staging has been used with intensification of the moyamoya in the early stages and disappearance in the late stages (Table II). The angiographic stage does not directly correlate with the distinct clinical presentations between pediatric and adult moyamoya disease.19 Imaging Computed tomography may be useful for detetecting hemorrhage. Low density areas may suggest infarction. There may be evidence of cerebral atrophy. Grey and white matter of the frontal lobe is most frequently affected. Magnetic resonance imaging It has been used extensively in Japan for screening purposes. Moyamoya vessels are visualized as multiple small round or tortuous low intensity areas extending from the suprasellar cisterns to the basal ganglia. Occlusive changes in the distal internal carotid, anterior cerebral artery and middle cerebral artery and ischemic cerebral lesions and collaterals can also be visualized. Proton magnetic resonance spectroscopy (MRS) is an effective method to noninvasively investigate cerebral metabolism. Electroencephalographic changes EEG changes reported in moyamoya include posterior slowing and centrotemporal slow activity. There is sleep spindle depression. A 'rebuilt up' phenomenon after cessation of hyperventilation has been reported. This rebuilt up corresponds to increase in cerebral blood flow in angiography. EEG has sometimes been used in the past for screening but has generally been replaced by magnetic resonance imaging. Surgery for moyamoya :When and what ? There is evidence to show that surgery is beneficial in reducing ischemic symptoms and improving neurological outcome. Many believe that the outcome is better with surgery as compared with the natural history of the disease or the results of medical treatment.20,21 There is however no controlled series to establish this point and success of the treatment is often based on perfusion studies and the patient's history. Parameters like intelligence quotient and daily living activity index have been used to demonstrate improvement with surgery. The results of follow-up studies have not always been unequivocal.22 The opponents of immediate surgery for all have cited surgical complications, lack of information about the natural history and lack of controlled studies for their opposition.23 Most experts would consider surgery in the symptomatic patients. Care must be taken in the administration of anesthesia and there is a definite risk of perioperative neurolgical deterioration.24 A number of procedures, each with its own proponents, have been devised to create collateralization on the brain surface. These procedures are either indirect revascularization procedures such as EDAS (encephaloduroarterio synangiosis), pial synangiosis, indirect revasularization using omental flaps etc. or direct revascularization procedures such as superficial temporal-middle cerebral artery bypass etc. Generally, indirect revascularization is preferred in treatment of children. The decision is based on angiography and cerebral blood flow studies. TlAs reduce in frequency and patients do not develop new strokes in successful cases. Medical treatment with vasodilators, corticosteroids, antiplatelet agents etc. has been tried with doubtful efficacy. Patients are often put on aspirin, even though there is no evidence that it stops or reverses arterial occlusion. Conclusion Moyamoya was initially recognized as an angiographic pattern. Attempts to classify it into a primary disease form and a secondary form associated with other diseases have led to criterion for its diagnosis being adopted. There is evidence to show linkage of moyamoya to several chromosomes and it is likely to have heterogenous loci. A role for various growth factors and proteins in its pathogenesis has been proposed and the role, if any, played by infections remains to be elucidated. Better methods for studying the cerebral blood flow and screening have been devised. A number of surgical procedures have been developed for revascularization and there is controversy regarding the timing and the surgical procedure to be used. There is some evidence to show that the pathogenesis may vary in different races. Moyamoya is an interesting disease and its study may help understand the genetics and the pathogenesis of vasoocclusive diseases in children. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02004t2.jpg] [ni02004f2.jpg] [ni02004t1.jpg] [ni02004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}